

Figure 2. MRI shows “hummingbird” and “Mickey Mouse” signs of midbrain atrophy in PSP.
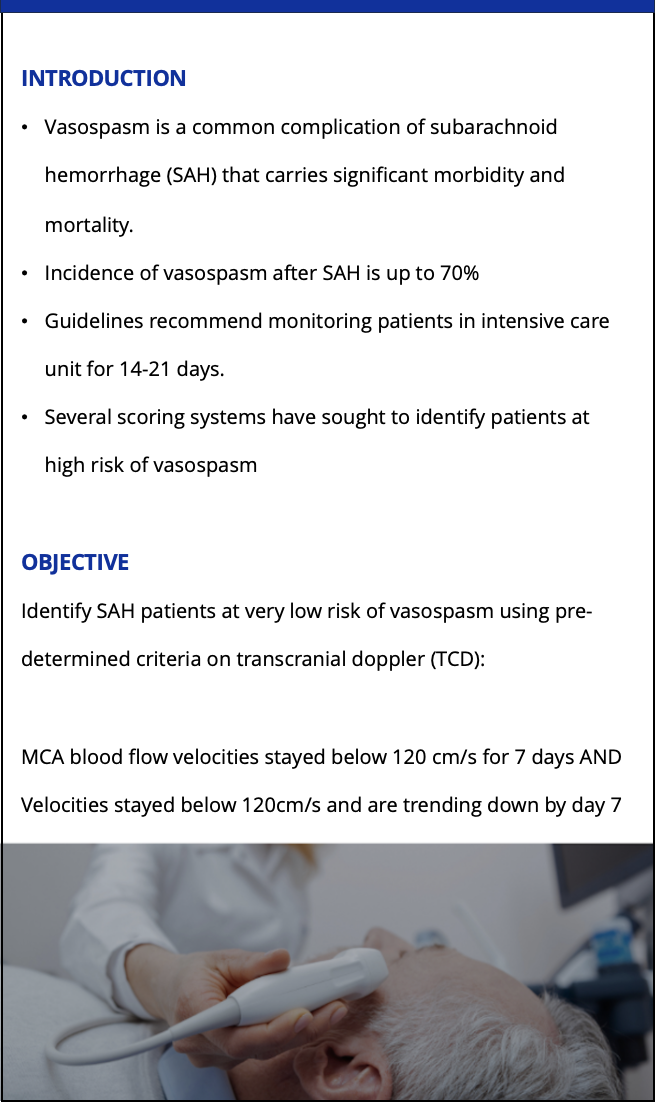
INTRODUCTION
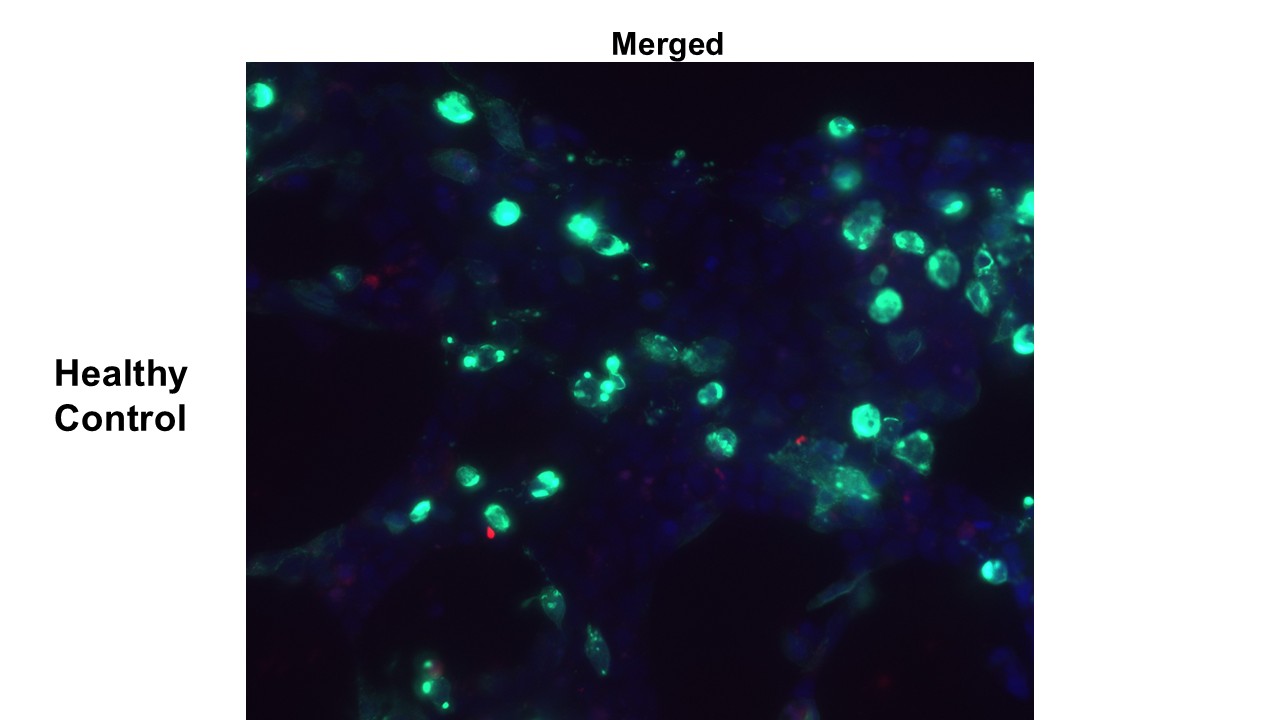
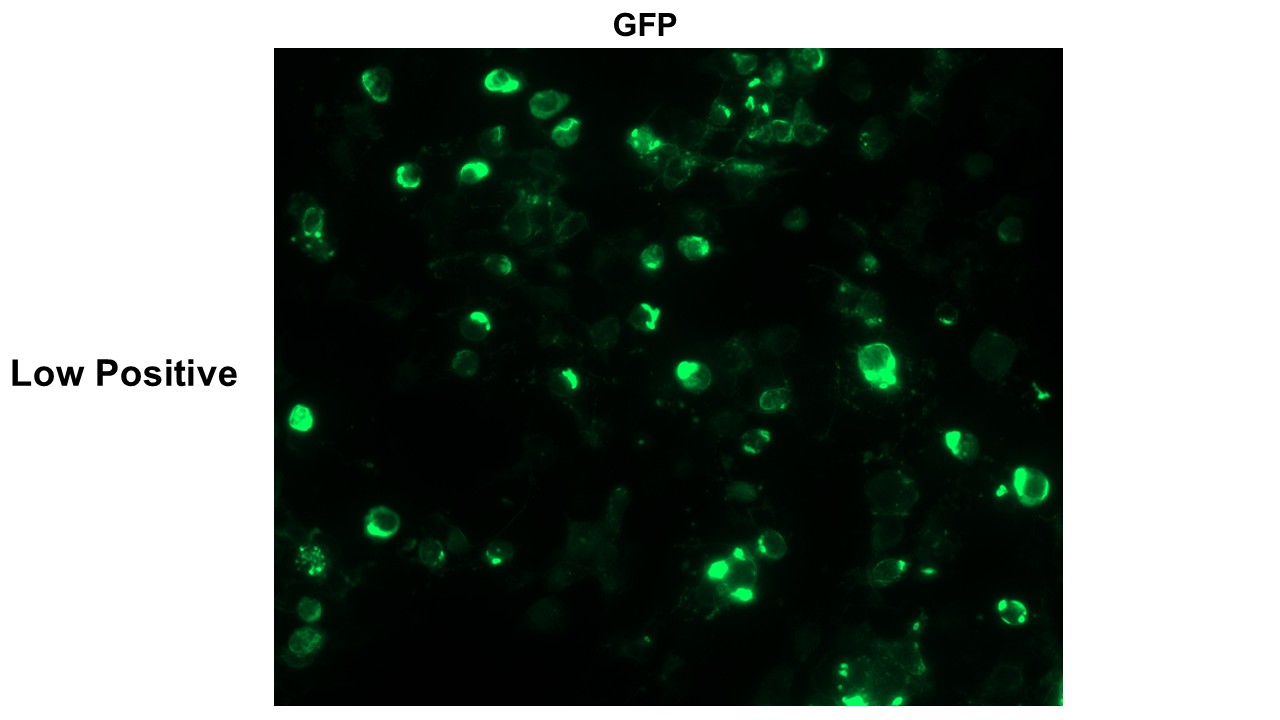
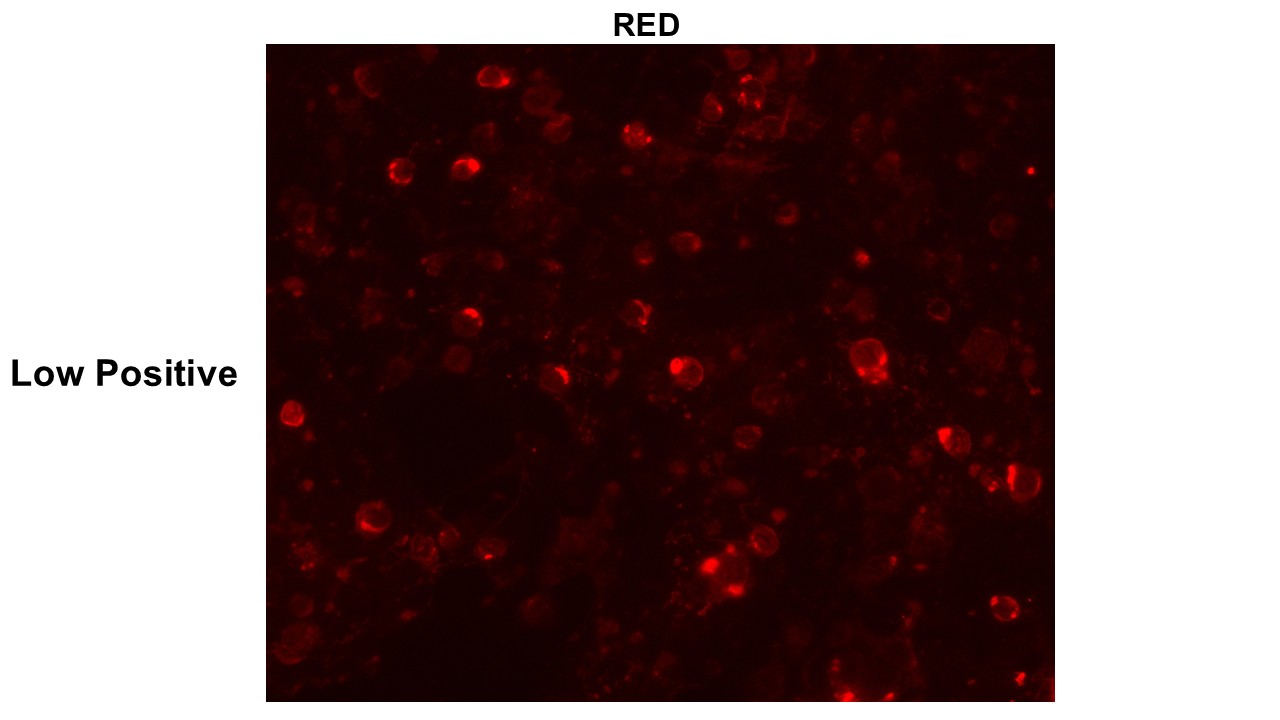
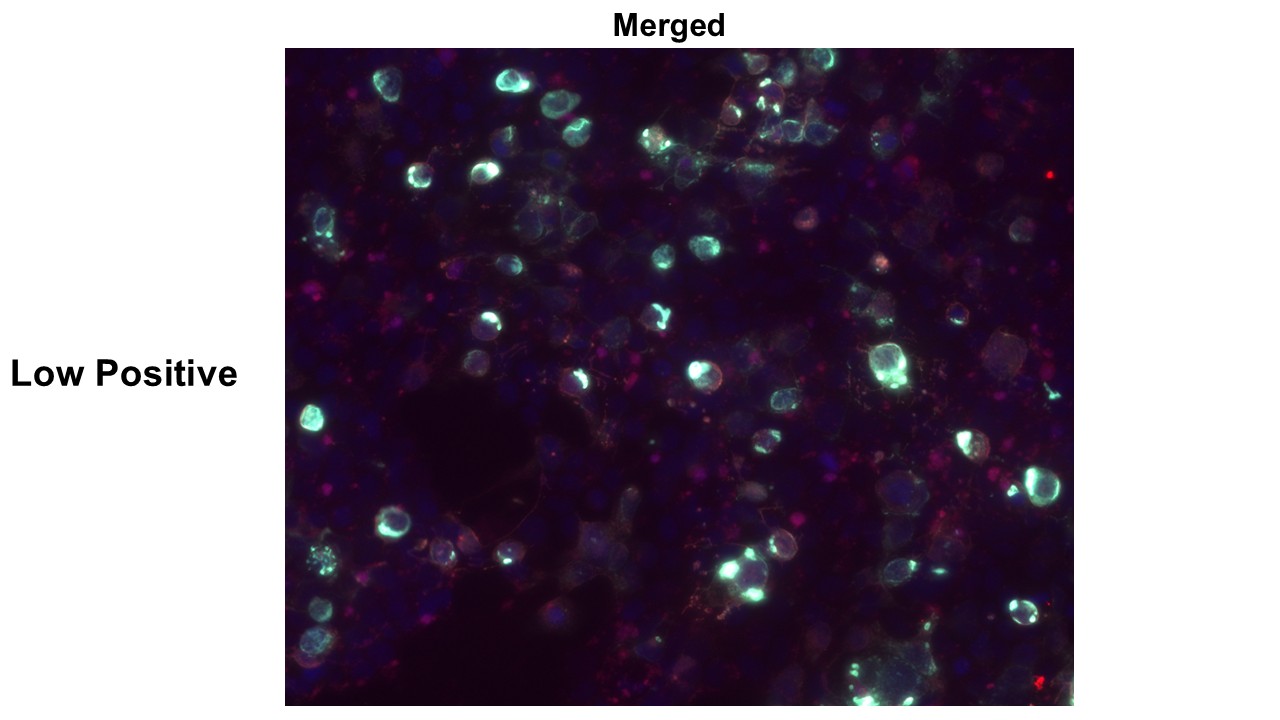
References
1. Waters PJ, Pittock SJ, Bennett JL, et al. Evaluation of aquaporin-4 antibody assays. Clin Exp Neuroimmunol. 2014; 5:290–303. DOI: 10.1111/cen3. 12107.
2. Waters PJ, Komorowski L, Woodhall M, et al. A multicenter comparison of MOG-IgG cell-based assays. Neurology. 2019;92: e1250–e1255. DOI: 10. 1212/WNL.0000000000007096.
3. Kumar P. et al, P.033 Detection of Myelin Oligodendrocyte Glycoprotein Immunoglobulin G (MOG-IgG) by live and fixed Cell-Based assays; June 2022. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques 49(s1): S16-S16 DOI: 10.1017/cjn.2022.135


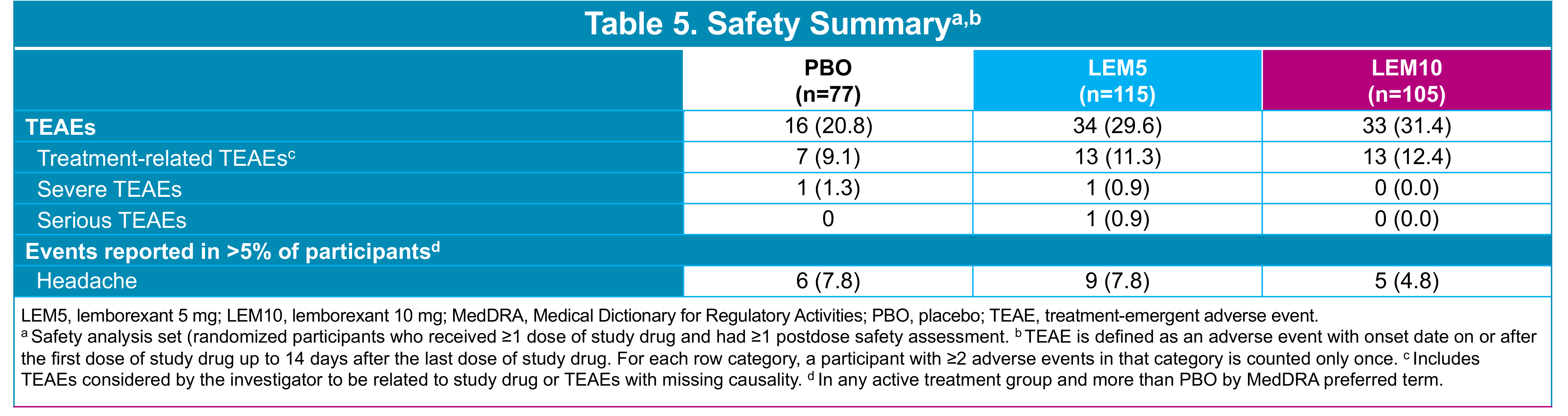
Funding for the study, analyses, and editorial support (Mayville Medical Communications) was provided by Eisai Inc.
References1. Swanson C, et al. Alzheimers Res Ther. 2021;13:80. 2. van Dyck CH, et al. N Engl J Med. 2023;388:9-21. 3. LEQEMBI™ (lecanemab-irmb) injection, for intravenous use [package insert]. Nutley, NJ: Eisai Inc. 4. Hampel H, et al. Mol Psychiatry. 2021;26(10):5481-5503. 5. Shi M, et al. Front Aging Neurosci. 2022; 14:1-11.6. Söderberg L, et al. Neurotherapeutics. 2023;20(1):195-206. 7. Kaplow JM, et al. Alzheimers Dement. 2013;9:P807-P808.
If you have any questions about this poster, please email or call Eisai Medical Information at ESI_Medinfo@eisai.com or 888-274-2378.
Alzheimer's Disease (AD) is a chronic, progressive neurodegenerative disorder that is the leading form of dementia and cause of cognitive and functional impairment.1 AD pathology is characterized by the accumulation of amyloid beta (Aβ) plaques, which precedes neurodegeneration, and cognitive decline.2,3 Early AD comprises mild cognitive impairment (MCI) due to AD and mild dementia due to AD.4 As AD progresses, cognitive decline worsens, leading to loss of independence, confusion, disorientation, mood changes, agitation, and eventually delusions or hallucinations.4-6 Beyond the impact of AD on patients, there are also significant impacts on the care partners of patients with AD.7 All aspects of daily living, such as job absenteeism, financial hardships, daily tasks, and available time, are impacted by caring for a person living with early AD.7
The current standard of care (SoC) for patients with early AD consists of non-pharmacological interventions with or without cholinesterase inhibitors (ChEIs) for symptomatic relief. However, current therapeutic options only address the symptoms of the disease and not the underlying cause; they do not halt or slow disease progression, providing only modest and temporary benefit to symptoms that is lost after treatment discontinuation.8-10
Lecanemab is a humanized IgG1 monoclonal antibody that binds to Aβ protofibrils, which in turn leads to clearance of Aβ protofibrils and plaques.11 Lecanemab was studied in the phase 3 randomized, multicenter, double-blind, placebo-controlled, parallel-group trial, Clarity AD (NCT03887455), in patients with early AD (MCI and mild dementia due to AD) with confirmed Aβ pathology.11 Lecanemab significantly slowed disease progression on CDR-SB by 27.1% at 18 months.11 Lecanemab was generally well-tolerated, with the most common adverse events (AEs) being infusion-related reactions, amyloid-related imaging abnormality-microhaemorrhage and haemosiderin deposit (ARIA-H), amyloid-related imaging abnormalities-oedema/effusion (ARIA-E), and headache. Most ARIA were asymptomatic and radiographically mild, and can be monitored by early magnetic resonance imaging (MRI).11
Model Structure: A Markov model with a one-month cycle length and lifetime horizon (30 years) was developed and used to capture the costs and outcomes associated with lecanemab + SoC and SoC alone when treating early AD (Figure 1). The model included four distinct health states based on disease severity according to Clinical Dementia Rating – Sum of Boxes (CDR-SB) (replicated in the community and institutional care settings) and death (ie., nine health states in total).
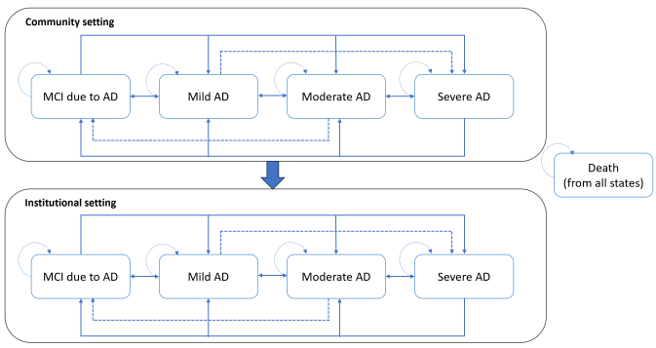
Dashed and solid lines are both used to denote possible transitions.
|
|
Lecanemab + SoC |
SoC |
Incremental |
|
Total life years (LYs) |
8.14 |
7.48 |
0.66 |
|
Total QALYs |
10.59 |
9.41 |
1.19 |
|
Incremental Costs |
$146,219 |
$68,407 |
$77,812 |
|
ICER (Cost/LY) |
$118,356 |
||
|
ICUR (Cost/QALY) |
$65,424 |
||

Recent evidence suggests that mindfulness training can support self-management for people with Mild Cognitive Impairment (MCI) (Wells et al, 2019).
Many mindfulness training programs, however, are not necessarily designed to address the specific needs of the MCI population, and sometimes even exclude persons with MCI from participating.
In 2021, the Neil and Susan Manning Cognitive Health Initiative (CHI) partnered with the BC Association for Living Mindfully (BCALM) to create a specialized mindfulness training program for MCI.
The BCALM-CHI collaboration created a specific course for persons with MCI based on Mindfulness Based Stress Reduction (MBSR), designed to develop community capacity. This was adapted from BCALMs "Art of Living Mindfully" course.
The study objectives were to:
1) Increase self-management capacity for participants with early cognitive impairment;
The Neil and Susan Manning Cognitive Health Initiative (CHI) is a partnership between the Vancouver Island Health Authority, UBC, the Universit of Victoria, and the Victoria Hospitals Foundation. Thanks to these generous and visionary donors, the Initiative is now in its 8th year.




Practical LHSC-specific care pathway
Timing and communication protocol for sample collection
Education and support for pediatricians and pathway to pediatric hematology
Paper +/- EMR prompts and nurse-led reminders, including Nurse Specialist Lead
Plan to coordinate and track any changes to baby vaccine schedules
In-person meetings that bring together all members of the healthcare team—nurses, physicians, administrators, IT professionals, quality specialists, and representatives from multiple hospitals and regions—can further enhance success through shared real-time collaboration and innovation.

Disclosures: Financial support for this project for food and transportation was provided by Roche. Courtney Casserly has received funding in the form of honoraria, consulting fees, or other compensation from: Multiple Sclerosis (MS): Biogen, Novartis, Roche, Sanofi, EMD Serono; Neuromyelitis Optica Spectrum Disorder (NMOSD): Horizon Therapeutics, Genentech/Roche, Alexion; Education funding through the Western Libraries Digital Innovation Grant & the Western Teaching Innovation Award.
This study explored whether Myelin Water Imaging could detect myelin injury in Anti-NMDA receptor autoimmune encephalitis (NMDAr-AIE), where traditional neuroimaging is often normal. Myelin Water Fraction (MWF) quantifies myelin content by distinguishing myelin sheath water from other brain water compartments.
Adult participants with confirmed NMDAr-AIE diagnoses and healthy controls (HC) underwent 3T brain MRI (Magnetic Resonance Imaging) including MWF mapping. Participants were recruited after discharge from the hospital. Mean MWF was calculated for 4 white matter regions of interest (ROI). MHI (Myelin heterogeneity Index) was calculated by dividing the MWF standard deviation by the mean MWF. Patient demographics, clinical assessments, treatment, and outcomes were collected.
Five participants with NMDAr-AIE (4F/1M, mean age 30, SD 7) and four HC (3F/1M, mean age 36, SD 6) were included. All NMDAr-AIE participants had normal or non-specific T2 hyperintensities on initial imaging and had received immunotherapy. The mean Modified Rankin Score (MRS) on discharge was 2. MWF (mean ± SD) for normal-appearing white matter, corpus callosum, corticospinal tract, and superior longitudinal fasciculus were 0.10±0.02, 0.12±0.02, 0.15±0.03, 0.12±0.02, which were very similar to HC at 0.09±0.02, 0.11±0.01, 0.15±0.02, and 0.11±0.02, respectively.
|
|
Patient 1 |
Patient 2 |
Patient 3 |
Patient 4 |
Patient 5 |
|
Age |
30 |
22 |
28 |
42 |
30 |
|
Sex |
F |
F |
M |
F |
F |
|
Treatment |
IVMP, OS, IVIG, PLEX, Rituximab |
IVMP, OS, IVIG |
IVMP, OS, PLEX, Rituximab |
IVMP, PLEX |
IVMP, OS, IVIG, PLEX, Rituximab |
|
mRS at discharge/assessment |
2/0 |
2/0 |
3/0 |
2/0 |
2/1 |
|
ICU Admission |
No |
No |
No |
No |
Yes |
|
Disposition |
Home with outpatient rehab |
Home, independent |
Home with family support |
Home with family support |
Home with outpatient rehab |
|
IVMP – Intravenous Methylprednisolone IVIG – Intravenous Immunoglobulins OS – Oral Steroids PLEX – Plasma Exchange |
|||||
|
Participants |
MWI Measure |
ROI |
|||
|
NAWM |
Corpus |
Cortical Spinal |
Superior Longitudinal Fasciculus |
||
|
Healthy Control |
Mean |
0.09±0.02 |
0.11±0.01 |
0.15±0.02 |
0.11±0.02 |
|
MHI |
0.52±0.13 |
0.36±0.08 |
0.28±0.06 |
0.30±0.06 |
|
|
AIE |
Mean |
0.10±0.02 |
0.12±0.02 |
0.15±0.03 |
0.12±0.02 |
|
MHI |
0.44±0.05 |
0.42±0.07 |
0.28±0.08 |
0.24±0.02 |
|
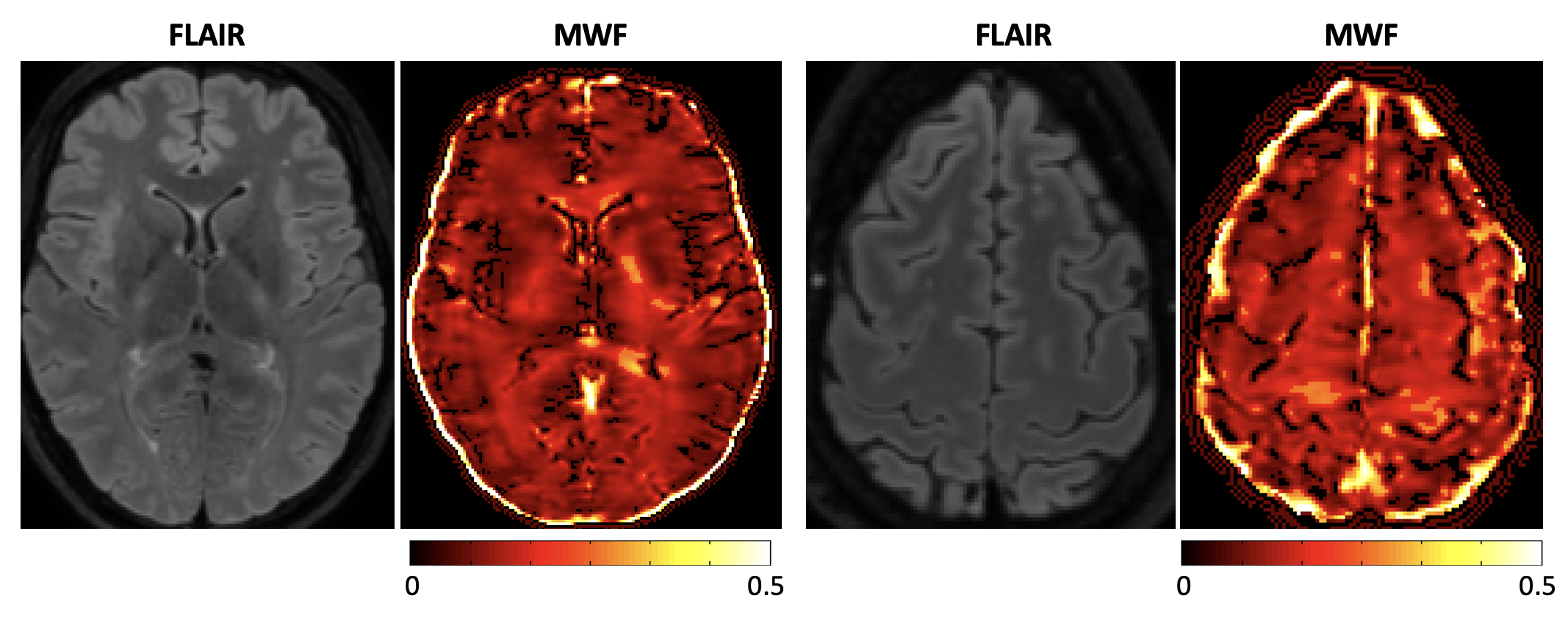
Myelin Water Imaging showed no myelin pathology in five NMDAr-AIE patients, with MWF and MHI values comparable to HC, suggesting that myelin pathways are relatively preserved post-recovery from AIE. Moving forward, we aim to continue recruiting healthy controls, patients post-recovery and those experiencing active disease to determine if there are any MWF abnormalities throughout the disease course. Future studies are needed to assess MWF changes in other antibody-mediated encephalitides.
The COVID-19 pandemic disrupted global healthcare systems, limiting access to care for individuals with chronic diseases, including people with multiple sclerosis (PwMS).
PwMS are at increased risk during pandemics due to immunosuppressive disease-modifying therapies (DMTs) and a higher baseline prevalence of psychosocial distress.
Oman, classified as a medium-risk zone for MS, had no prior data evaluating the pandemic's impact on PwMS.
Evaluate the impact of COVID-19 on MS management and disease progression.
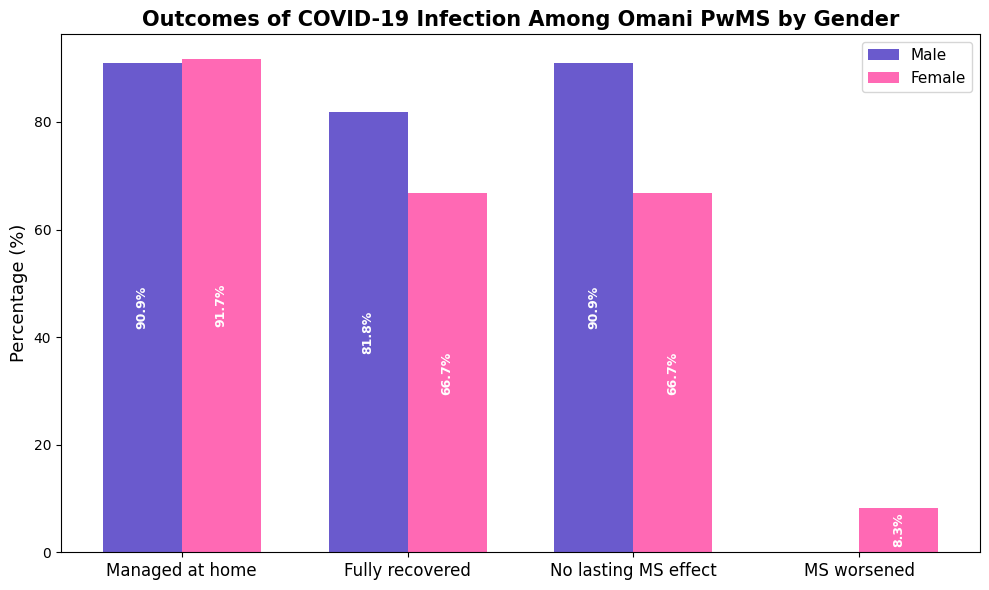
Investigate the incidence and clinical outcomes of COVID-19 infection among Omani PwMS.
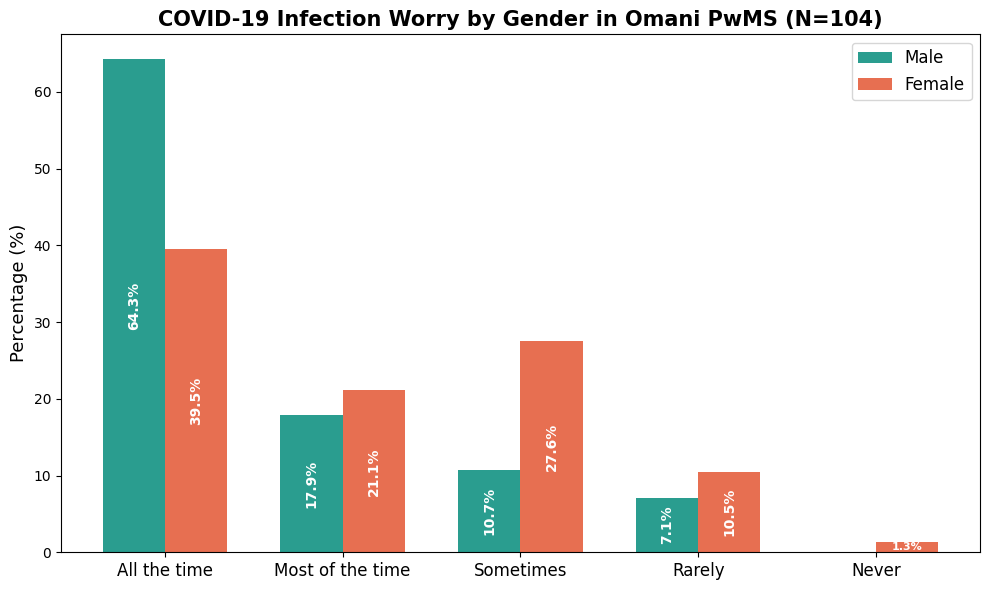
Investigate the psychosocial impact of the pandemic on PwMS and its demographic and clinical determinants.
Cross-sectional study of 104 adult Omani PwMS, at Sultan Qaboos University Hospital (SQUH) between Jan–Apr 2021.
Data collected via structured phone interviews and medical record reviews; COVID-19 diagnosis confirmed via PCR.
Assessed disease characteristics, MS relapses, DMT adherence, access to care, COVID-19 symptoms, and psychosocial status.
Statistical analyses were conducted using R version 4.2.2 and included both descriptive and inferential statistics.
| Variable | All Participants (n=104) | COVID19 Infected (n=23) |
| Sex, n (%) | ||
| Male | 28 (26.9%) | 11 (47.8%) |
| Female | 76 (73.1%) | 12 (52.2%) |
| Age, years (range) | 39.2 (23–66) | 38.9 (27–58) |
| EDSS severity, n | ||
| Slight (1.0–1.5) | 35 | 7 |
| Minimal (2.0–2.5) | 19 | 4 |
| Moderate (3.0–4.5) | 19 | 5 |
| Severe (≥5.0) | 30 | 7 |
| DMT use, n | 88 | 21 |
| None | 16 | 2 |
| Oral DMT (teriflunomide, fingolimod, dimethyl fumarate) | 38 | 12 |
| Immune reconstitution therapy (Cladribine) | 4 | 0 |
| Infusion DMT (ocrelizumab, rituximab, natalizumab) | 41 | 9 |
| Injectable DMT (interferons and glatiramer acetate) | 5 | 0 |
| COVID-19 Pandemic Impact, n (%) | ||
| Continued DMT use | 94 (90.4%) | 18 (78.3%) |
| MS relapse(s) | 13 (12.5%) | 4 (17.4%) |
| Received IV methylprednisolone | 10 (9.6%) | 2 (8.7%) |
| Problems with prescription access | 5 (4.8%) | 2 (8.7%) |
| Neurologist appointments affected | 3 (2.9%) | 0 (0%) |
| MRI appointments affected | 20 (19.2%) | 5 (21.7%) |
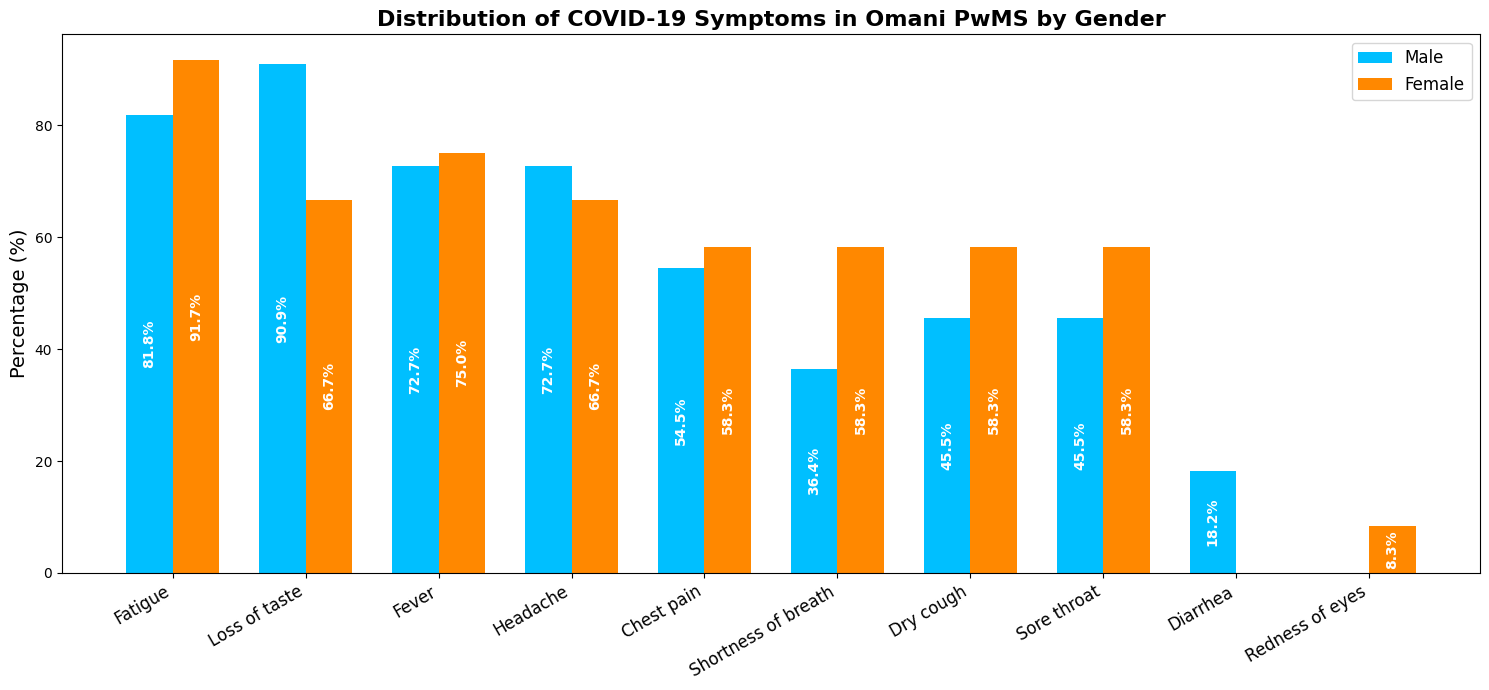
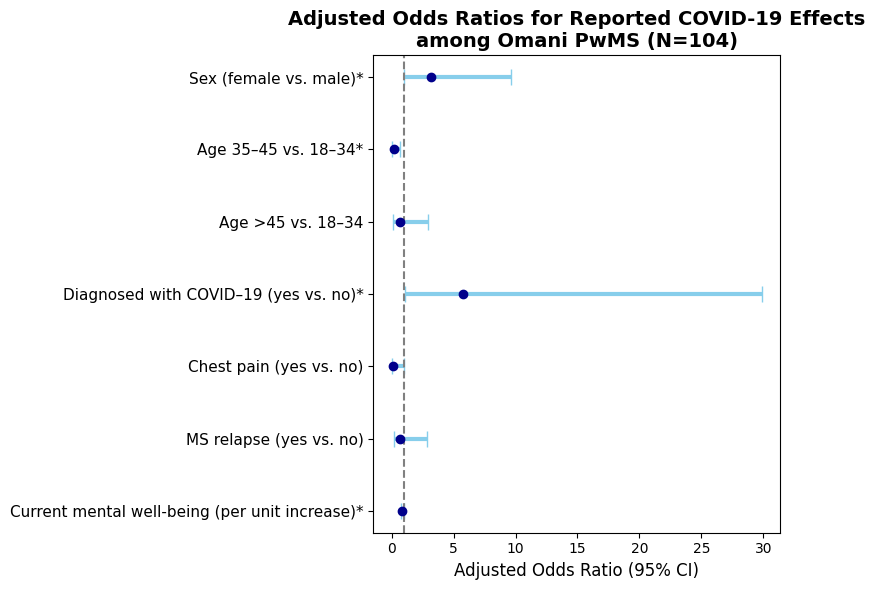
COVID-19 infection was relatively uncommon in this MS cohort, and most cases were mild.
Females, younger participants, and those with lower mental well-being were more likely to report COVID-19 effects.
Most PwMS continued their MS therapy and had minimal disruption to care.
Psychological concerns were prevalent, especially among males, despite females being more likely to report COVID-19 effects.
Severe MS worsening due to COVID-19 was rare.

This study aims to:
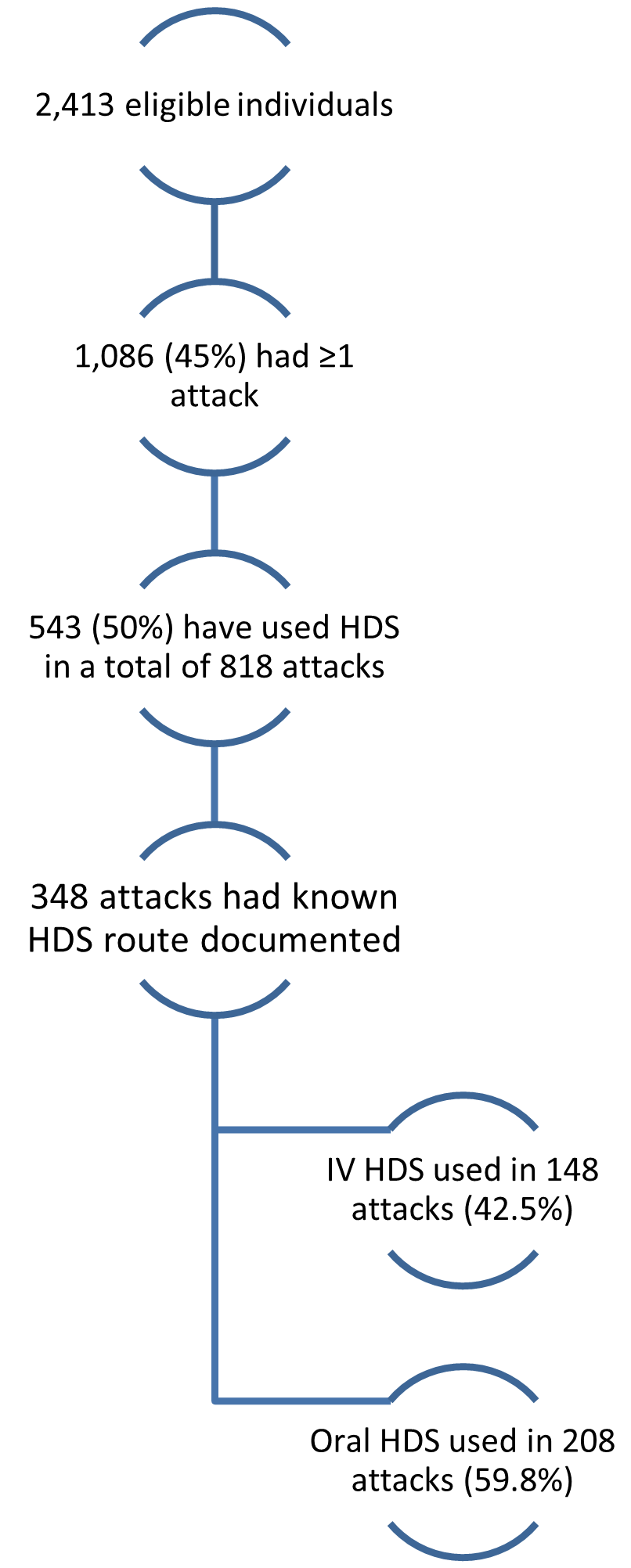
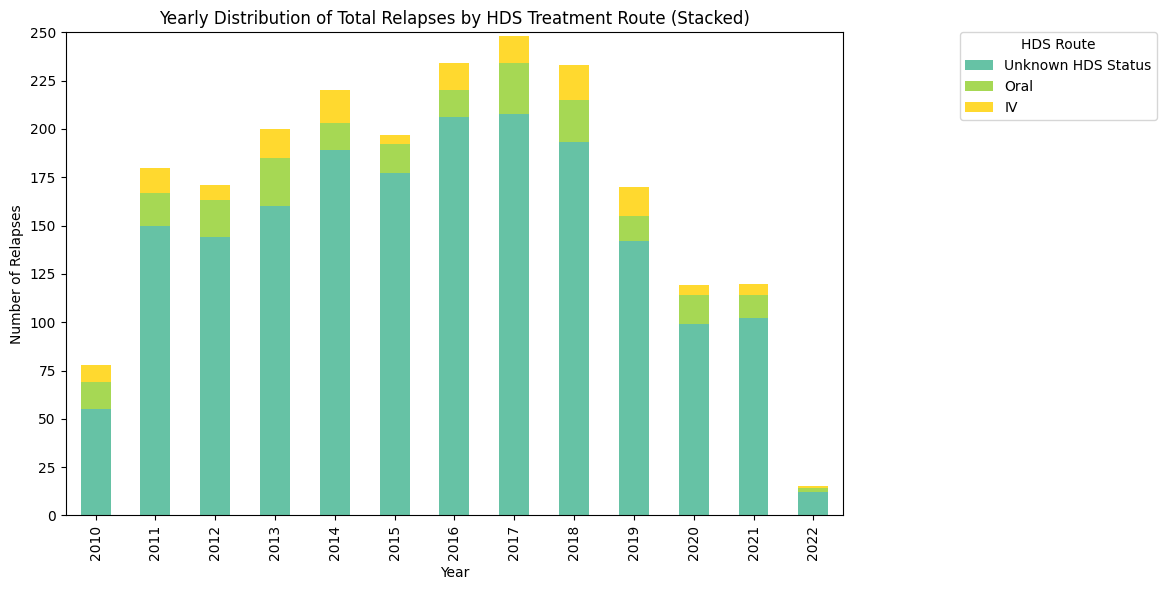
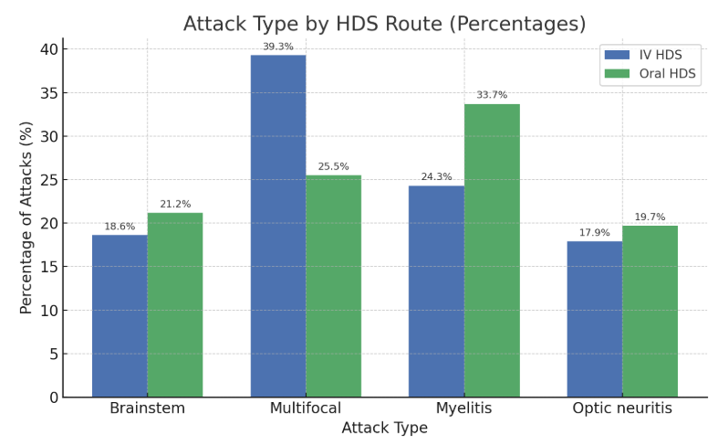
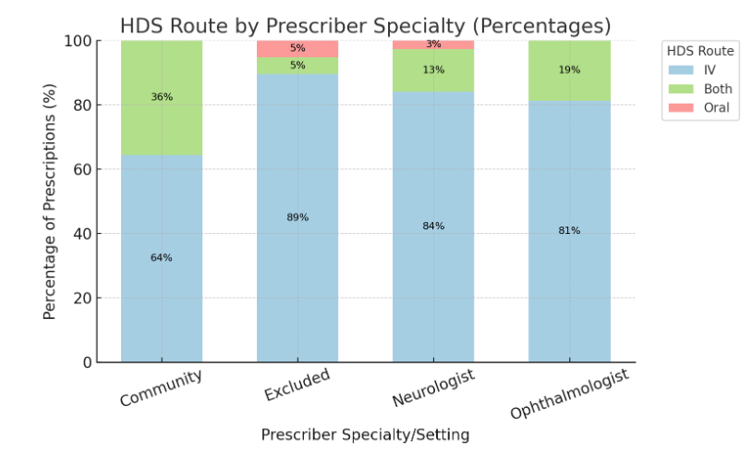
A significant association was observed between relapse type and HDS route, while prescriber specialty didn’t significantly impact route selection.
However, these findings should be interpreted with caution given the substantial proportion of relapses with undocumented HDS route and the single-center nature of the study.Multiple Sclerosis International Federation. Atlas of MS, 3rd Edition. MSIF, 2020.
Lublin, Fred D., et al. "Defining the Clinical Course of Multiple Sclerosis: The 2013 Revisions." Neurology, vol. 83, no. 3, 2014, pp. 278–286.
Sørensen, Per Soelberg. "New Management Algorithms in Multiple Sclerosis." Current Opinion in Neurology, vol. 27, no. 3, 2014, pp. 246–259.
Berkovich, Regina. "Treatment of Acute Relapses in Multiple Sclerosis." Neurotherapeutics, vol. 10, no. 1, 2013, pp. 97–105.
Morrow, S. A., et al. "Management of Multiple Sclerosis Relapses in Canada: A Survey of Neurologists." The Canadian Journal of Neurological Sciences, vol. 38, no. 5, 2011, pp. 719–725.

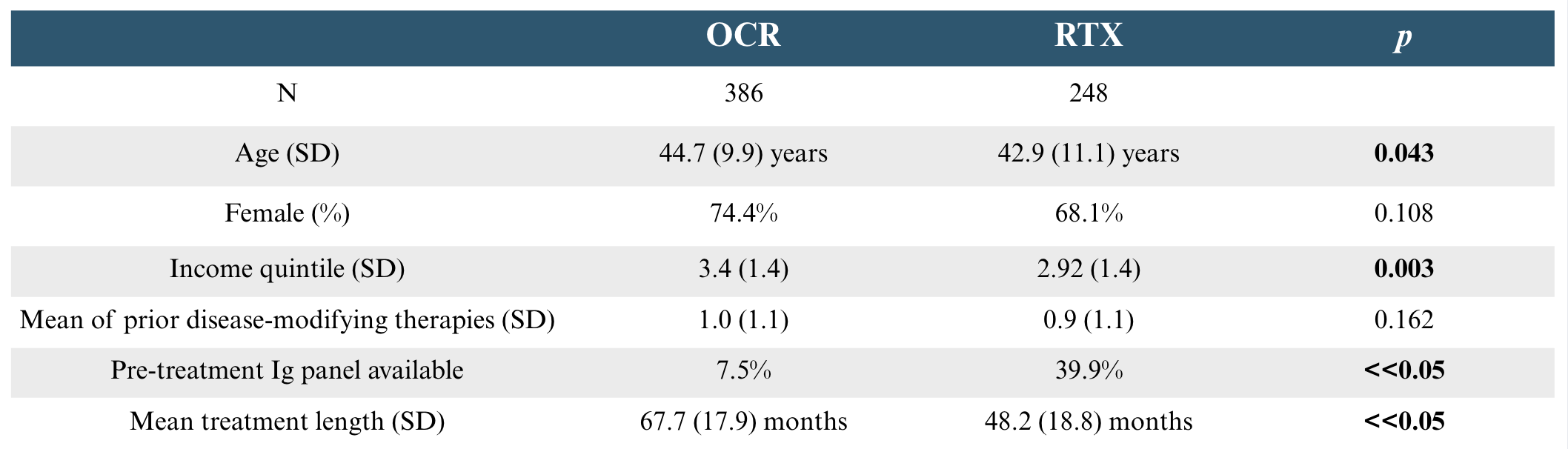
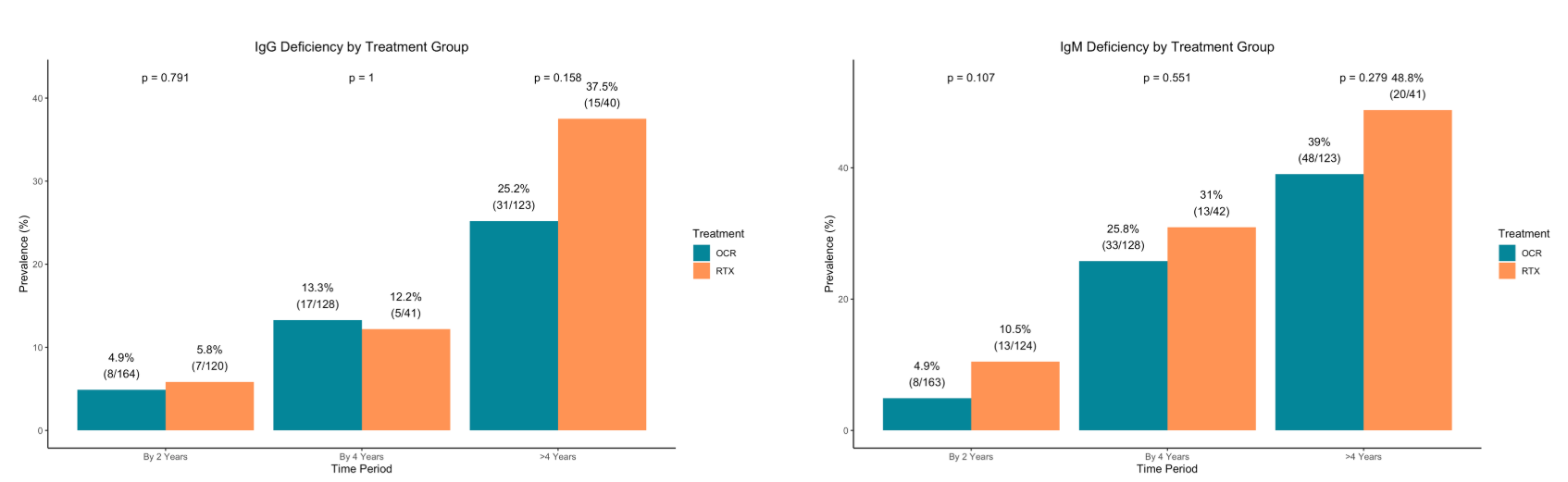
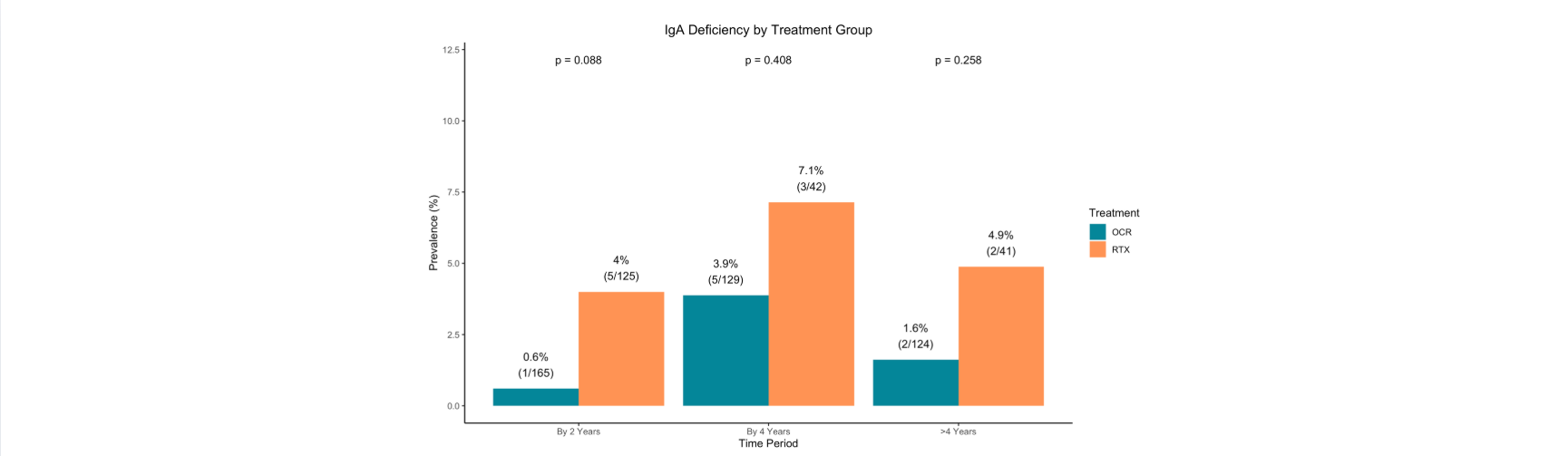
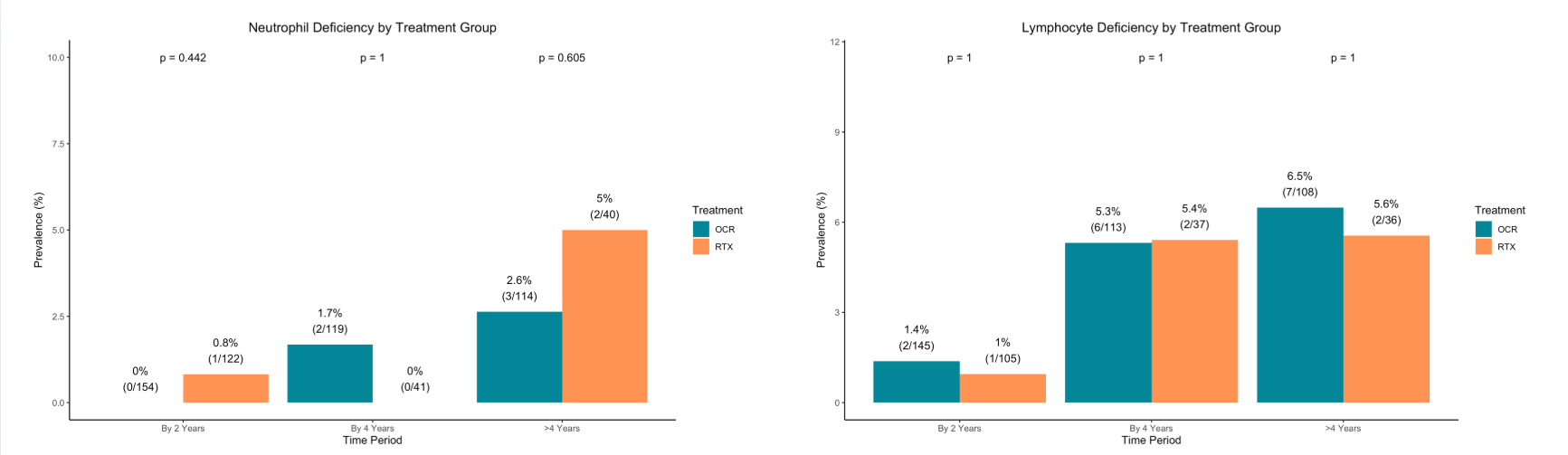
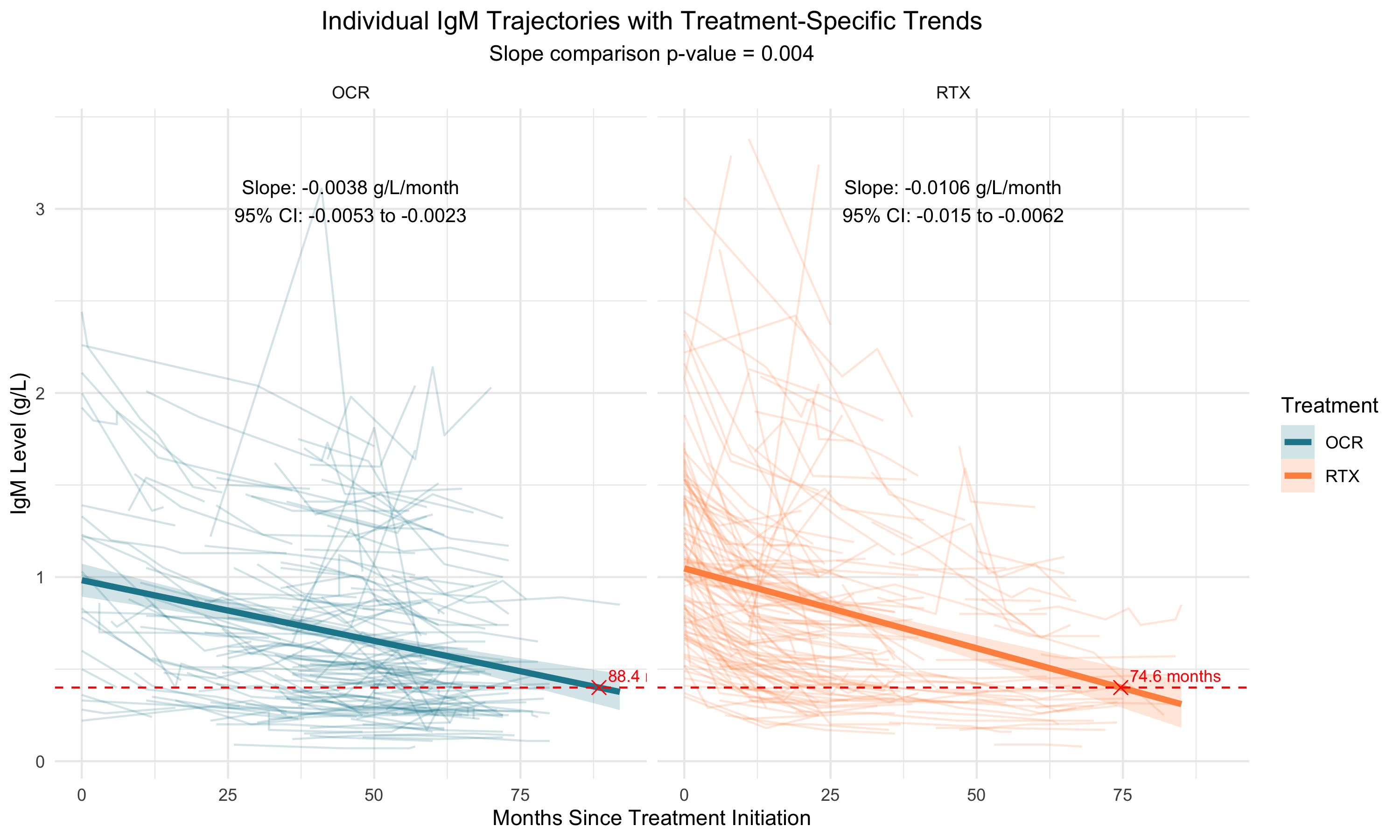
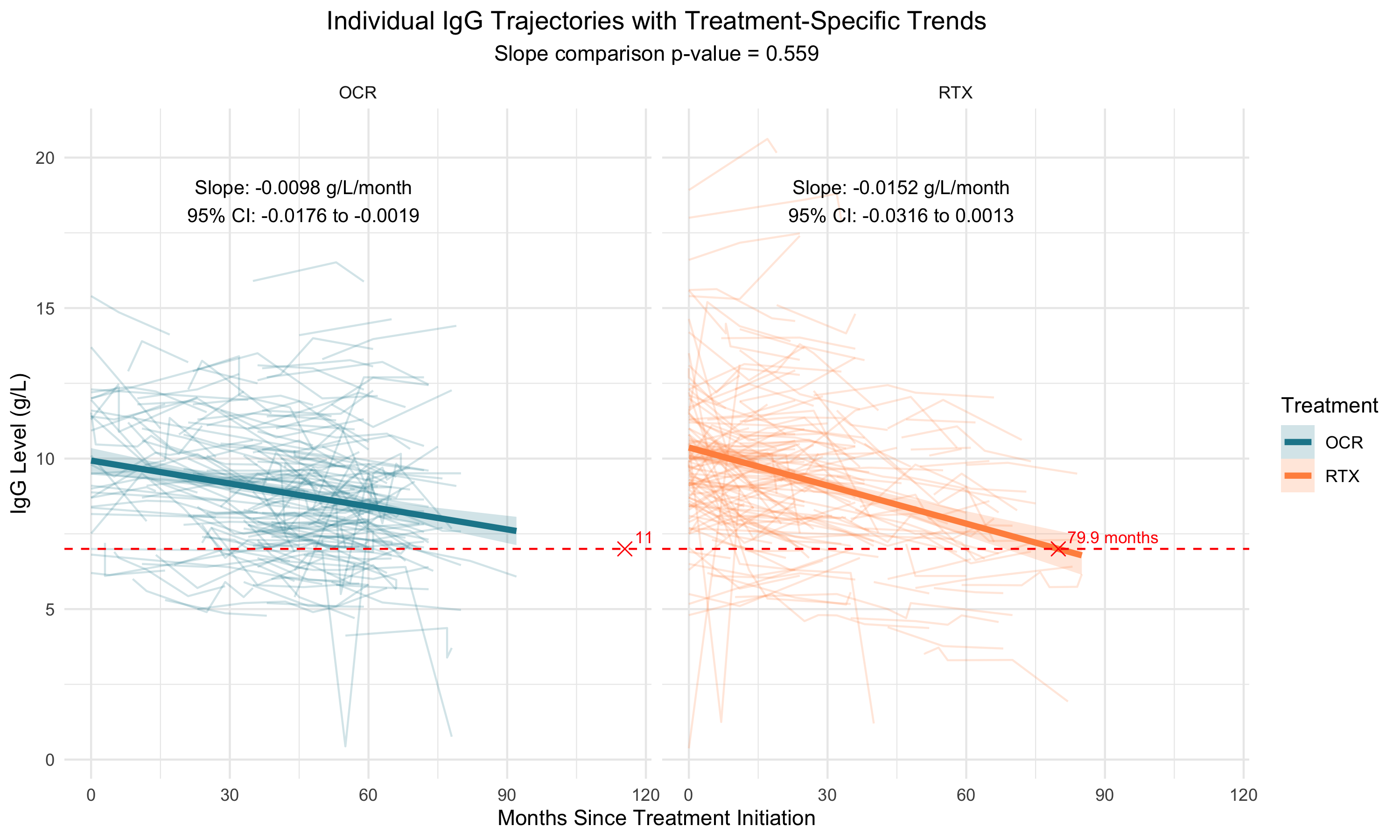
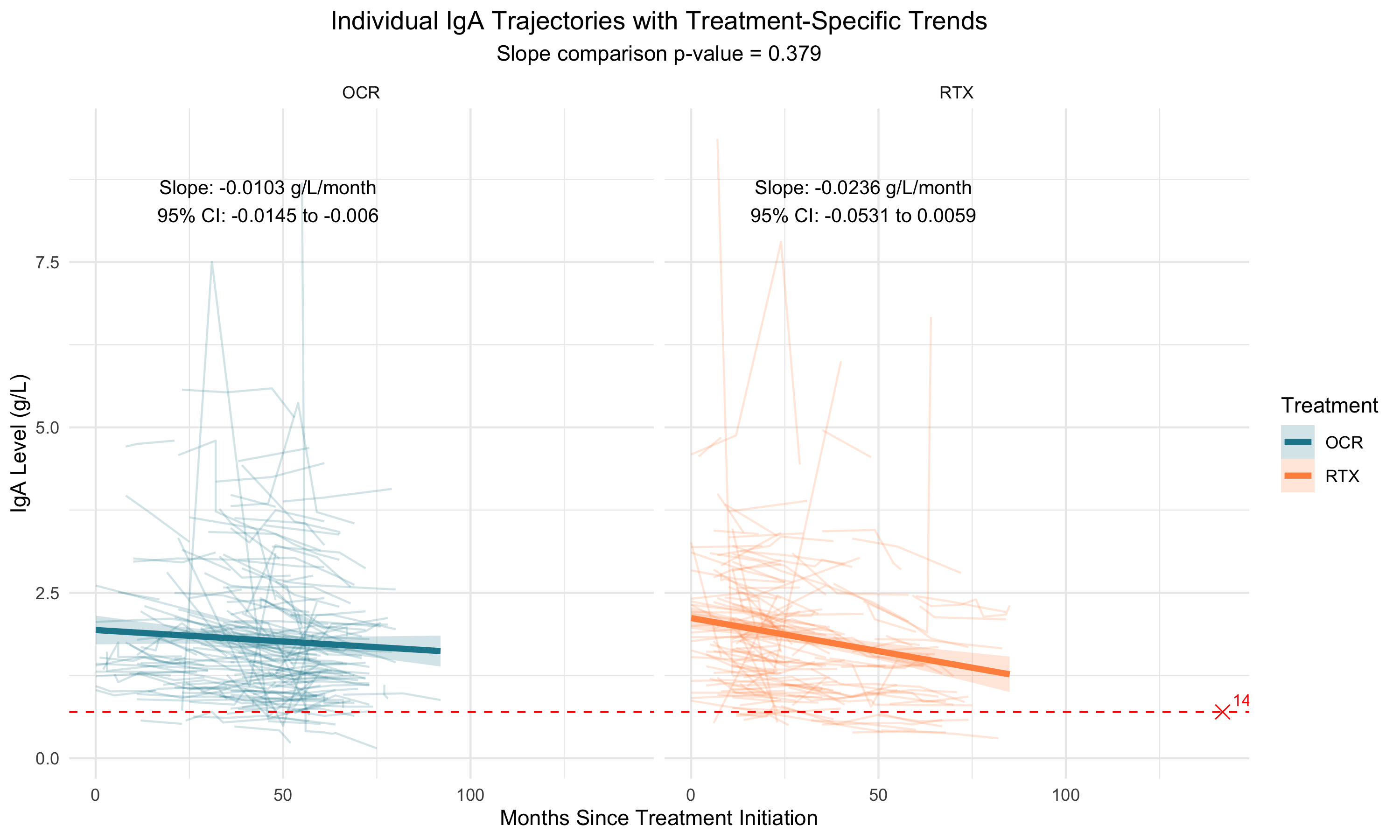
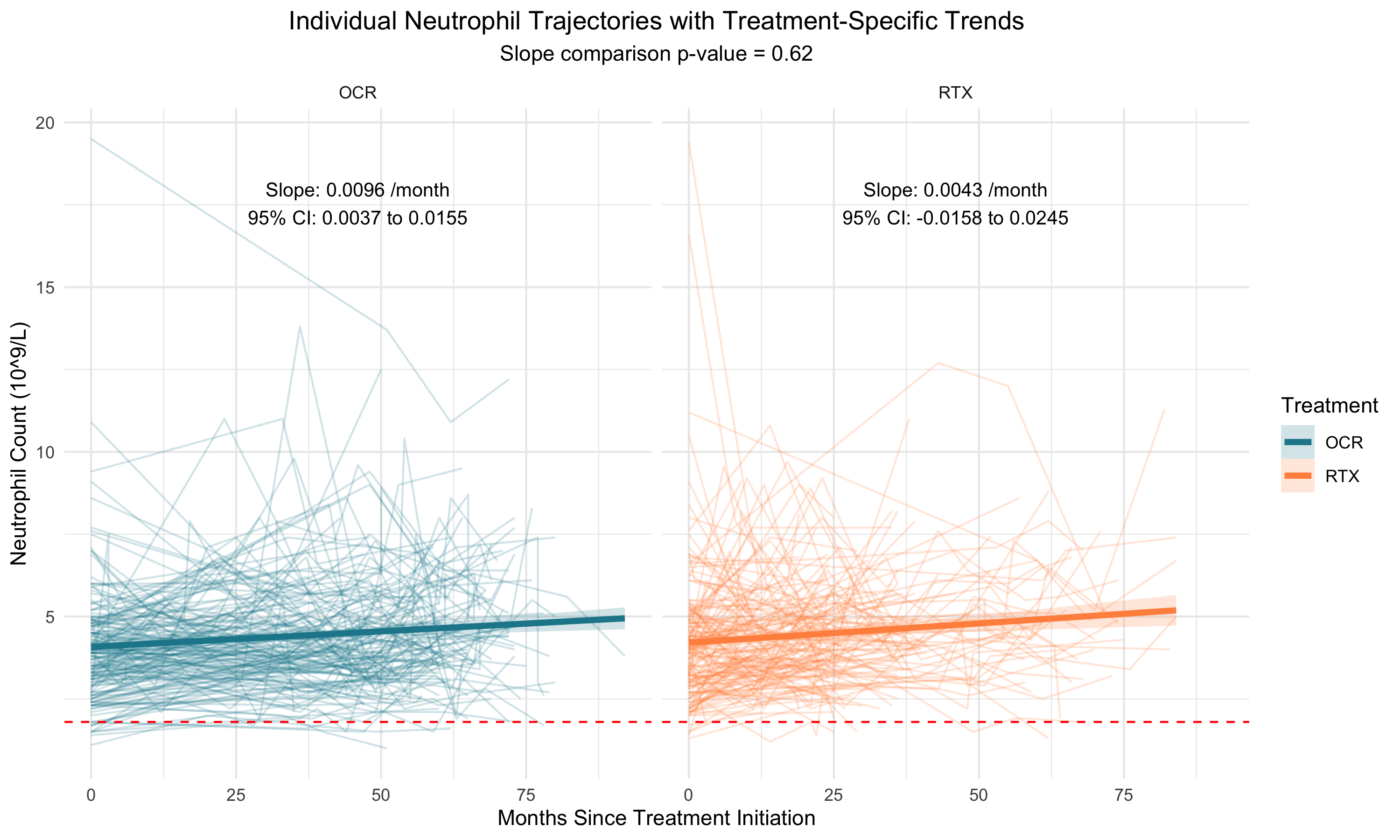
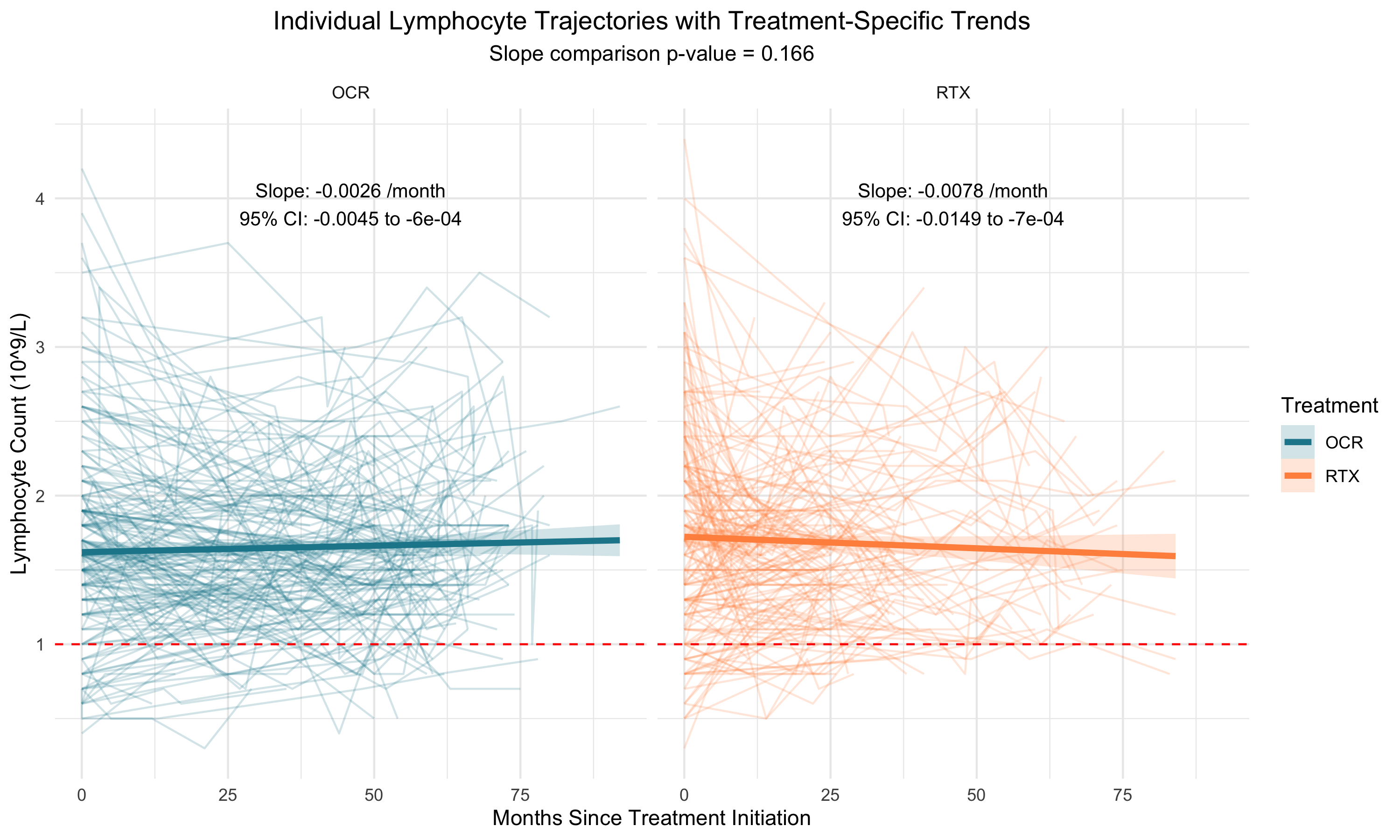
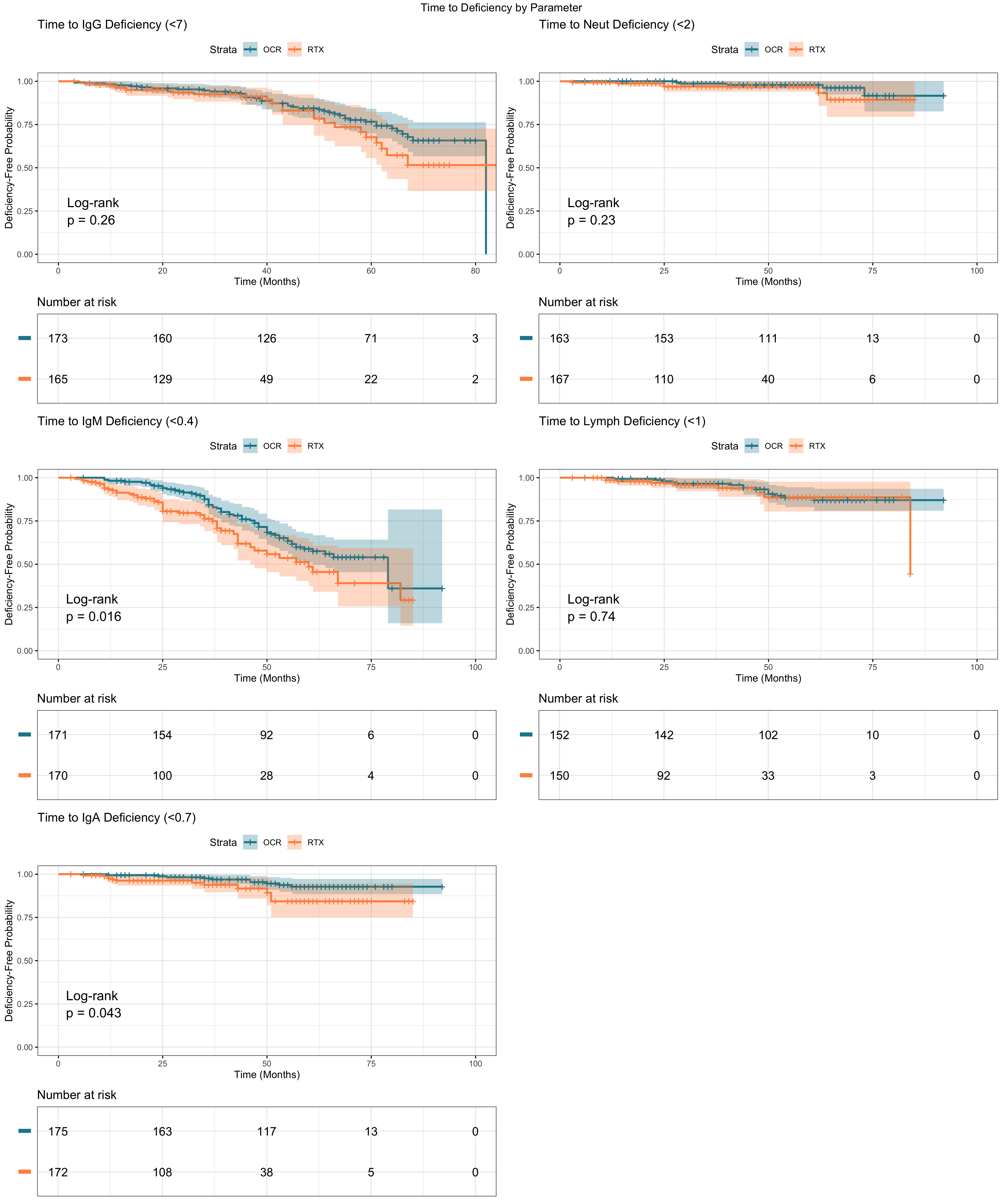
This retrospective chart review included patients with confirmed RMS who initiated treatment with OCR or RTX between January 2017 and June 2023, and who had at least one pre-treatment complete blood count (CBC) and one post-treatment CBC and immunoglobulin panel available. Treatment assignment was primarily influenced by insurance coverage. Lymphocyte, neutrophil and immunoglobulin levels (IgG, IgA, IgM) from before and after treatment initiation were collected, where available. Deficiencies were defined as values below the lower limit of normal as per local laboratory guidelines. The statistical approach comprised three complementary analyses:
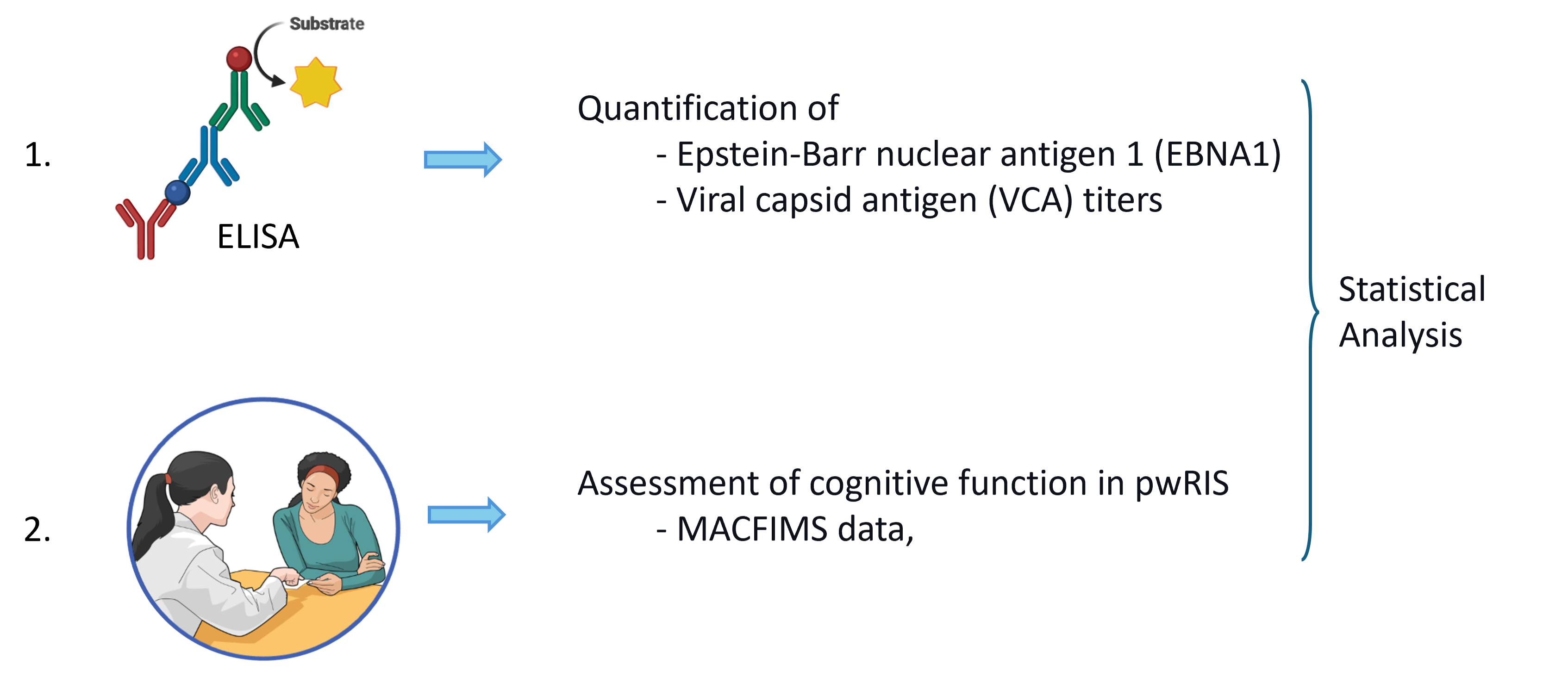
EBV antigen titers were quantified in a cohort of 37 pwRIS, 50 people with MS (pwMS), and 24 healthy controls (HC) using Enzyme-Linked Immunosorbent Assay (ELISA). Cognitive function of pwRIS were assessed using Minimal Assessment of Cognitive Function in Multiple Sclerosis (MACFIMS).
Anti-EBV Antibody Responses Across MS Subtypes and RIS
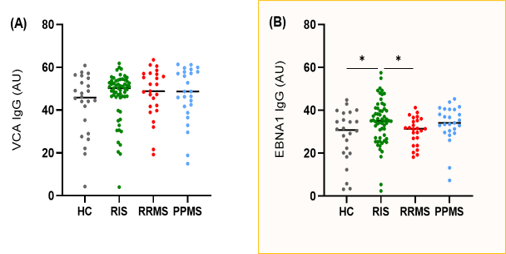
Anti-EBV Antibody Titers in Relation to Global Impairment
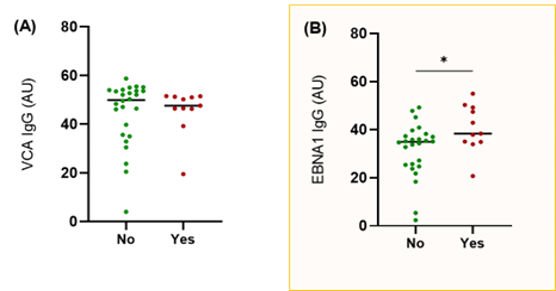
Figure 2. Anti-EBV antibody titers in patients with or without global impairment. (A) VCA IgG titers and (B) EBNA1 IgG titers measured by ELISA. *p < 0.05 with Mann-Whitney U test.
Association Between EBV Antibody Levels and Cognitive Function
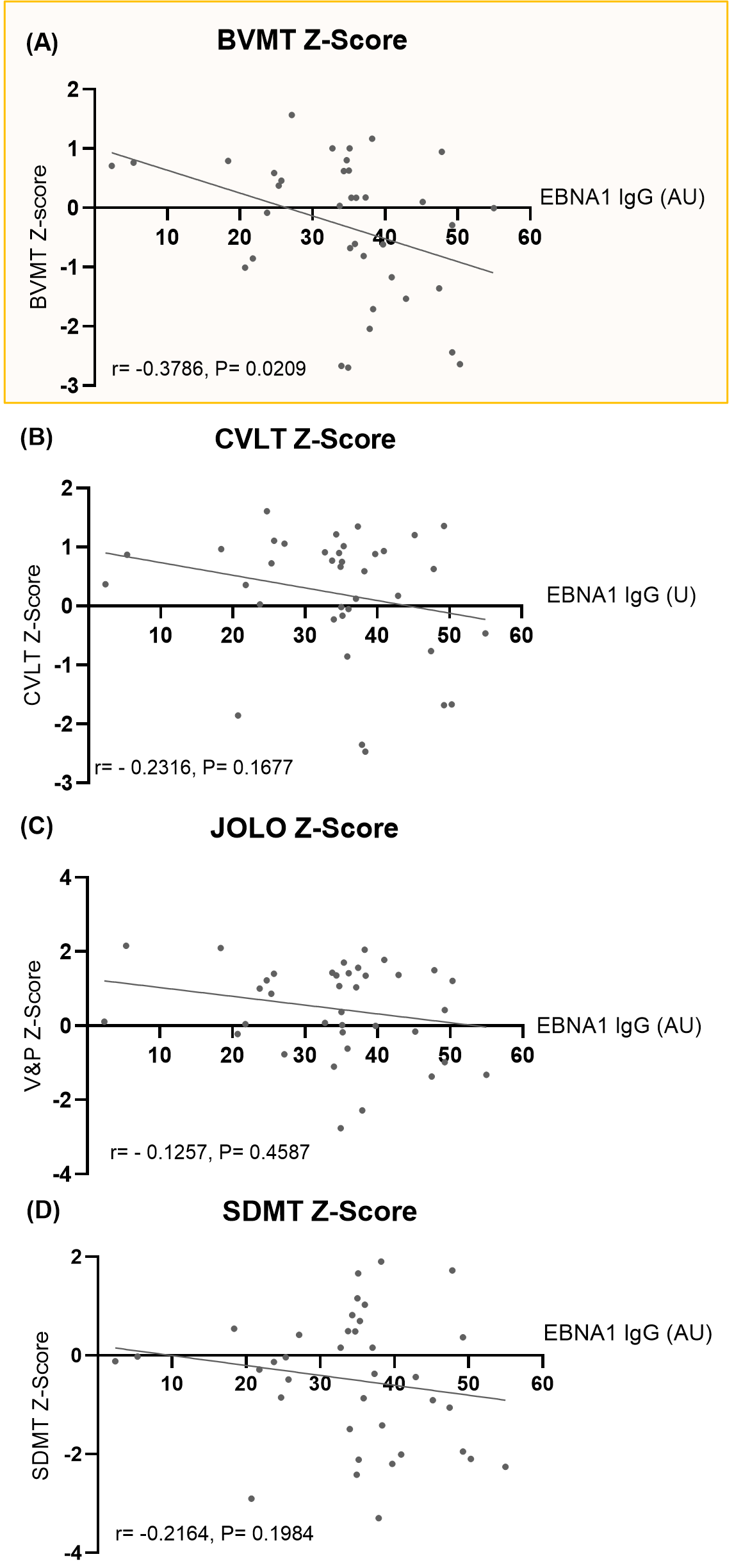
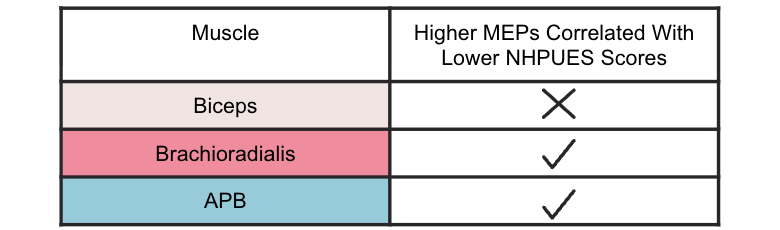
Figure 3. Correlation of EBNA1 IgG Titers with Minimal Assessment of Cognitive Function in Multiple Sclerosis (MACFIMS) Scores. Scatter plots showing the correlation between EBNA1 IgG titers and Z-scores from (A) Brief Visuospatial Memory Test (BVMT), (B) California Verbal Learning Test (CVLT), (C) Judgment of Line Orientation (JOLO), and (D) Symbol Digit Modalities Test (SDMT). The correlation coefficient (r) and p-values (P) were assessed using Spearman rank correlation.
Association Between EBV Antibody Levels and Cognitive Function
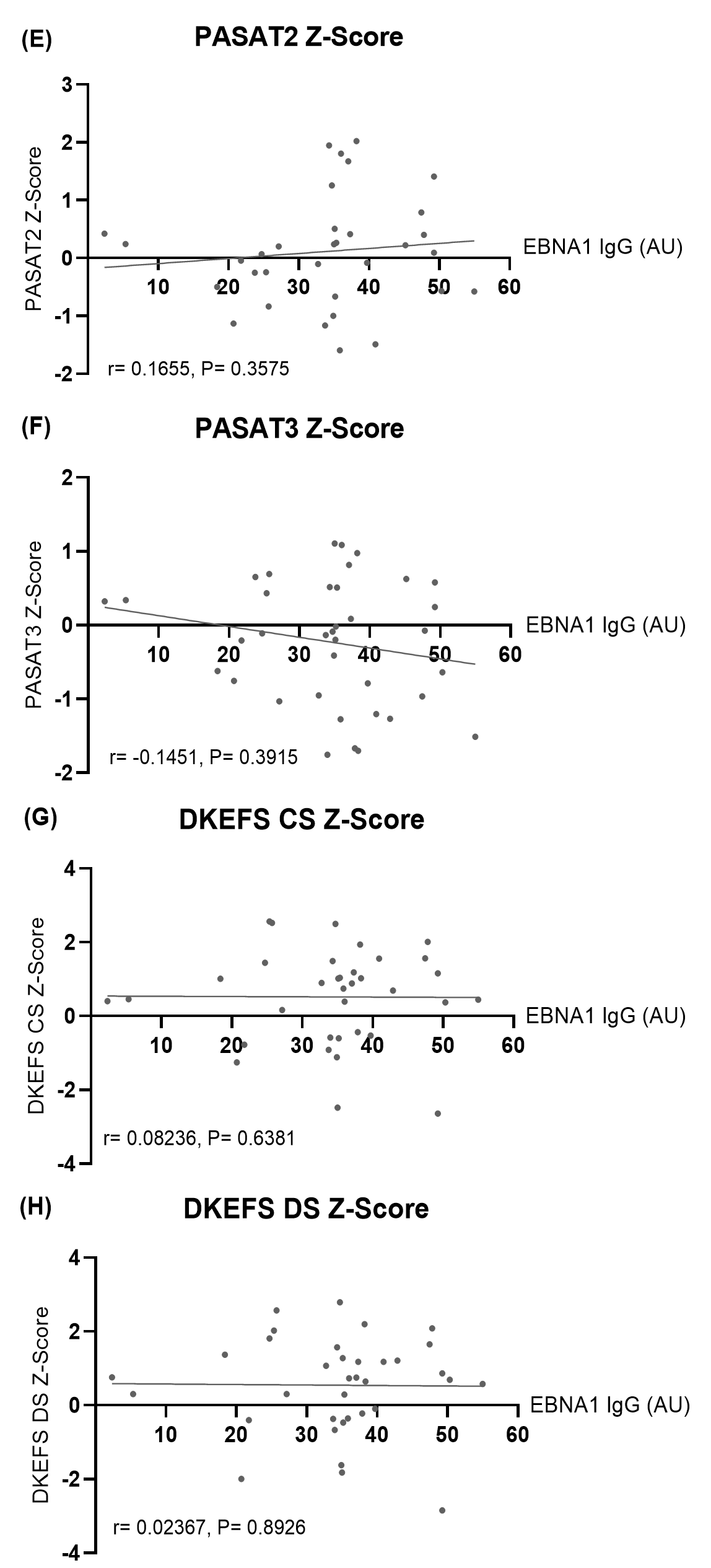
Figure 3. (E–H) Scatter plots showing the correlation between EBNA1 IgG titers and Z-scores from (E) Paced Auditory Serial Addition Test 2-second version (PASAT2), (F) PASAT 3-second version (PASAT3), (G) Delis-Kaplan Executive Function System - Color-Word Interference Test: Condition 3 (DKEFS CS), and (H) DKEFS - Design Fluency: Condition 1 (DKEFS DS). The correlations were assessed using Spearman rank correlation.
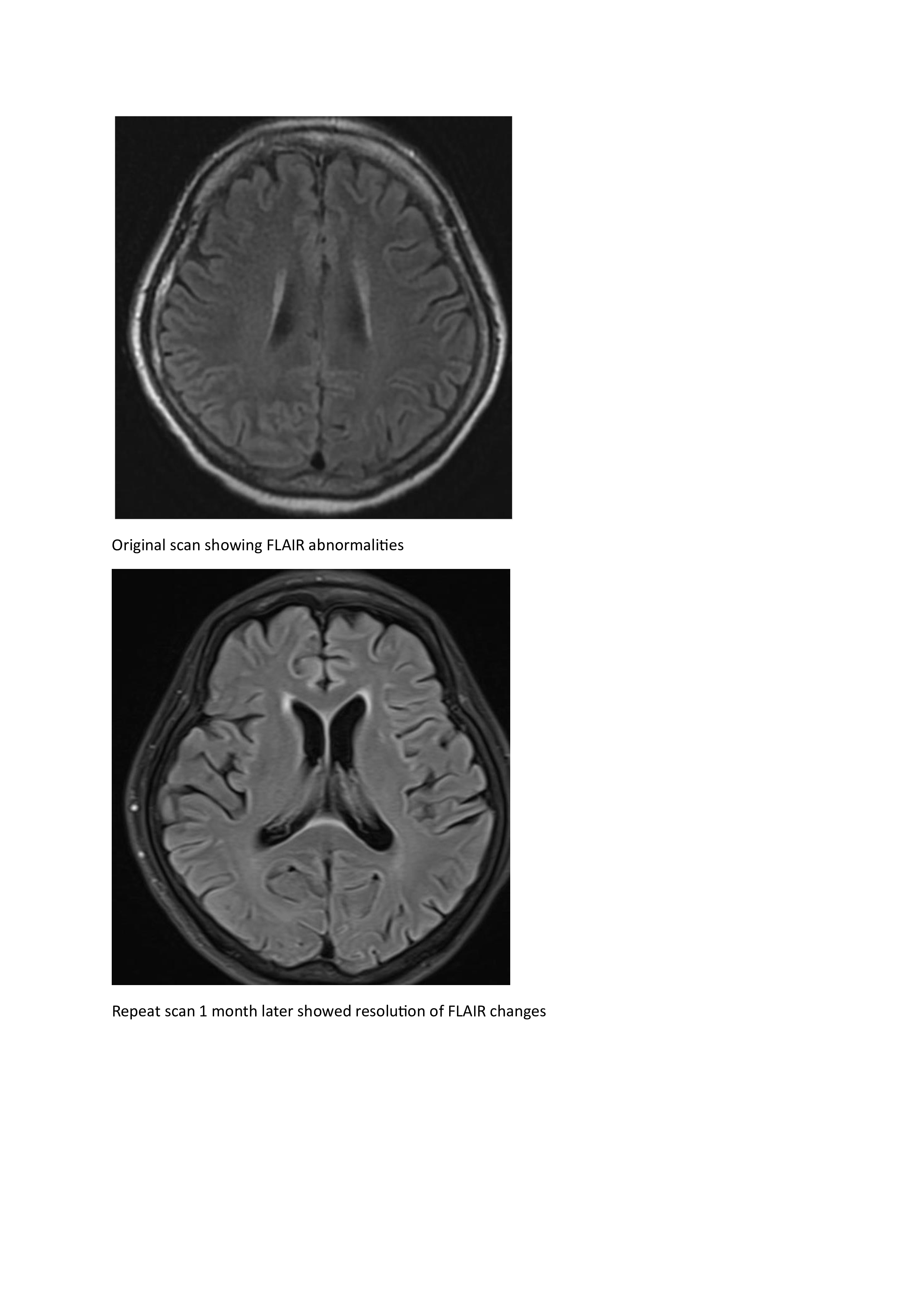
Hyperglycemia presenting with visual hallucinations due to occipital lobe seizures
|
Background: Hyperosmotic hyperglycemic nonketotic state (HHS) is associated with myriad neurological complications such as seizures.
Methods: We report a case presenting with visual hallucinations due to occipital lobe epilepsy.
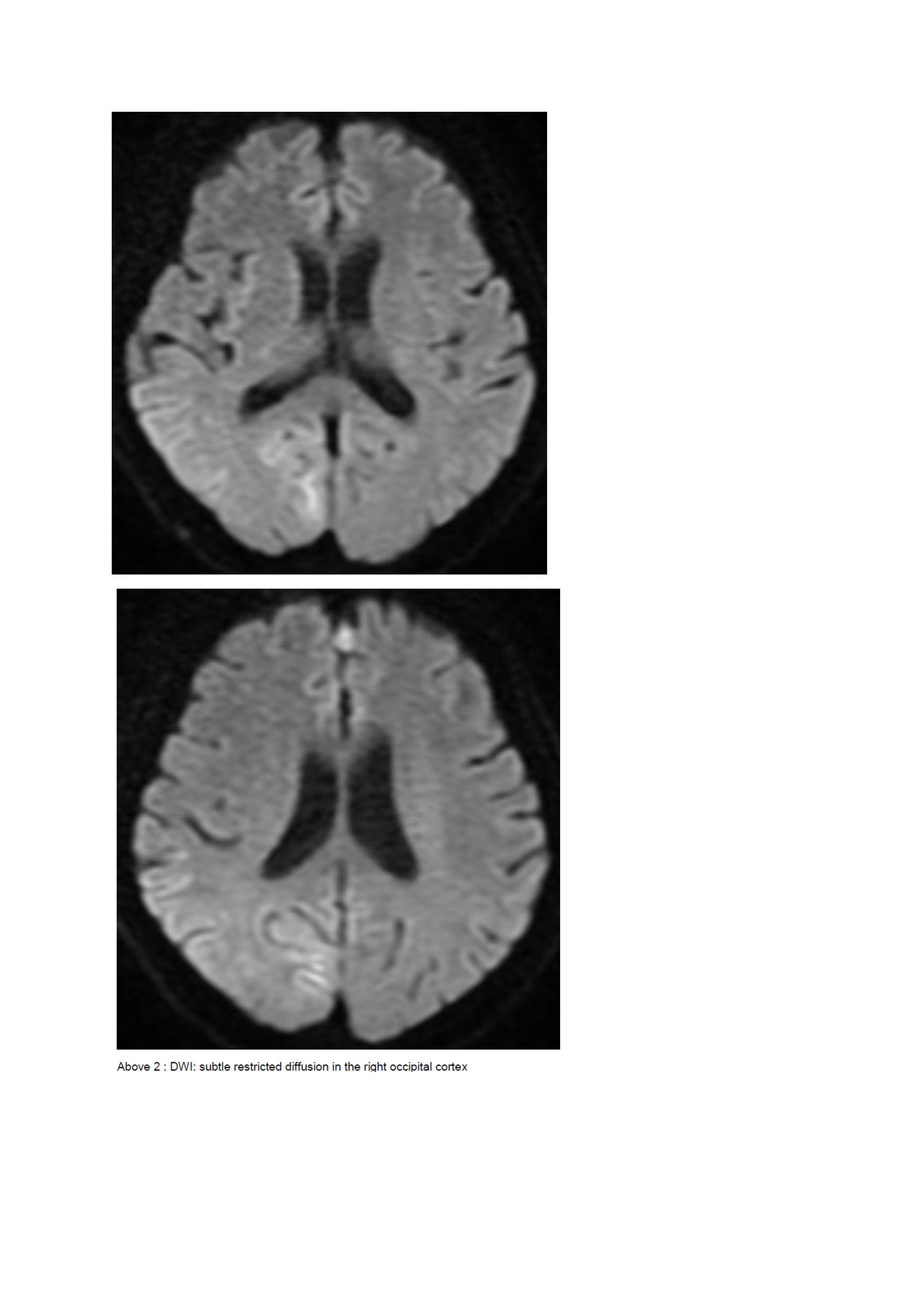
Results: A 67-year old woman with chronic hypertension, hyperlipidemia and diabetes mellitus non-compliant to medication presented with a 10-day history of recurrent visual phenomena in the left visual field. She described stationery multi-coloured flashing lights which decreased in intensity, brightness and size after 3 minutes. She was alert and conscious during attacks. There was no limb jerking. Neurological examination was normal with no visual field defect. Capillary glucose was 28.1 mmol/L, Hba1c 9% and B-hydroxybutyrate < 0.1. She was treated with actrapid 8 units, glipizide 5 mg BD and empagliflozin 12.5 mg OM. Interictal electroencephalogram was normal with no epileptiform activity. Brain magnetic resonance imaging revealed restricted diffusion in the right occipital cortex with corresponding cortical thickening and increased FLAIR signal with subtle hypodensity on GRE sequence. Her visual symptoms improved dramatically with hydration and diabetic control. She was treated with a short course of keppra. One month later repeat MRI brain showed resolution of the DWI and FLAIR abnormalities.
Conclusions: Visual hallucinations are an uncommon but well recognised and fully reversible complication of HHS. Clinicians should not forget HHS in the workup of occipital lobe. |

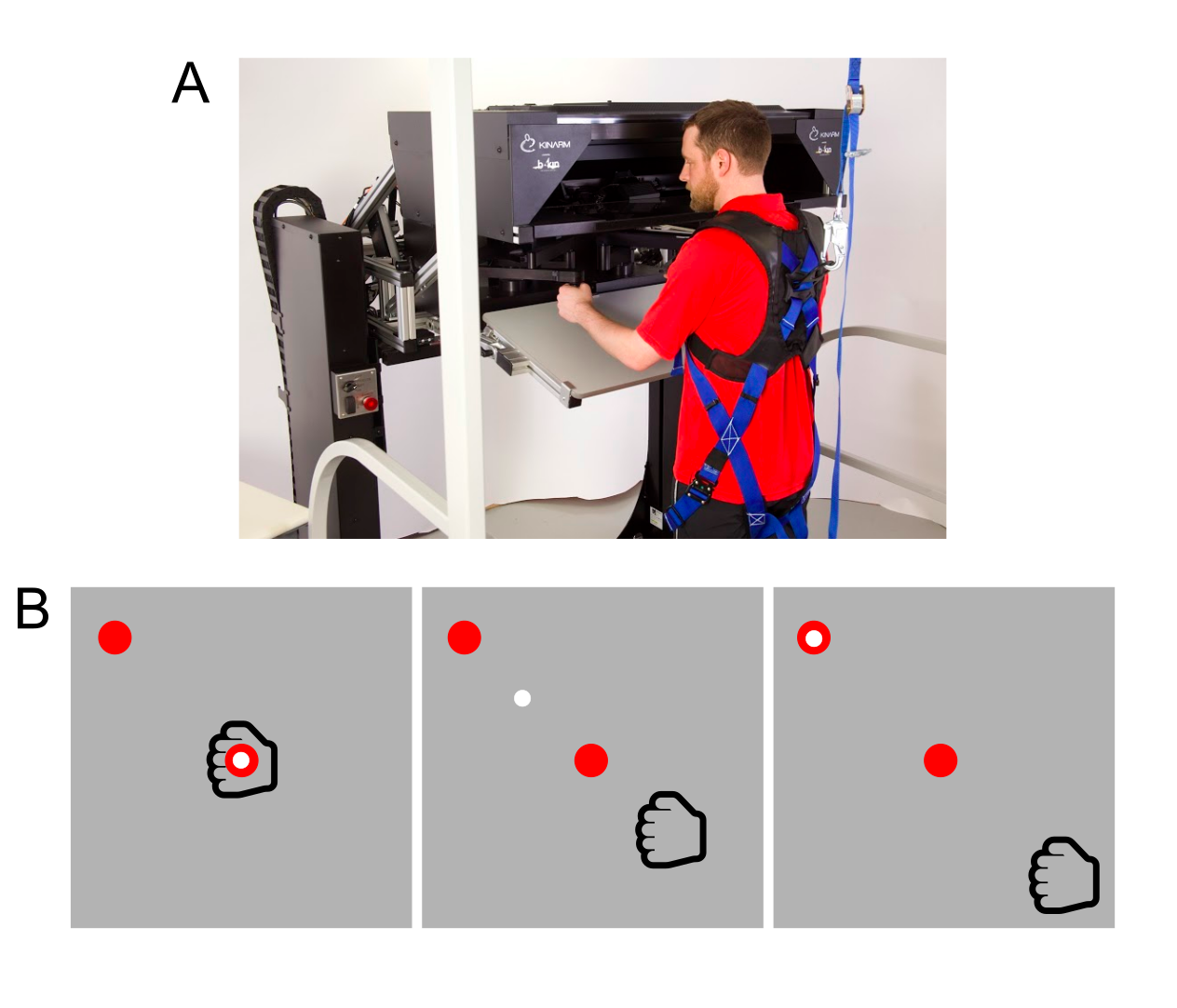
After exposure to repetitive nonconcussive impacts, football athletes will have reduced CVR and increased CBF.
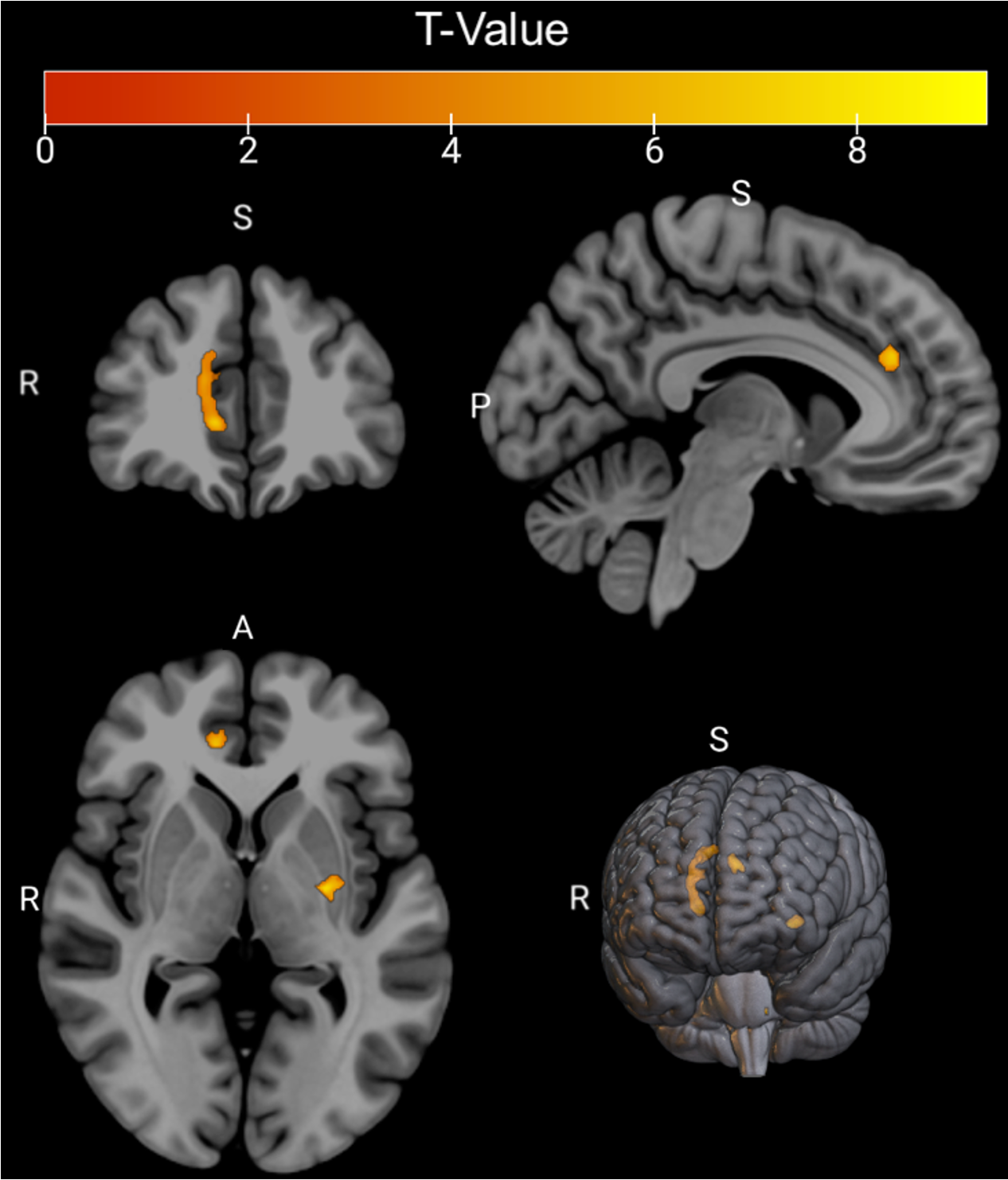
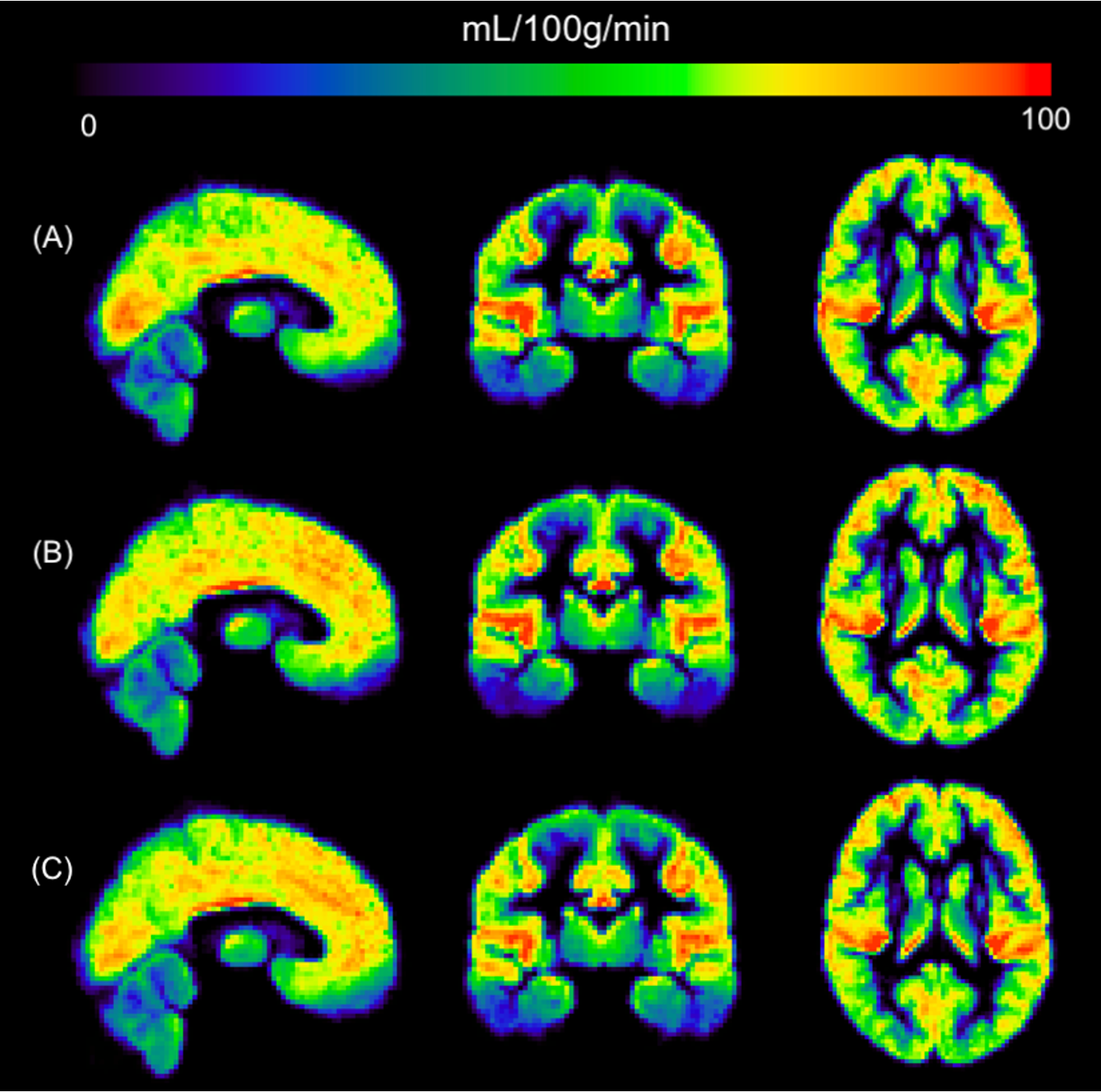
Figure 2. Average (A) PRE (n=18), (B) MID (n=18), and (C) POST (n=16) GM CBF expressed in mL/100g/min. Images are in MNI space.
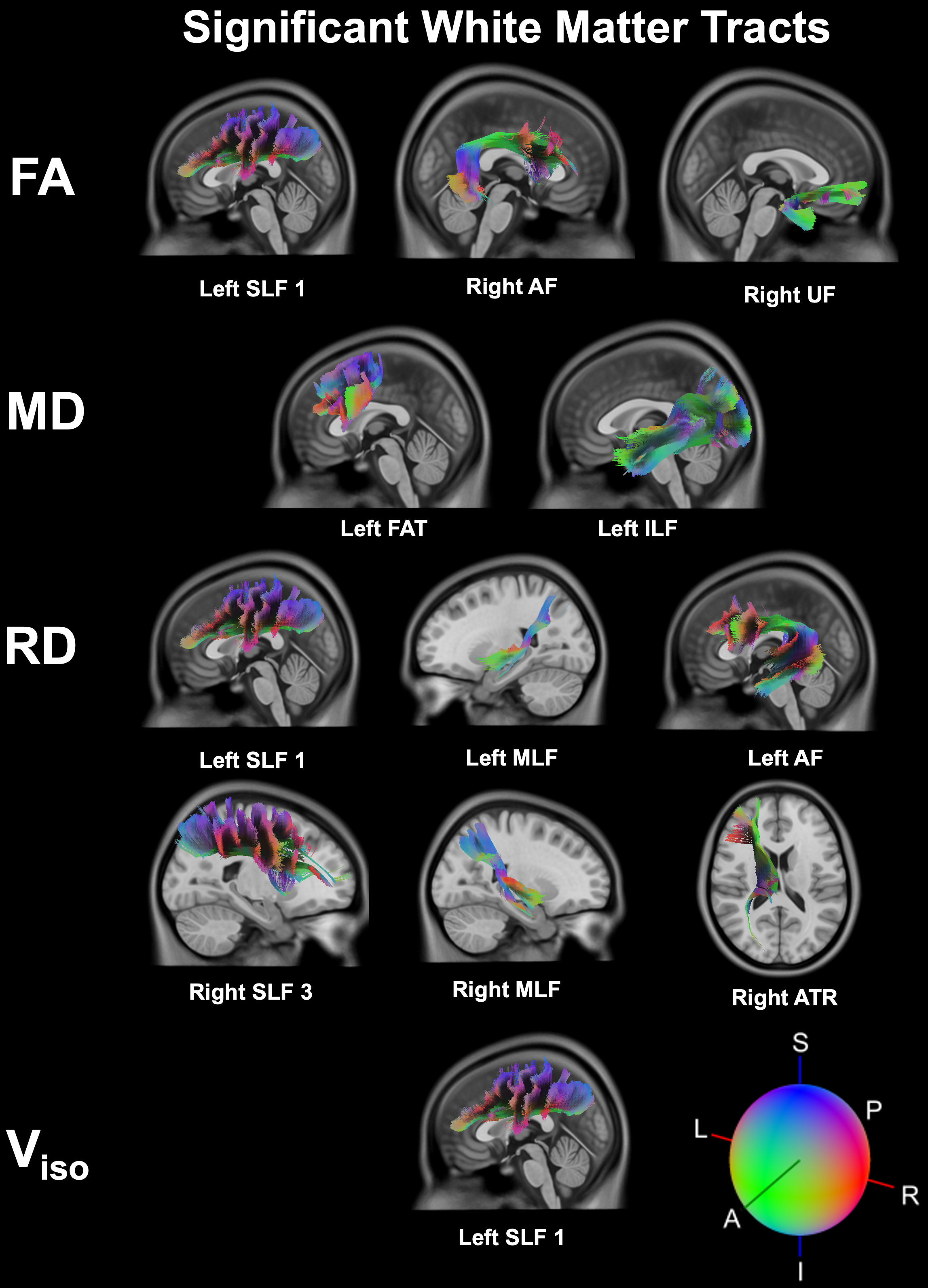
Neuroimaging (DTI/NODDI): Highly sensitive, revealing significant acute microstructural alterations in key white matter tracts.

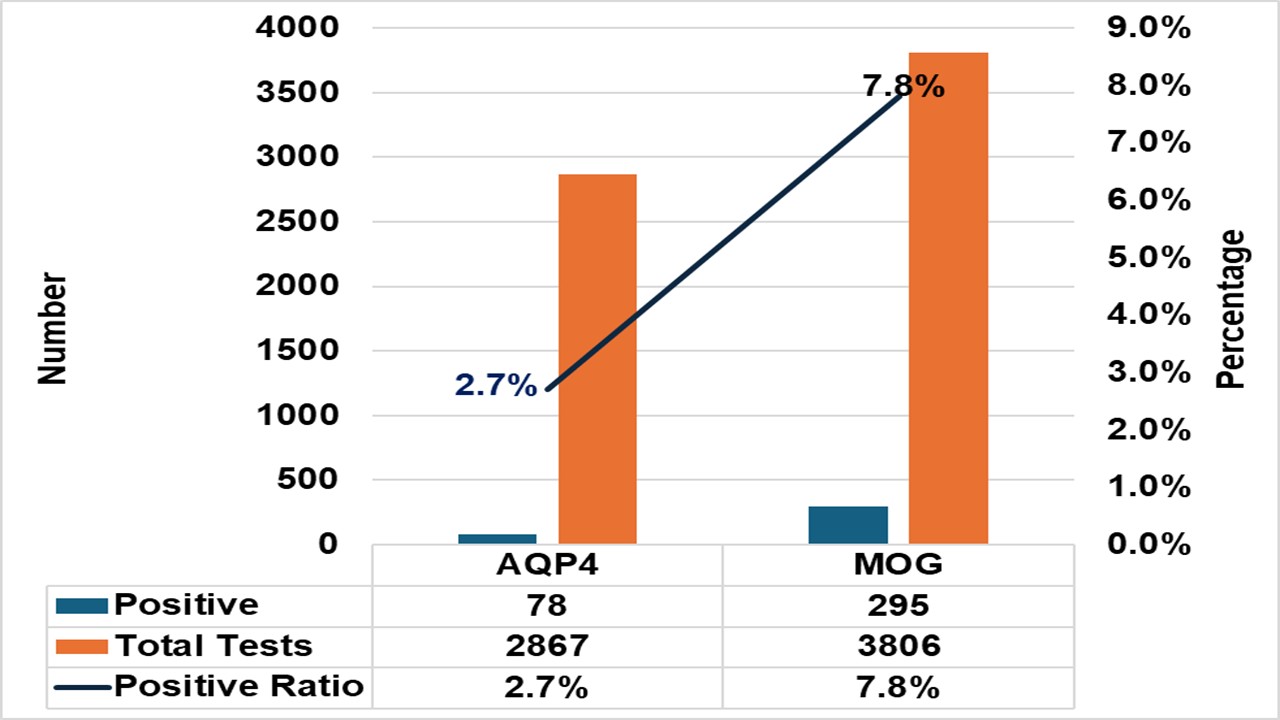
3631 patients were included for analysis:
|
|
Men (N=1778) |
Women (N=1853) |
p-value |
|
Age (mean±SD) |
68.0±13.1 |
71.8±14.6 |
0.001 |
|
Median (IQR) onset to puncture - min |
232 (155-365) |
235 (163-377) |
0.159 |
|
Median (IQR) puncture to reperfusion - min |
25 (17-37) |
24 (17-37) |
0.984 |
|
Tici 2b3 |
1446 (81.3%) |
1554 (83.9%) |
0.319 |
|
Tici 3 |
898 (50.5%) |
1021 (55.1%) |
0.264 |
|
sICH |
44 (2.5%) |
37 (2%) |
0.388 |
|
Complications
|
26 (1.5%) 11 (0.6%) 25 (1.4%) 45 (2.5%) |
30 (1.6%) 7 (0.4%) 25 (1.3%) 43 (2.3%) |
0.804 0.426 0.996 0.761 |
Table: Baseline characteristics in male and female
1. Carvalho A, Cunha A, Greg´orio T, et al. Is the efficacy of endovascular treatment for acute ischemic stroke sex-related. Interv Neurol. 2018;7:42–7. DOI10.1159/000484098.
2. Uchida K, Yoshimura S, Sakai N, Yamagami H, Morimoto T. Sex differences in management and outcomes of acute ischemic stroke with large vessel occlusion. Stroke. 2019;50:1915–8. DOI 10.1161/strokeaha.119.025344.
3. Momen AI, Francis T, Schaafsma JD, Rac V, Baig A, Pereira VM, Pikula A. Sex Differences in Functional Outcomes Following Endovascular Treatment for Acute Ischemic Stroke. Can J Neurol Sci. 2023 Mar;50(2):174-181. doi: 10.1017/cjn.2022.22.

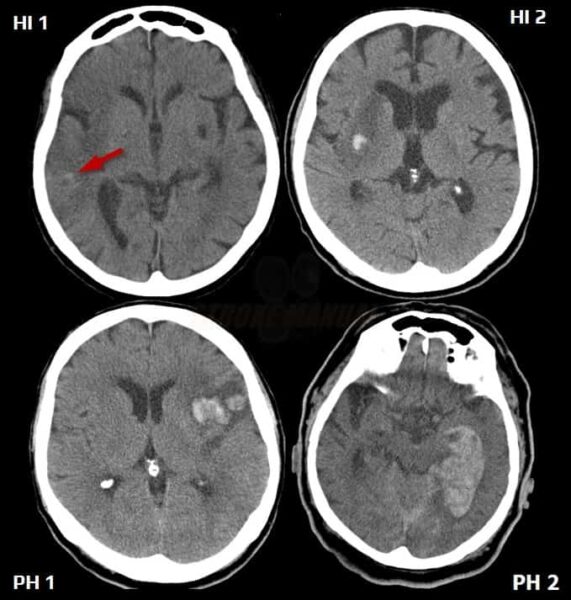
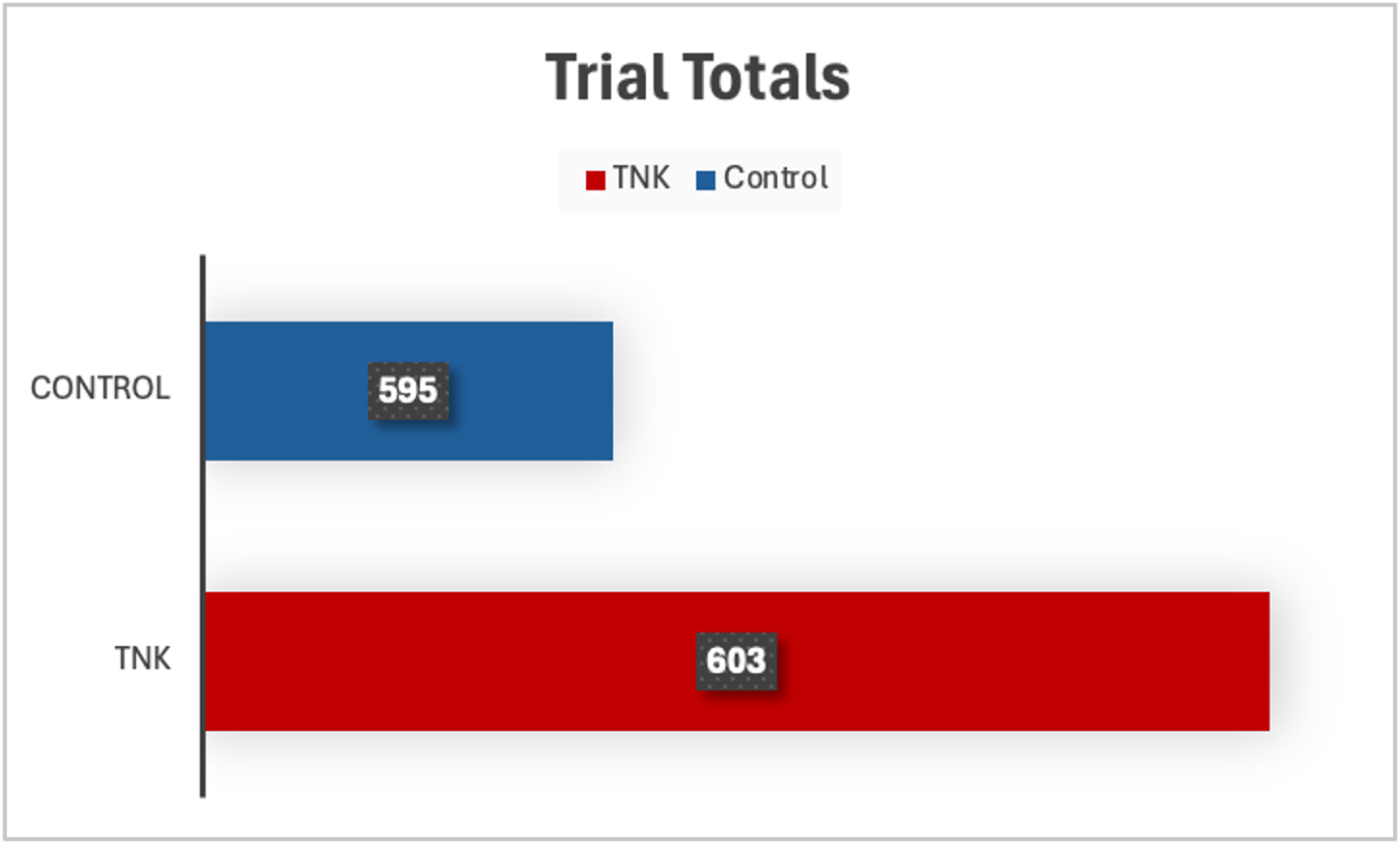
The use of Tenecteplase (TNK) in the Extended Time Window (ETW) for Acute Ischemic Stroke (AIS) remains an ongoing debate. We aim to evaluate the current literature and data of TNK use for AIS in the ETW.
Inclusion criteria for RCT of thrombolysis in the ETW:
Studies that did not meet these criteria were excluded from review.
From this, 3 RCTs were included in our review:
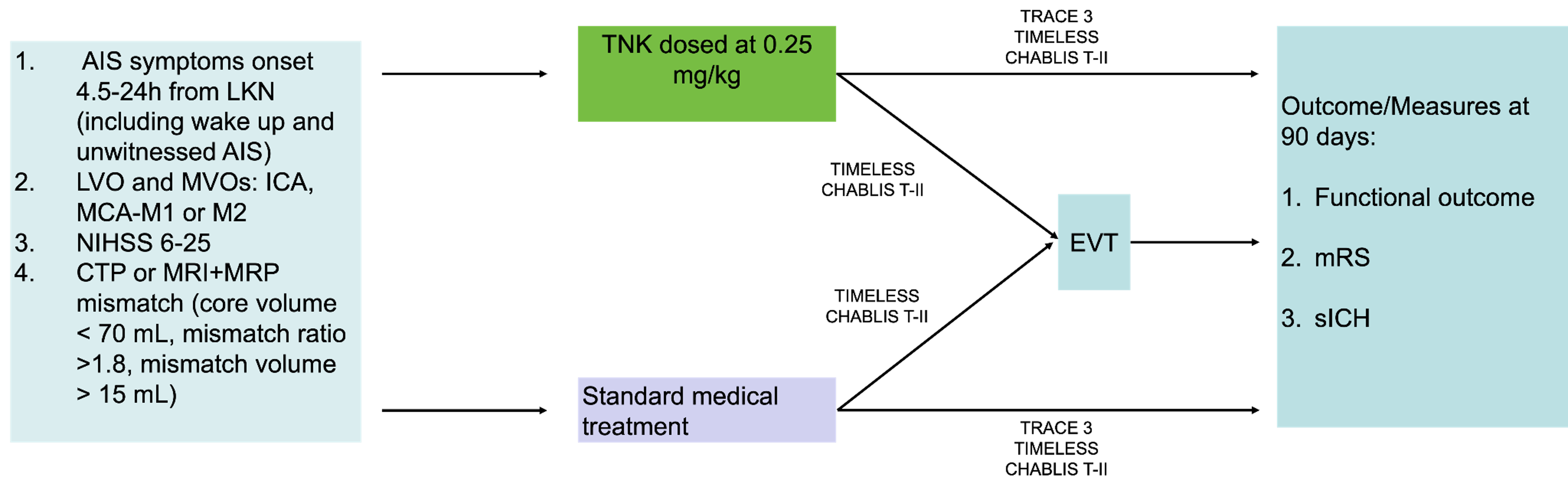
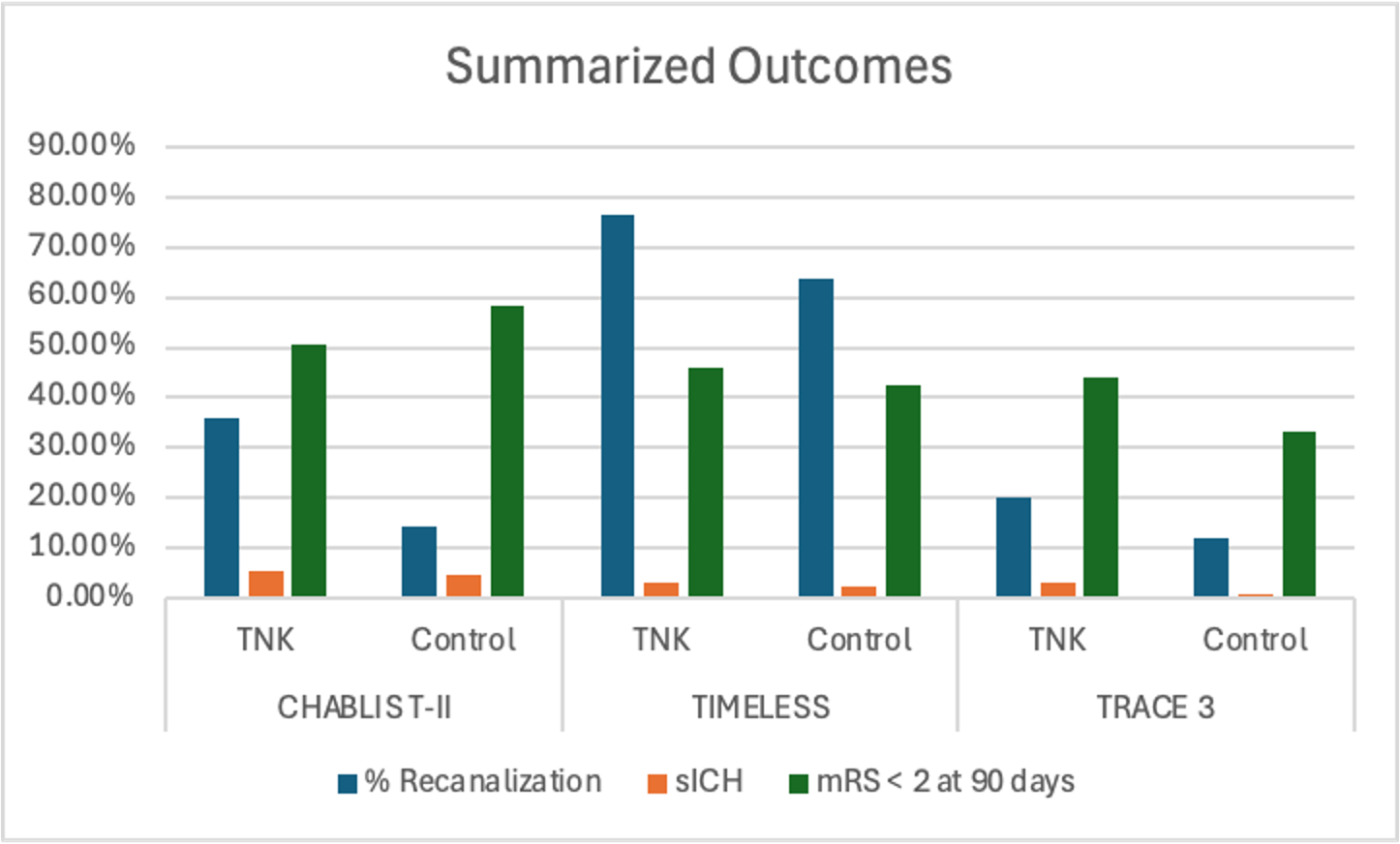
Better recanalization rates are seen with TNK in ETW, but may not be associated with improved functional outcomes at 90 days compared to medical management. Incidence of sICH also remains largely favorable, except in TRACE 3, which showed a higher incidence in the TNK group. There remains a need for more RCTs in this population.
|
Trial
|
LVO
|
EVT Access
|
Recanalization
|
Functional Outcome
|
sICH
|
|
TIMELESS |
Yes |
Yes |
TNK group: ↑ |
No difference (mRS=3) |
Similar |
|
CHABLIS-T II |
Yes |
Yes |
TNK group: ↑ |
No difference (mRS=3) |
Similar |
|
TRACE 3 |
Yes |
No |
N/A |
TNK better (33% vs. 24.2%) |
Increased in TNK group (3% vs 0.8%) |














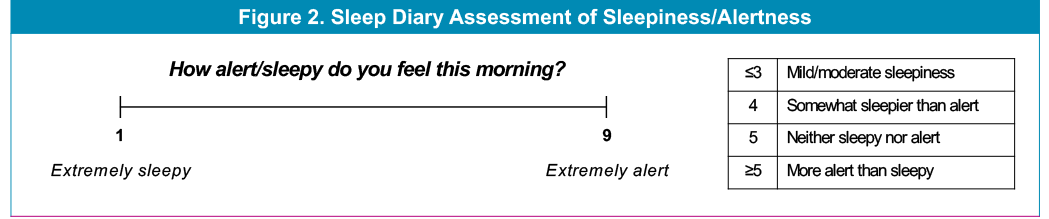

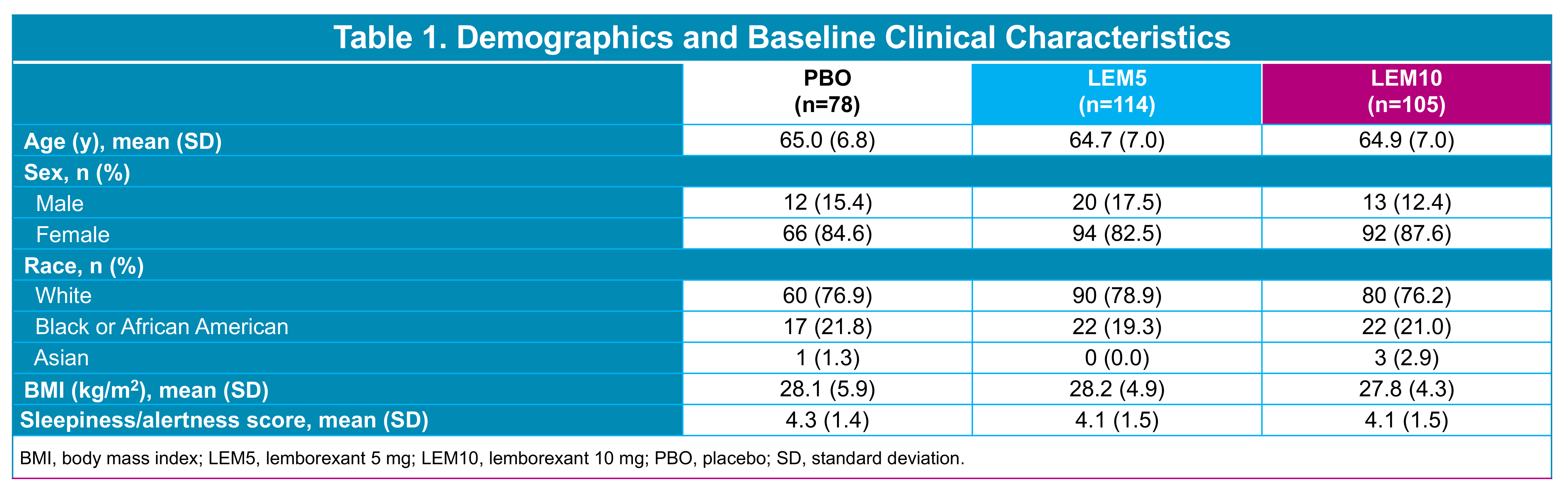
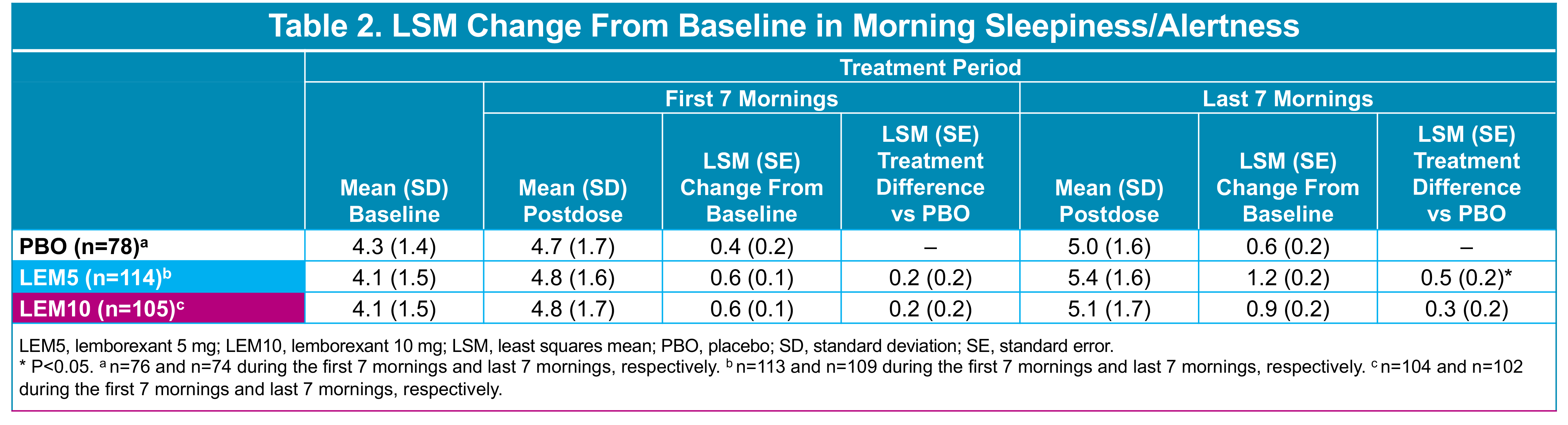
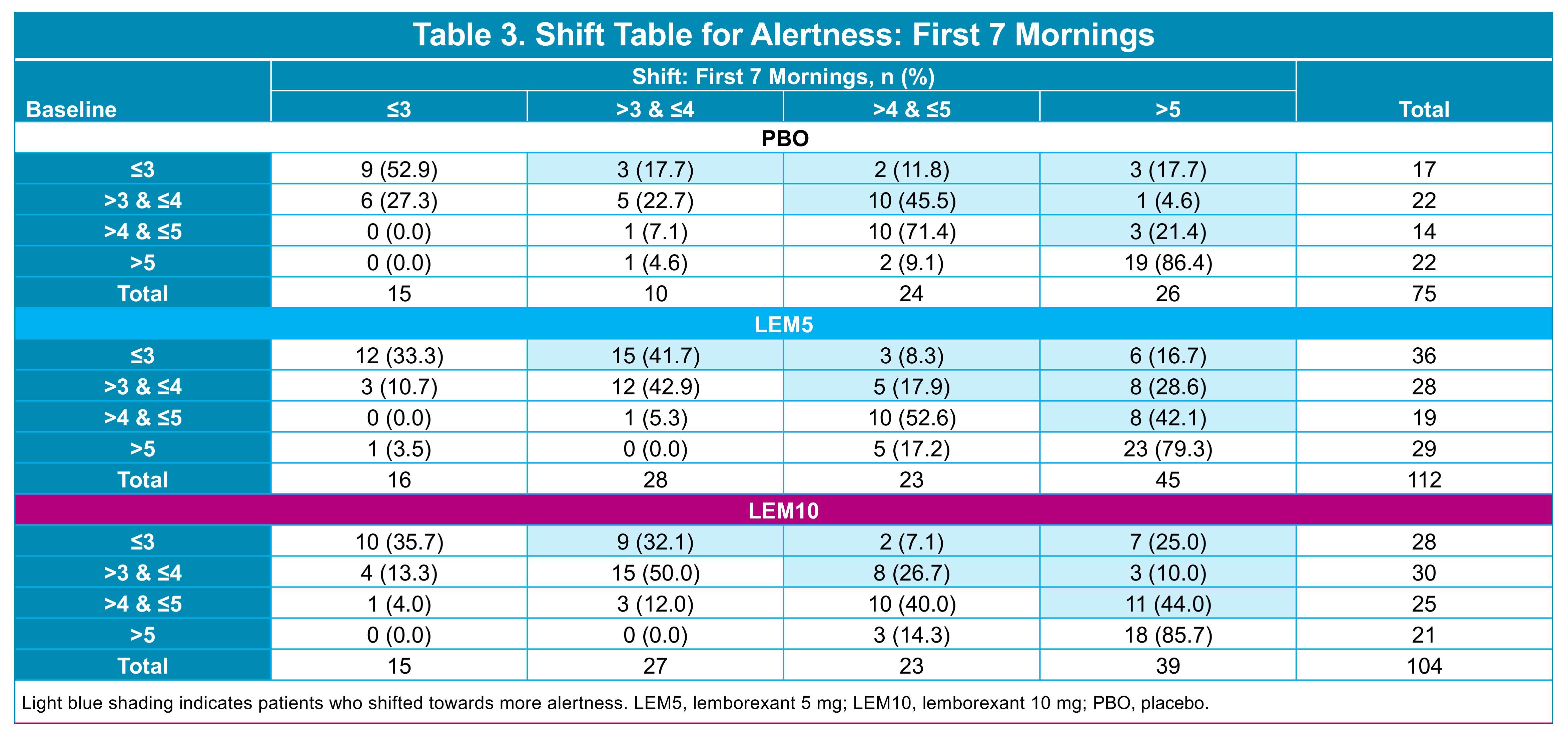
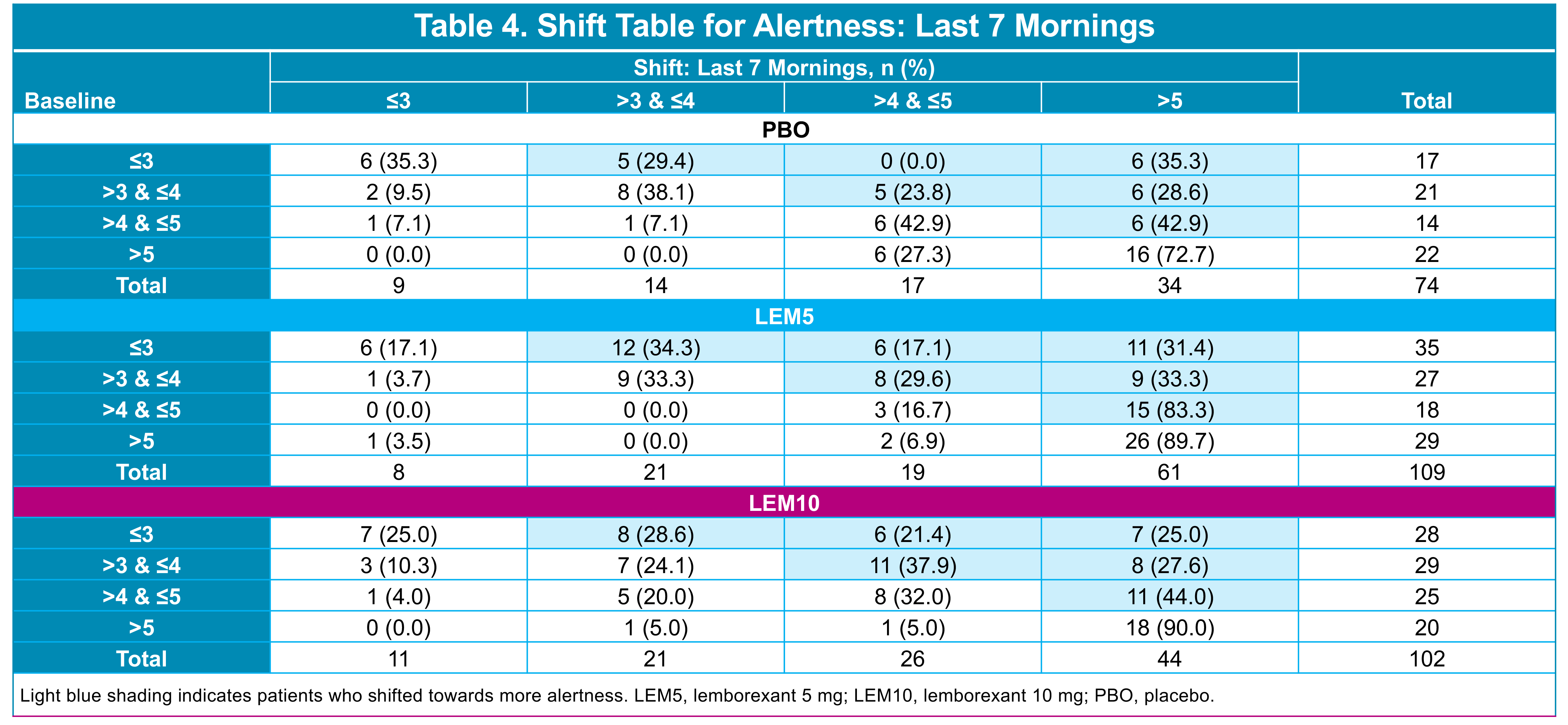
Morning Sleepiness/Alertness Rating








Process Mapping
Root Cause Analysis revealed:
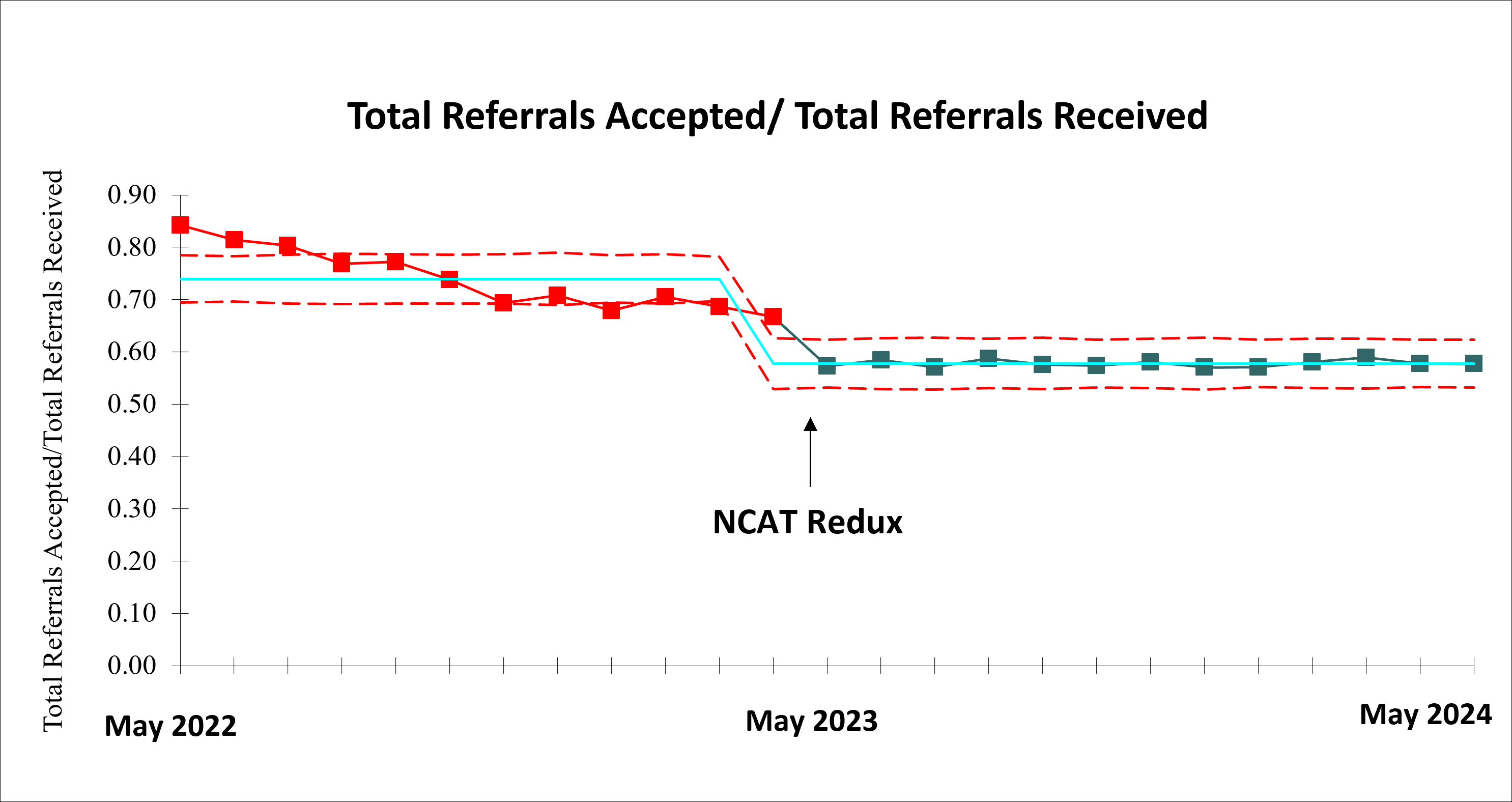
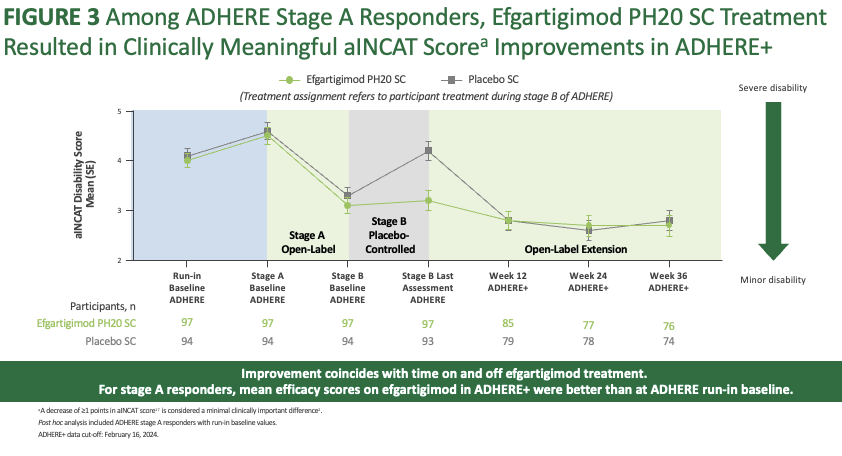
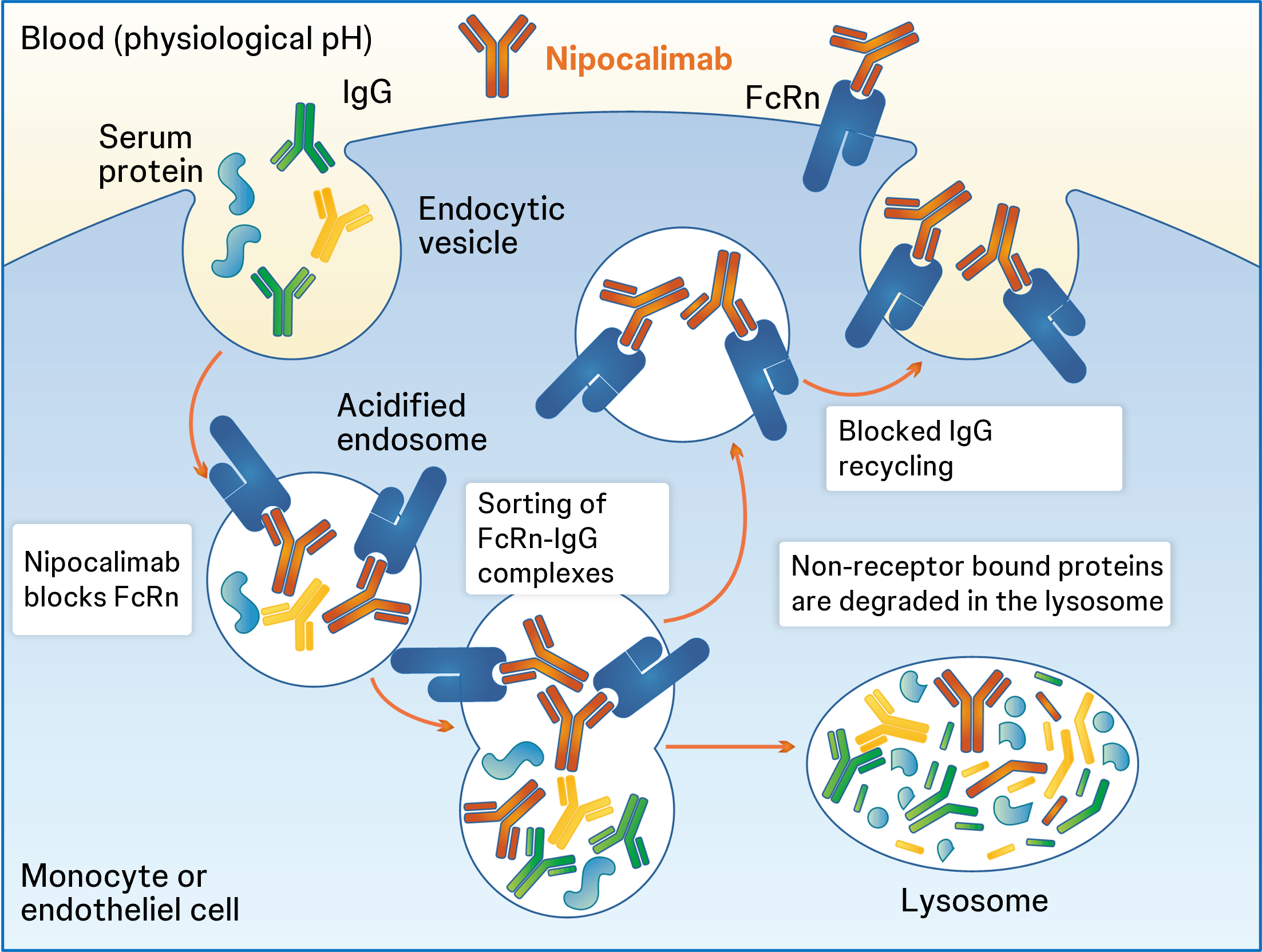
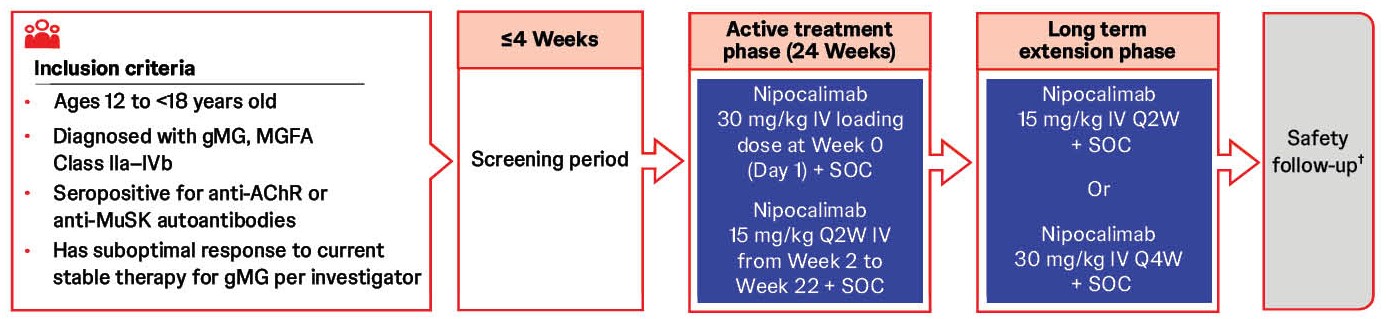
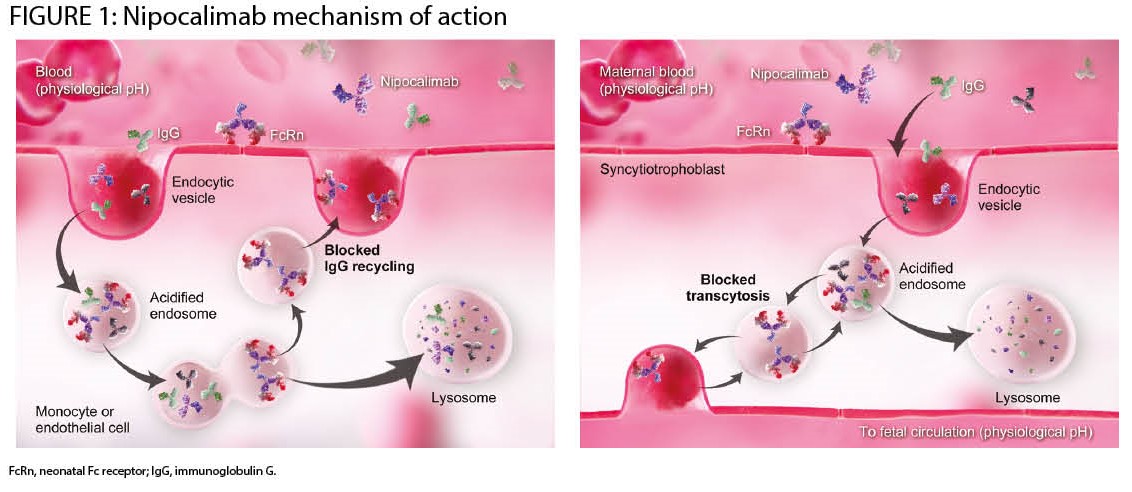
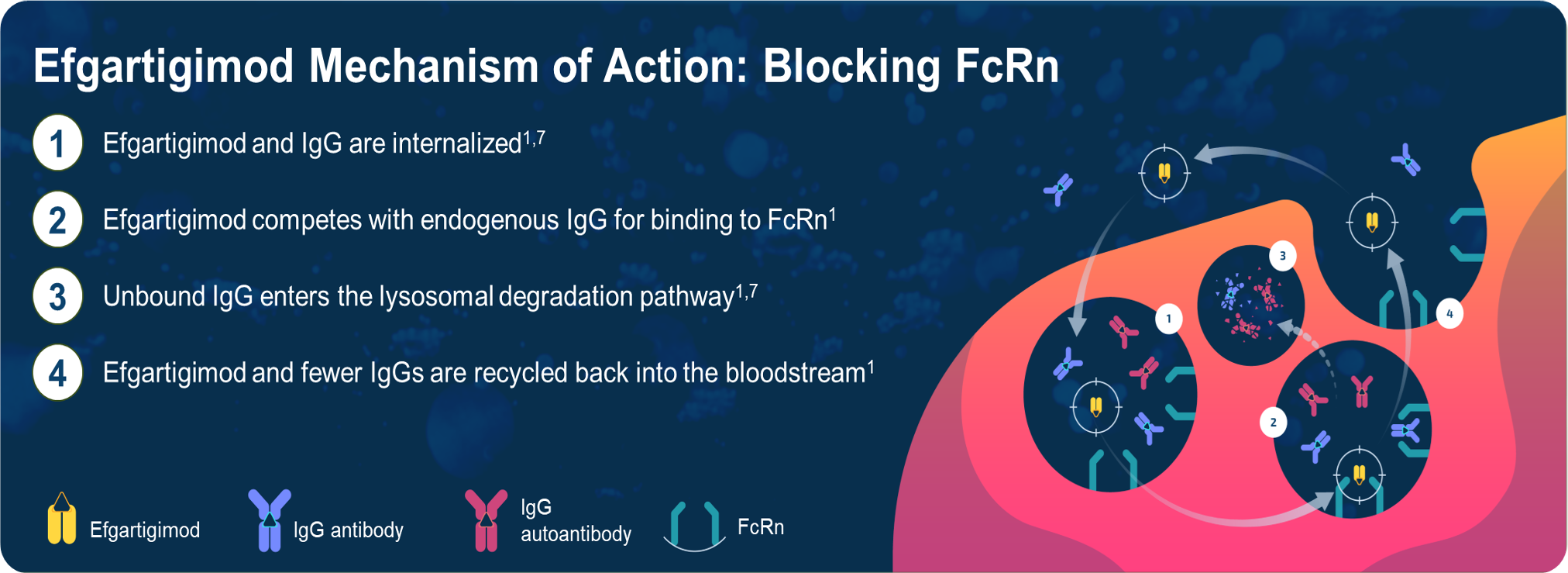
Efgartigimod PH20 SC is a coformulation of efgartigimod and recombinant human hyaluronidase PH20, which allows for rapid (30–90s single injection) SC administration10,11 (Figure 1)
METHODS
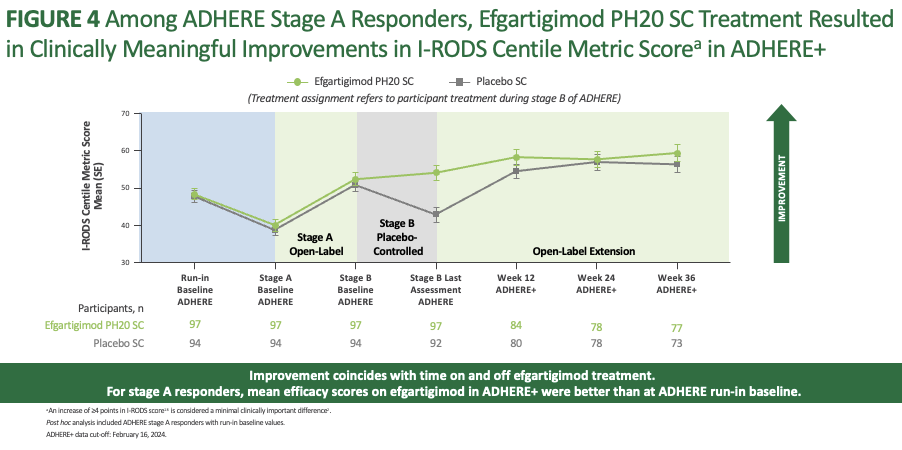
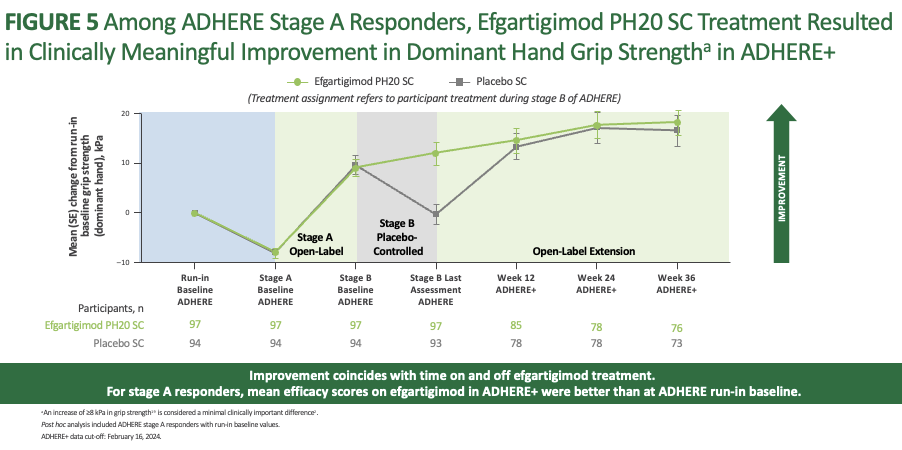
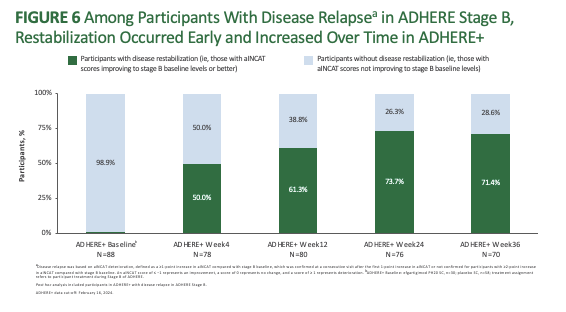
Baseline characteristics were similar across ADHERE Stages A and B
and ADHERE+
KEY TAKEAWAYS

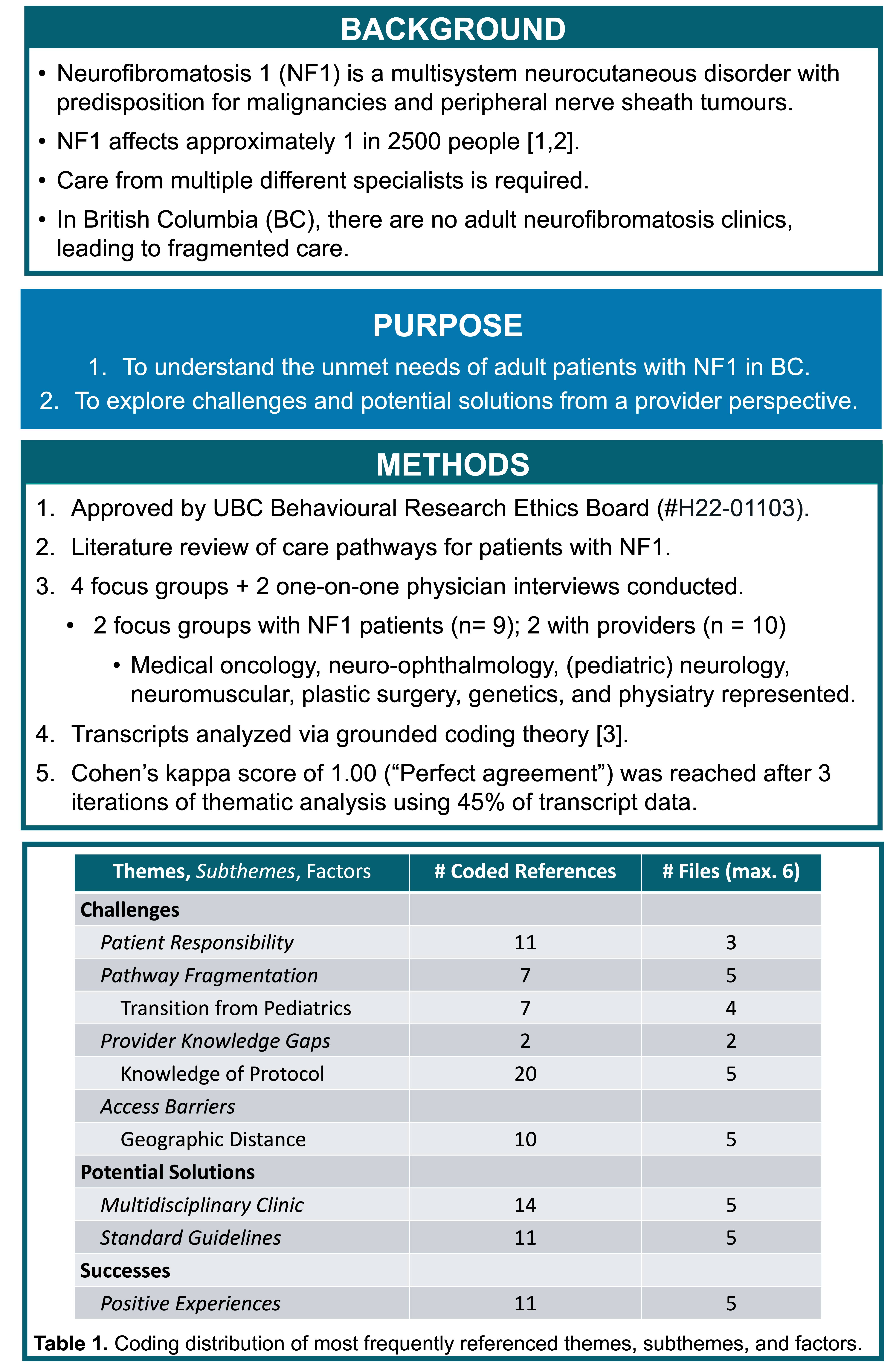

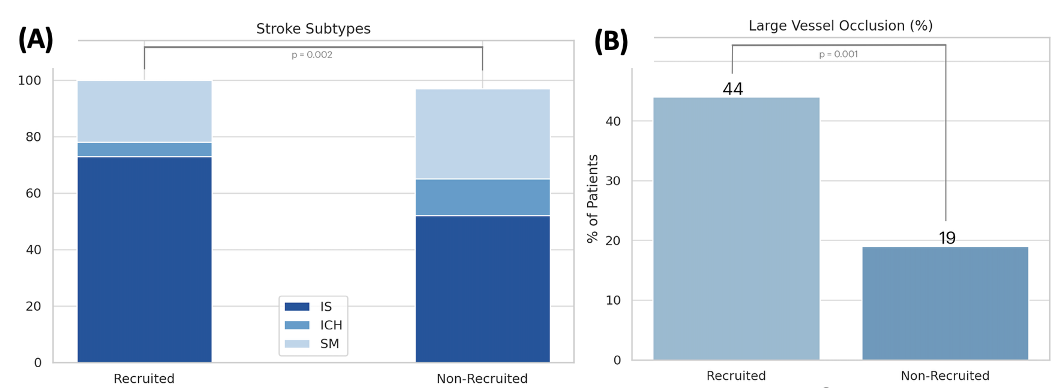
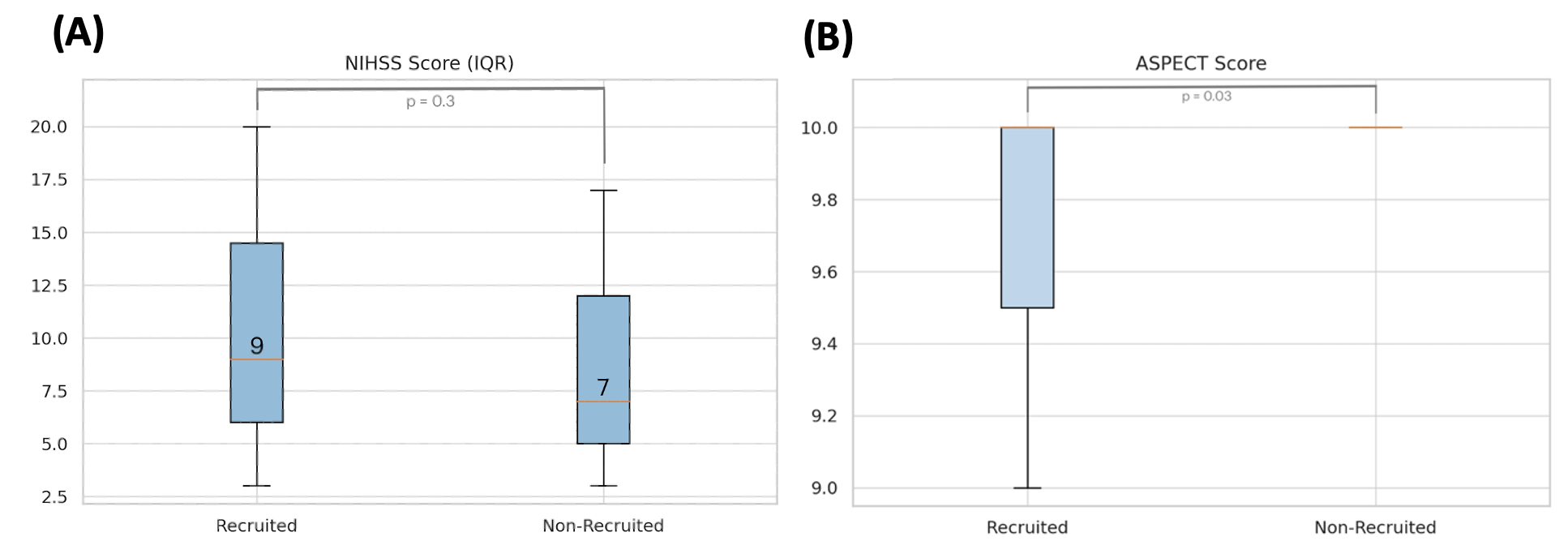
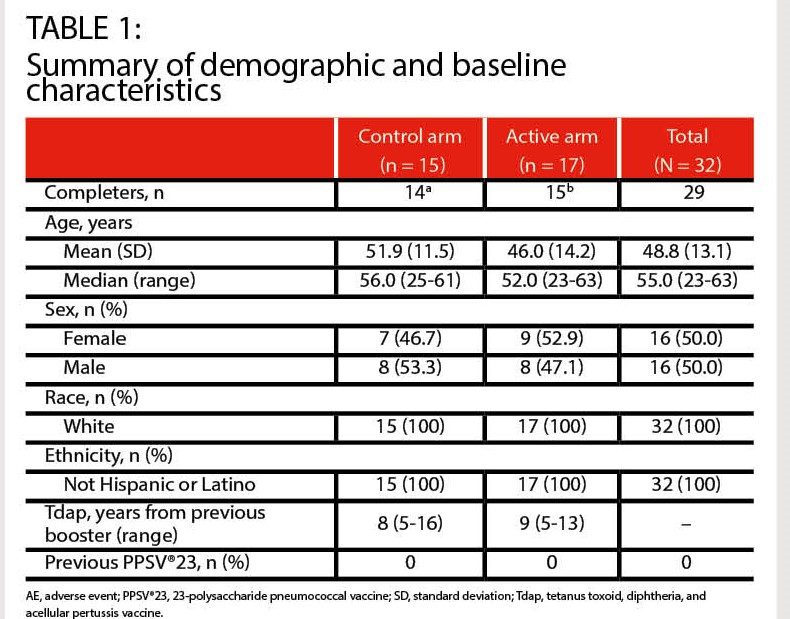
Table 1. Demographics and Clinical Characteristics of Patients Approached in ACT-TBI and CANCCAP
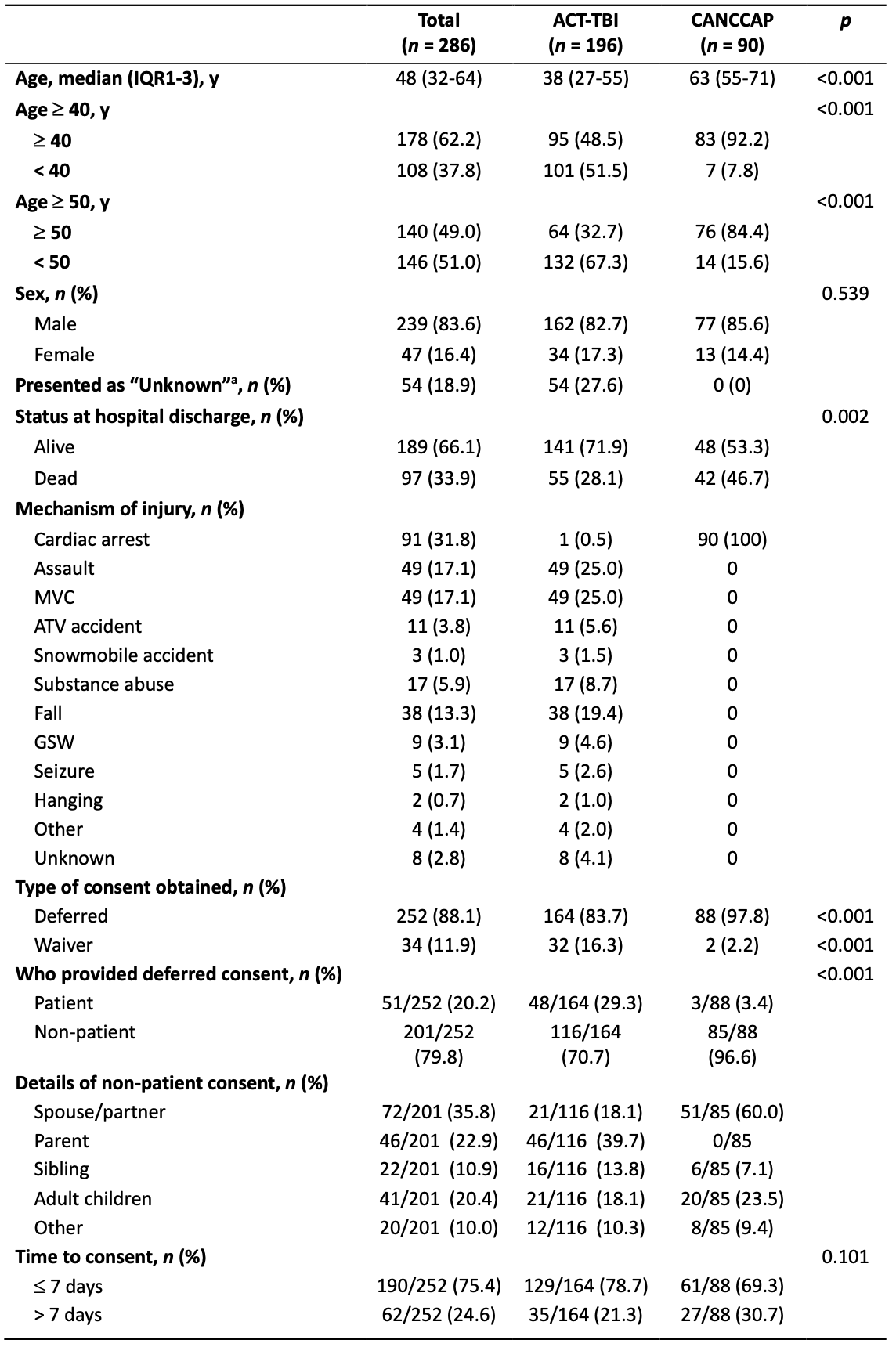
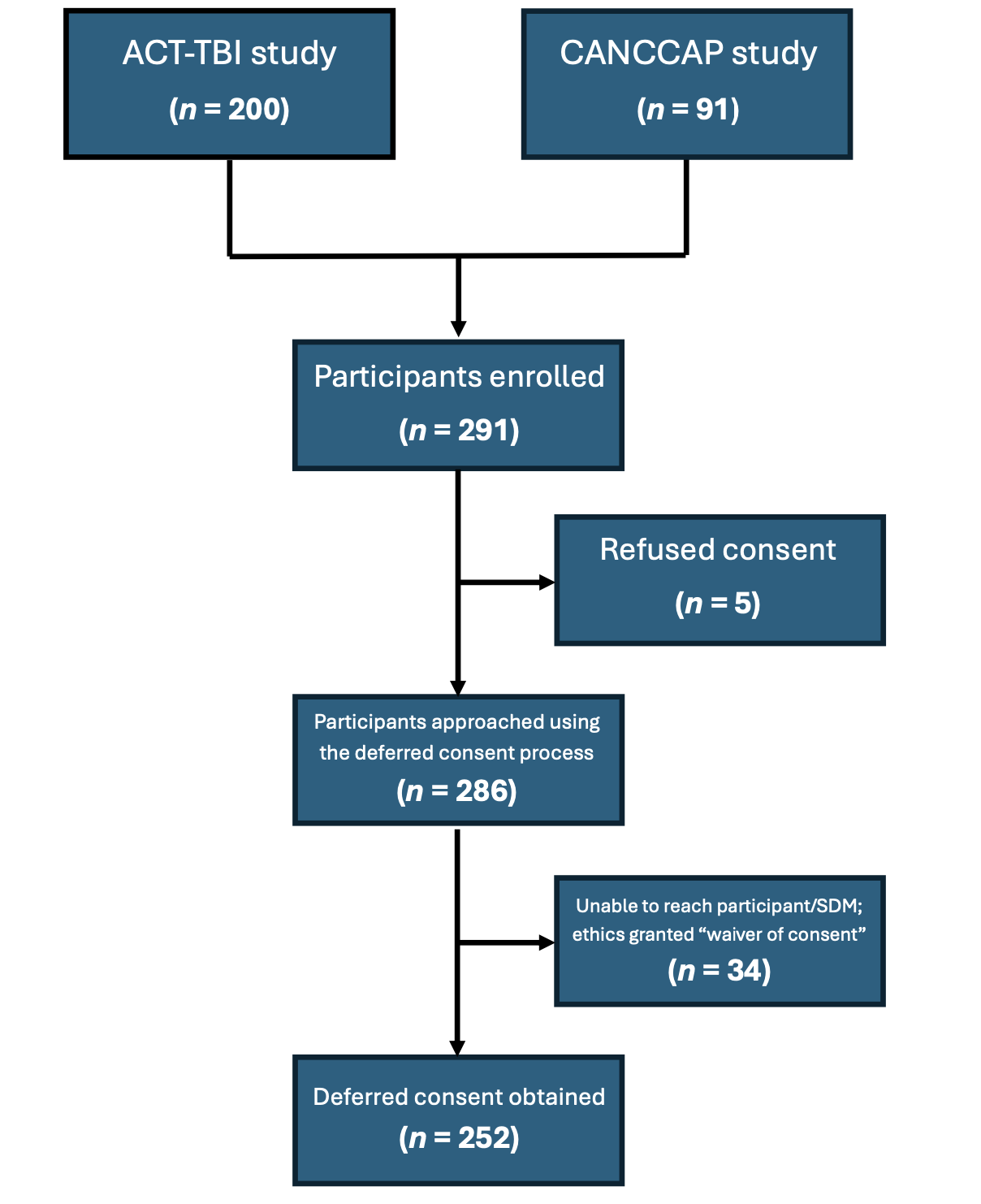
Table 2. Significant Differences Between ACT-TBI and CANCCAP studies
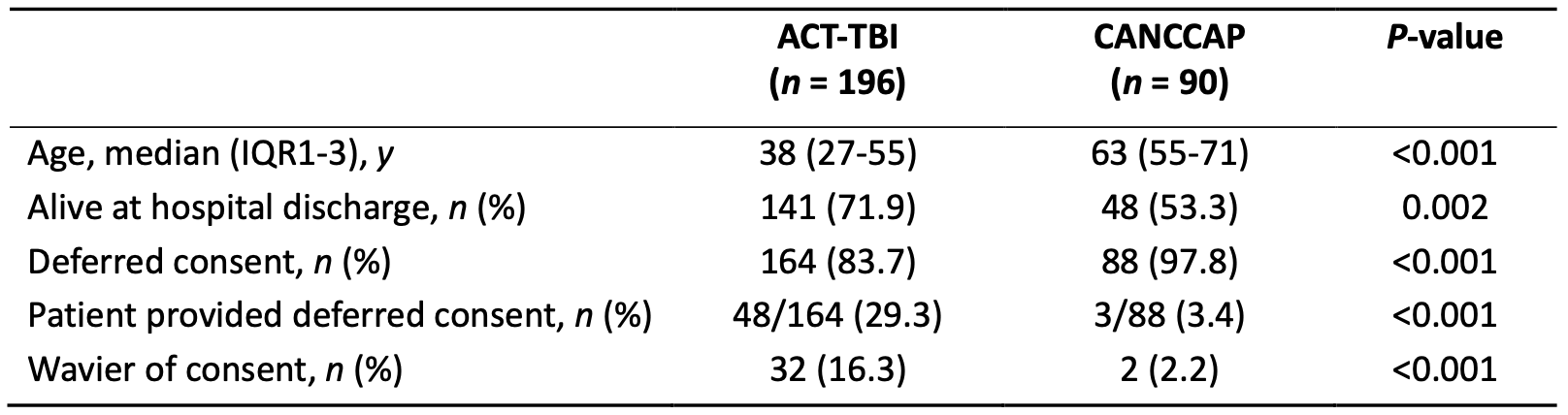
Table 3. Length of Time to Obtain Deferred Consent for Study Participants
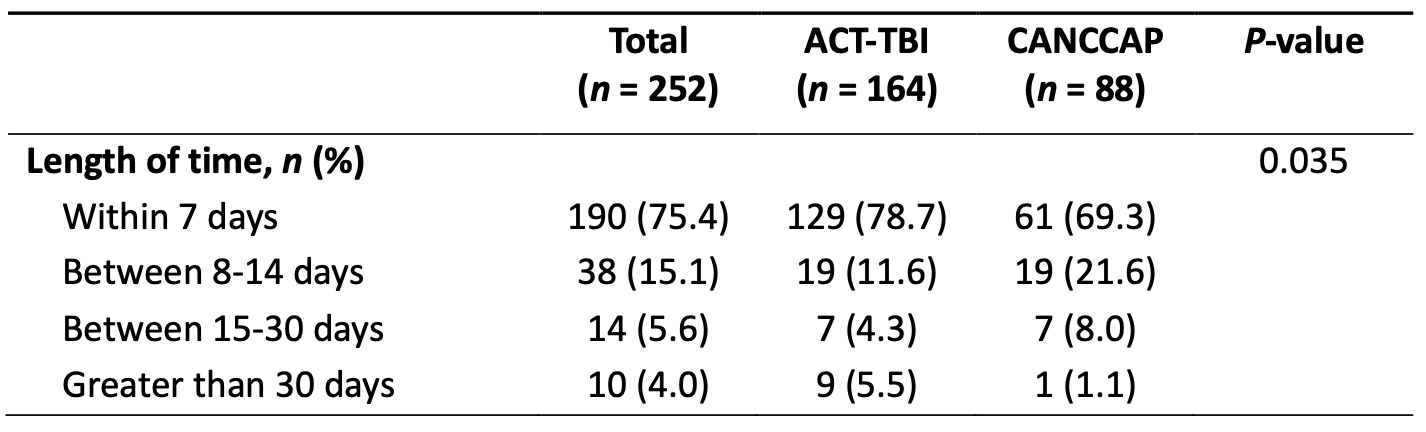
Table 4. Reasons for Delay in Obtaining Consent
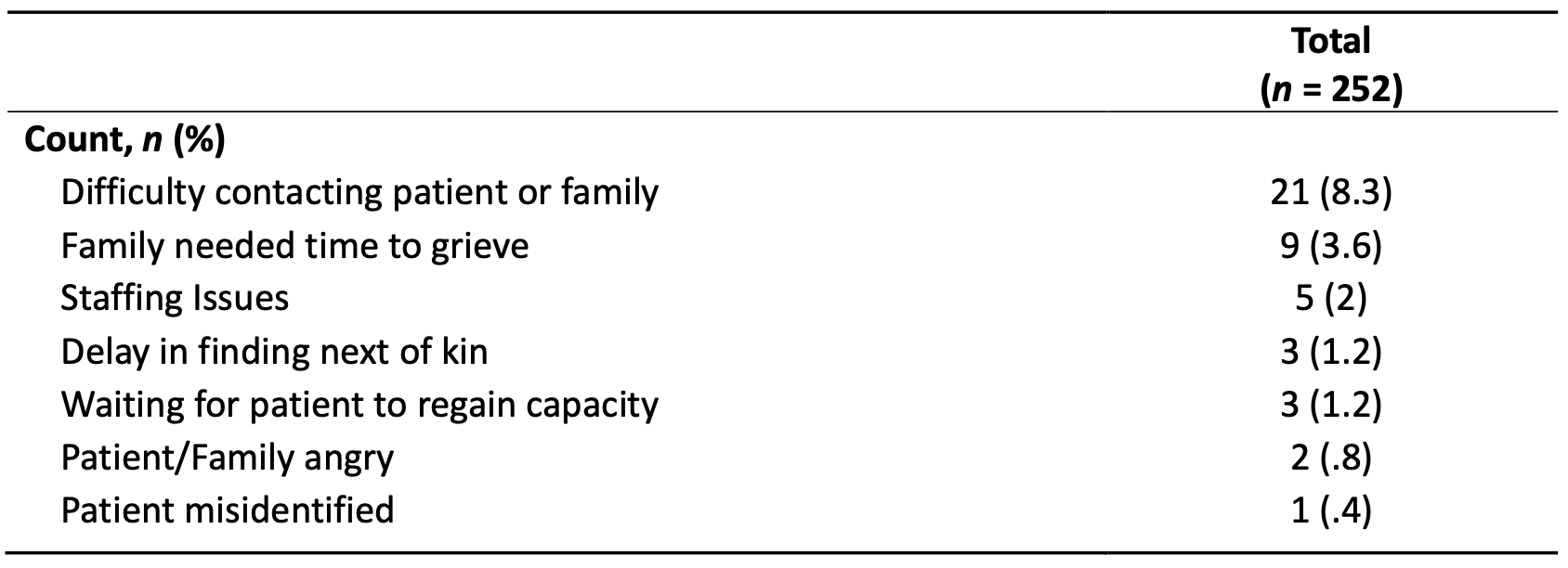
Table 5. Logistic Regression Analysis of Obtaining Deferred Consent

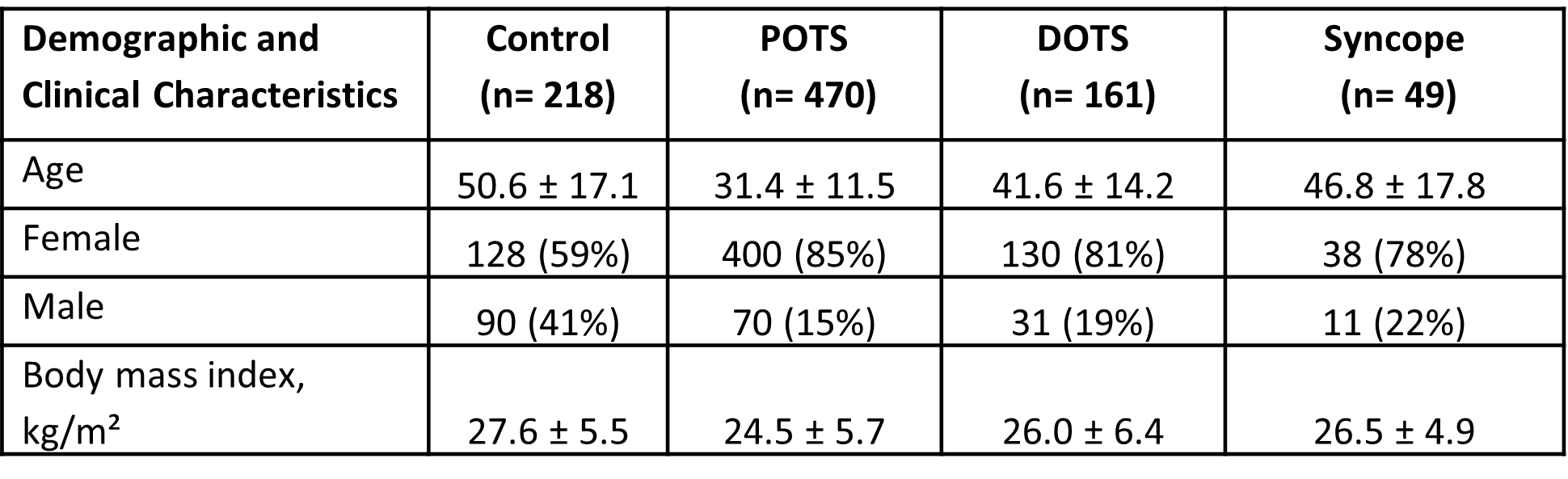
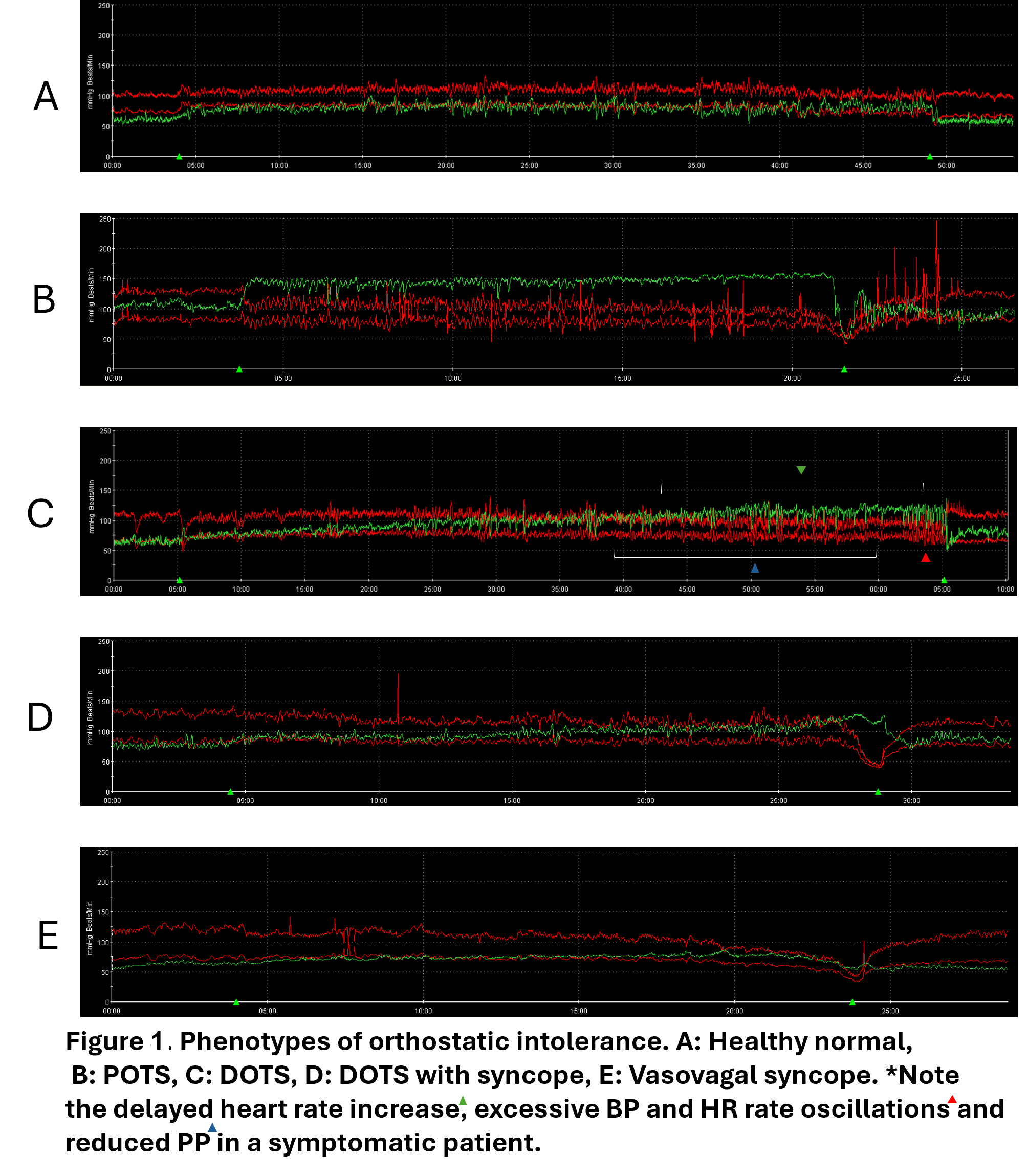
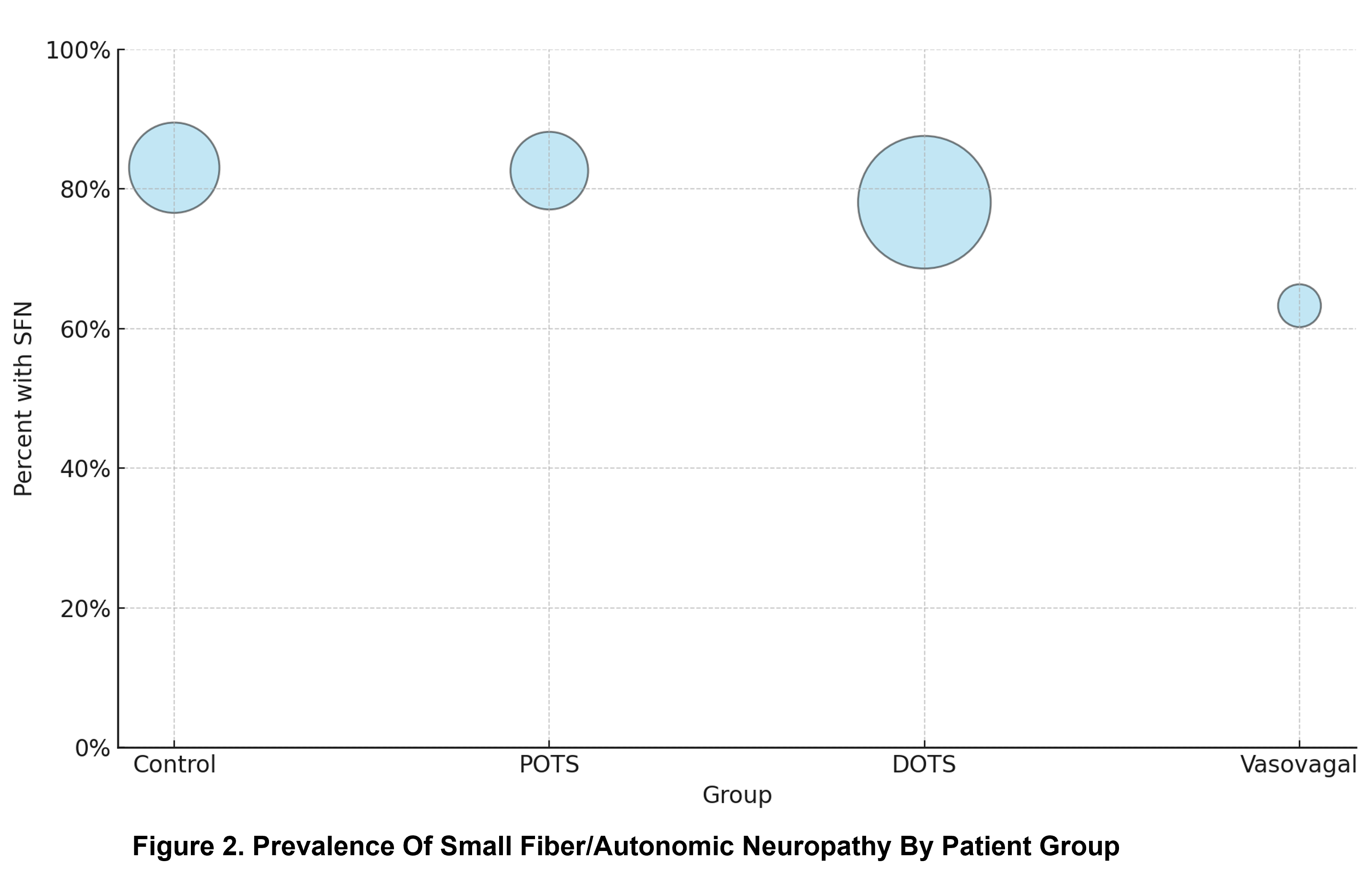
Postural Orthostatic Tachycardia Syndrome (POTS) is characterized by a sustained increase in heart rate (HR) of >30 beats per minute (bpm; >40 bpm in patients under 18 years of age) —often exceeding 120 bpm—within 10 minutes of standing or head-up tilt (HUT), in the absence of accompanying orthostatic hypotension (OH). However, some patients develop presyncopal symptoms after 10 minutes of upright posture in the absence of OH. This group remains poorly characterized.
OBJECTIVES
To characterize the clinical and laboratory features of early and delayed orthostatic intolerance (OI) in a large cohort of patients.
METHODS
Study design: Chart-based retrospective cohort study.
Population: Clinical histories and autonomic laboratory test results of 1,127 patients referred to the University of Alberta Autonomic Laboratory between 2010 and 2025 for assessment of orthostatic intolerance (OI) were reviewed. Symptoms suggestive of OI included lightheadedness, presyncope or syncope, palpitations, postural tachycardia, and/or shortness of breath. Patients were excluded if they had incomplete or artifact-laden data, a diagnosis of diabetes, underlying cardiovascular disease, or had used chronotropic or inotropic medications within five days of testing.
All patients underwent comprehensive autonomic testing, including:
Delayed OI criteria: Patients were considered to have abnormal delayed orthostatic tachycardia after the first 10 minutes during the HUT if they developed symptoms of OI and their HR increased by ≥40 bpm from baseline or reached ≥140 beats per minute.
RESULTS
SUMMARY
CONCLUSIONS


1. Kumar A, Misra S, Yadav AK, Sagar R, Verma B, Grover A, Prasad K. Role of glial fibrillary acidic protein as a biomarker in differentiating intracerebral haemorrhage from ischaemic stroke and stroke mimics: a meta-analysis. Biomarkers. 2020;25(1):1-8.
2. Paul JF, Ducroux C, Correia P, Daigneault A, Larochelle C, Stapf C, Gioia LC. Serum glial fibrillary acidic protein in acute stroke: feasibility to determine stroke-type, timeline and tissue-impact. Frontiers in Neurology. 2024;15.
3. Yue JK, Yuh EL, Korley FK, Winkler EA, Sun X, Puffer RC, et al. Association between plasma GFAP concentrations and MRI abnormalities in patients with CT-negative traumatic brain injury in the TRACK-TBI cohort: a prospective multicentre study. Lancet Neurol. 2019;18(10):953-61.
- We retrospectively analyzed the Canadian OPTIMISE registry which included data from 20 comprehensive stroke centers across Canada between January 1, 2018, and December 31, 2022.
- We compared treatment metrics and early outcomes between two groups: 1) patients evaluated by telemedicine (TM) and 2) patients evaluated in person (non-TM) at the PSC prior to CSC transfer.
- We used mixed-effects logistic regression models to compare the likelihood for symptomatic intracerebral hemorrhage (sICH), good functional outcome (defined as a modified Ranking Scale [mRS] score of 0-2), or all-cause mortality at 90 days between the two groups.
- All models were adjusted for predefined confounders (age - baseline ASPECTS - baseline NIHSS - onset to groin puncture time - final TICI - anesthesia type - IV-tPA - carotid stenting - participating centre).
- We included 3289 patients who were transferred from a PSC to a CSC: 888 TM and 2401 non-TM.
- There were no major differences in baseline characteristics, including IV thrombolysis administration, though the TM group included more men and a slightly lower baseline ASPECTS.
- In unadjusted analyses, outcomes of successful recanalization (TICI≥ 2b) and functional outcome were similar between TM and non-TM. However, we found that TM patients had longer onset-to-puncture times (355 vs 310 minutes, p<0.001), higher sICH rates (6.8% vs 3.3%, p<0.001) and higher risk for all-cause mortality at 90 days (39.6% vs 29.4%, p<0.001). (Table 1)
|
No telemedicine |
Telemedicine |
P-value |
|
|
Onset needle (Median [IQR]) |
131 [99,184] |
139 [98,187] |
0.280 |
|
Door needle (Median [IQR]) |
31 [23,42] |
34 [29,39] |
0.418 |
|
Onset puncture (Median [IQR]) |
310 [224,485] |
355 [255,526] |
<0.001 |
|
Door puncture (Median [IQR]) |
39 [21,70] |
37 [24,58] |
0.026 |
|
Puncture reperfusion (Median [IQR]) |
26 [17,40] |
25 [16,36] |
0.100 |
|
Succesful reperfusion (TICI≥2b) |
1960 (84.8%) |
736 (85.7%) |
0.562 |
|
sICH |
79 (3.3%) |
60 (6.8%) |
<0.001 |
|
Discharge mRS 0-2 |
300 (20.9%) |
188 (23.4%) |
0.172 |
|
Discharge mortality |
271 (18.9%) |
121 (15.1%) |
0.022 |
|
90-day mRS 0-2 |
670 (39.5%) |
185 (34.8%) |
0.050 |
|
90-day mortality |
524 (29.4%) |
216 (39.6%) |
<0.001 |
- In adjusted analyses (mixed effect logistic regression model), there were no differences for sICH, 90-day mRS≤2 and all-cause mortality at 90 days between TM and non-TM patients. (Table 2)
|
|
*aOR |
95% confidence interval |
|
sICH |
1.803 |
0.82 – 3.99 |
|
90-day mRS≤2 |
0.813 |
0.51 – 1.30 |
|
90-day mortality |
1.384 |
0.86 – 2.24 |
- Patients transferred to a CSC for EVT first evaluated by TM had similar characteristics to those evaluated in person at the PSC, but longer treatment times and worse outcomes.
- The higher risk for unfavourable outcomes did not persist after adjustment for confounders, including treatment time.
- It is likely that TM patients had longer treatment delays because TM is more commonly used for more distant and rural sites, contributing to a higher risk of worse outcomes.
- There is a need for quality improvement initiatives to optimize the workflow of patients receiving telemedicine consultation prior to CSC transfer for EVT from more remote PSCs.
References:
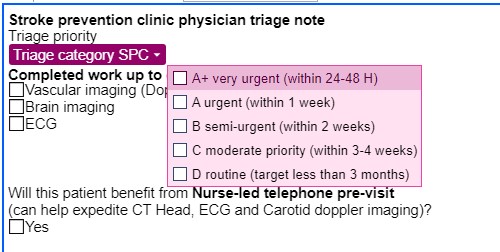
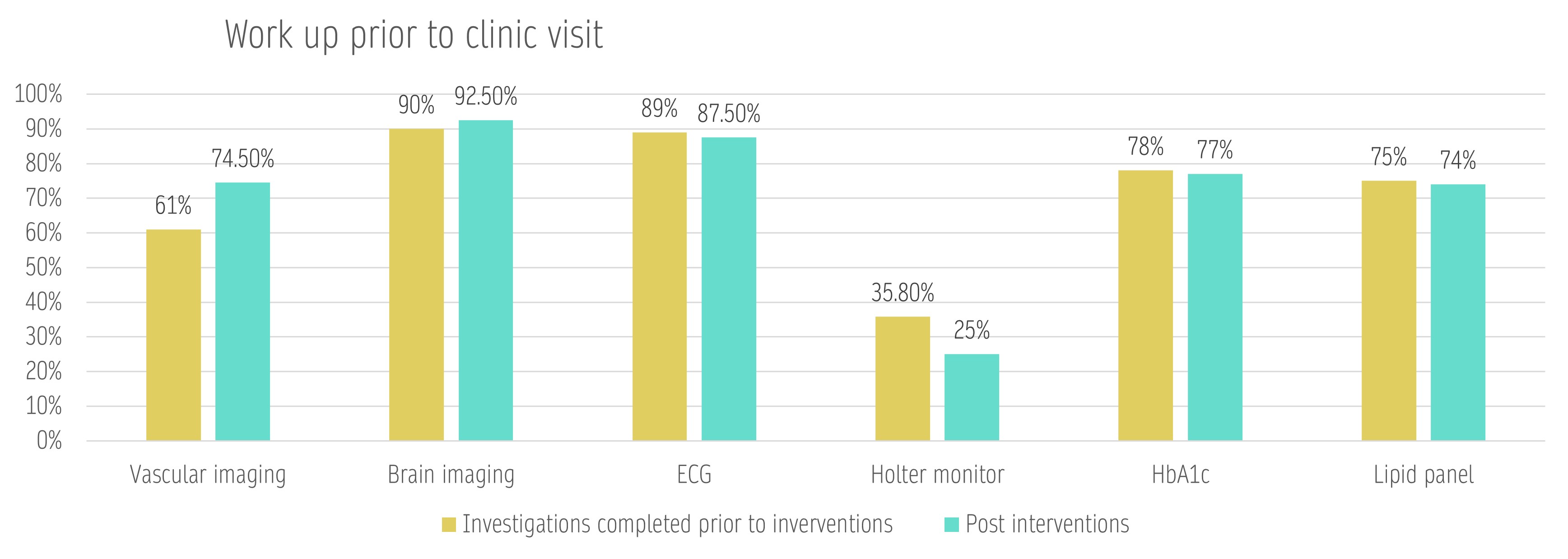
Timely access to a Stroke Prevention Clinic (SPC) after a stroke or TIA is critical. Stroke specialists rely on specific investigations to assess vascular risk and guide secondary prevention. If these tests aren't done before the first visit, treatment may be delayed, and more follow-up visits required, straining limited clinic capacity
Objective: This project at the University of Alberta Hospital SPC aimed to streamline the referral process and preliminary work-up by ensuring key investigations are completed before the first appointment to reduces follow-ups and free up slots for more new patients.
For the purpose of this project we have defined “bare minimum Investigations” as:
| Baseline data |
Post intervention | Baseline data |
Post intervention | ||
|
Number of all new referrals seen in the clinic during the surveillance period |
320 | 453 | Patients who completed all minimum investigations | 55% (109) | 65% |
|
Number of patients who met inclusion criteria |
198 | 200 | Completed brain imaging | 90% | 92.5% |
| Age |
67±19.5 years |
68±13.4 years | Completed vascular imaging | 61% | 74.5% |
| Sex | 50% female | 46% | Completed EKG | 89% | 87.5% |
| True vascular events | 64.6% | 61.3% | Completed Holter | 35.8% | 25% |
| Referral source |
62% - ED, 26% from PCP, the rest from subspecialists |
66.5% - ED, 21% from PCP, the rest from subspecialists |
HbA1c of fasting BG | 78% | 77% |
| Triage categories |
A+ 3%, A 13.75, B 31.8%, C 32.8% D (routine) 18.7%
|
A+ 3%, A 7%, B 30%, C 32% |
Lipid panel | 75% | 74% |
Clinic staff survey: 100% of respondents indicated that the pre-visit was beneficial for patient care; the overall experience with the intervention was rated at 4.3 out of 5.
Nurse-led pre-visit was shown to be an effective tool for completing vascular imaging. Further work needs to be done to improve cardioembolic stroke workup (Holter, Echo). Pre-visit can be considered for future use in the stroke prevention clinics if enough nursing staff are consistently available. It is rolled out for use on a regular basis at UAH SPC in May 2025.

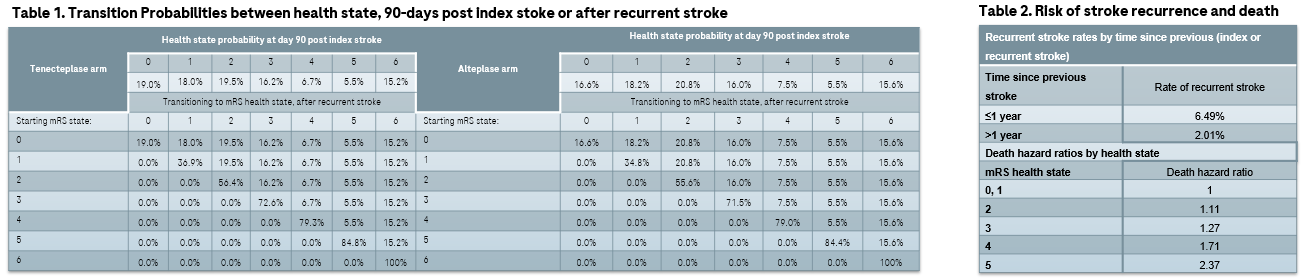
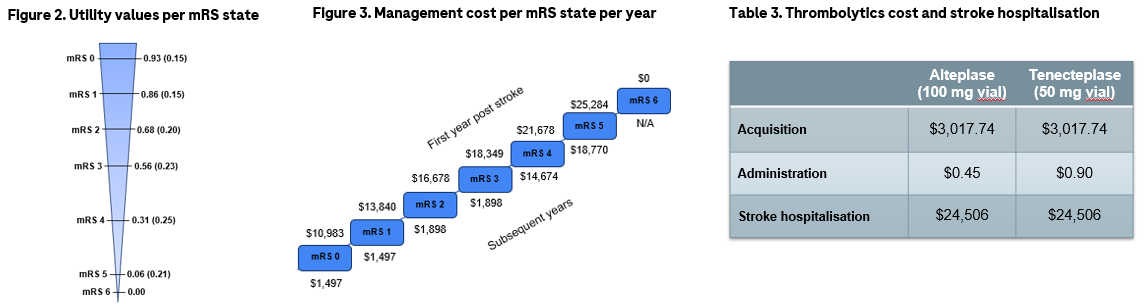
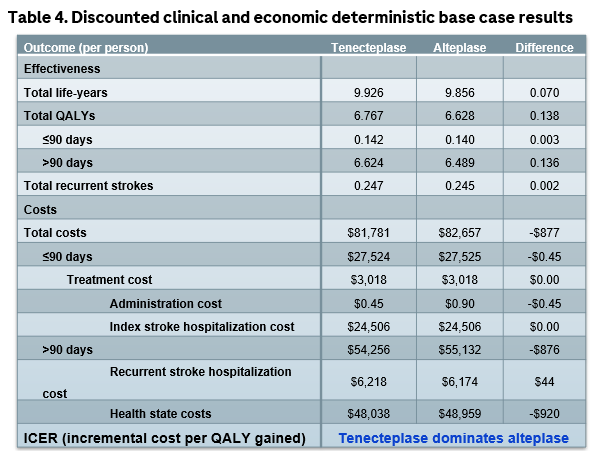
This pharmacoeconomic analysis, which leverages the same structure as many stroke models, is the first to show that tenecteplase is cost-effective in AIS patients within 4.5 hours of symptom onset, from a Canadian health care payer perspective. Sensitivity analysis confirm the robustness of this finding.
The analysis incorporates several economic and clinical inputs from Canadian sources, including the AcT trial, which reinforces its external validity and applicability to the hospital context from this country.
Additional QALYs and cost savings were mostly generated by the 2.1% difference in mRS score of 0-1 in favor of tenecteplase in the AcT trial. Though this was a non-inferiority design, evidence from a recently published meta-analysis (which included 16 randomized controlled trials)7 found tenecteplase to be associated with statistically significant better 90-day excellent neurological recovery (i.e. mRS score 0-1), which supports the base case assumption.
In conclusion, though all the benefits for the health care system could not be quantified and integrated in the model (no infusion pump needed, simplified administration protocol versus alteplase which reduces the time for setting up for the administration, may decrease dosing errors, expedite / facilitate the transportation of the patient to comprehensive stroke center for thrombectomy), this economic study, along with the accumulating clinical evidence, could be helpful to support decision-making regarding the possible addition of tenecteplase on hospitals’ formularies and use in clinical practice.


Introduction
Absence epilepsy is a common epilepsy syndrome in children. This can have a negative impact on the cognitive abilities of preschool and school-age children. The objective was to study in the Guinean context, the epidemiological, clinical, electrophysiological, therapeutic and evolutionary aspects of this syndrome.
Participants and methods
The study included all children diagnosed with absence epilepsy based on evidence obtained from history, clinical, and electroencephalogram (EEG) recording results.
Results
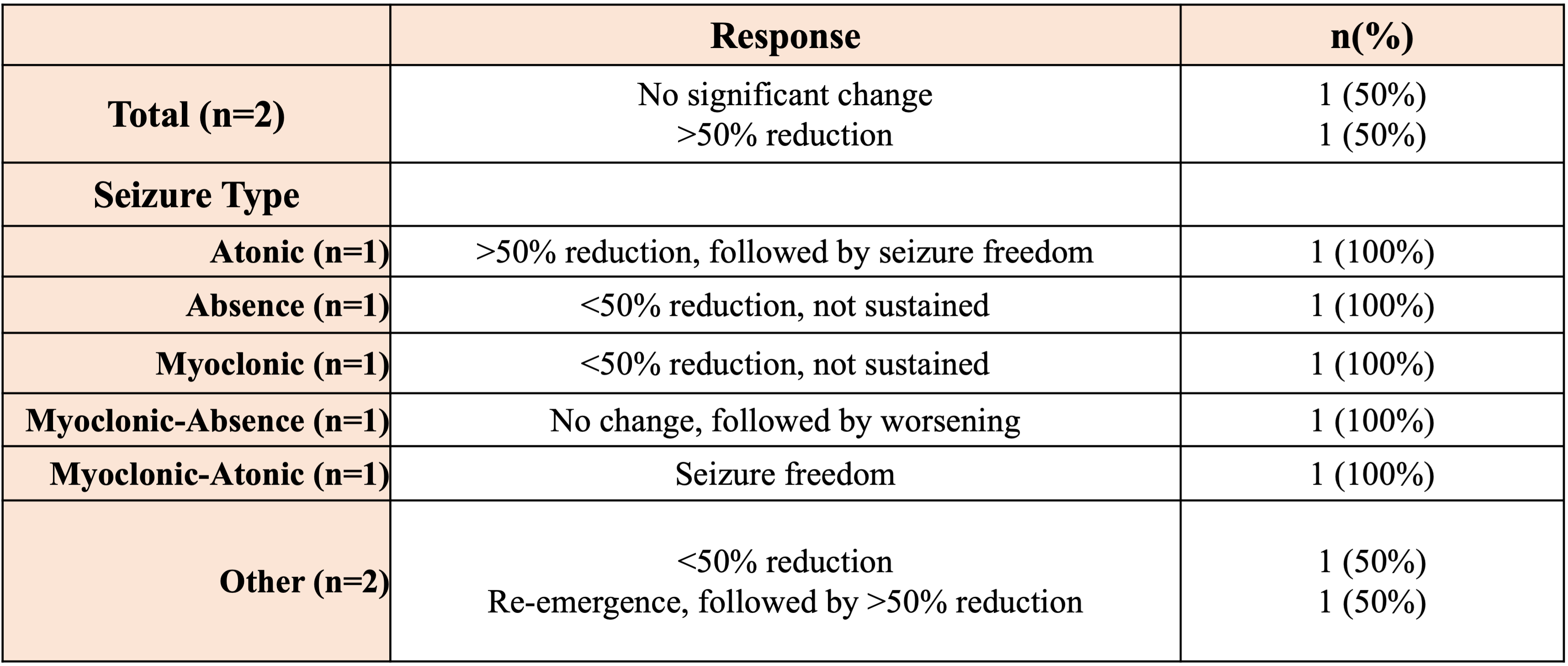
The cohort was made up of 41 girls and 28 boys with a sex ratio (F/M) equal to 1.46. The mean age was 8 ± 2 years with extremes of 2 and 14 years. Clinically, simple absences were observed in 42.02% of cases. The components : tonic was associated in 11.59%, clonic in 10.14%, atonic in 13.04%, automatisms in 15.94% and vegetative in 7.25%. EEG was typical in 75.36%. As monotherapy, sodium valproate was used in 92.75% and ethosuximide in 2.9%. Valproate/lamotrigine dual therapy was carried out in 2.9% of cases. The evolution was marked by a remission of seizures in 85.51%. During follow-up, the appearance of tonic-clonic convulsions was noted in 4.3%, myoclonus in 2.9%, a combination of myoclonus and tonic-clonic convulsions noted in 4.3%.
Conclusion
Effective and efficient collaboration between stakeholders is essential for the best overall management of this syndrome with serious cognitive repercussions in children, particularly between pediatricians, pediatric neurologists, epileptologists, neurophysiologists, the children's parents and the health authority.
Keywords: Absence epilepsy, children, EEG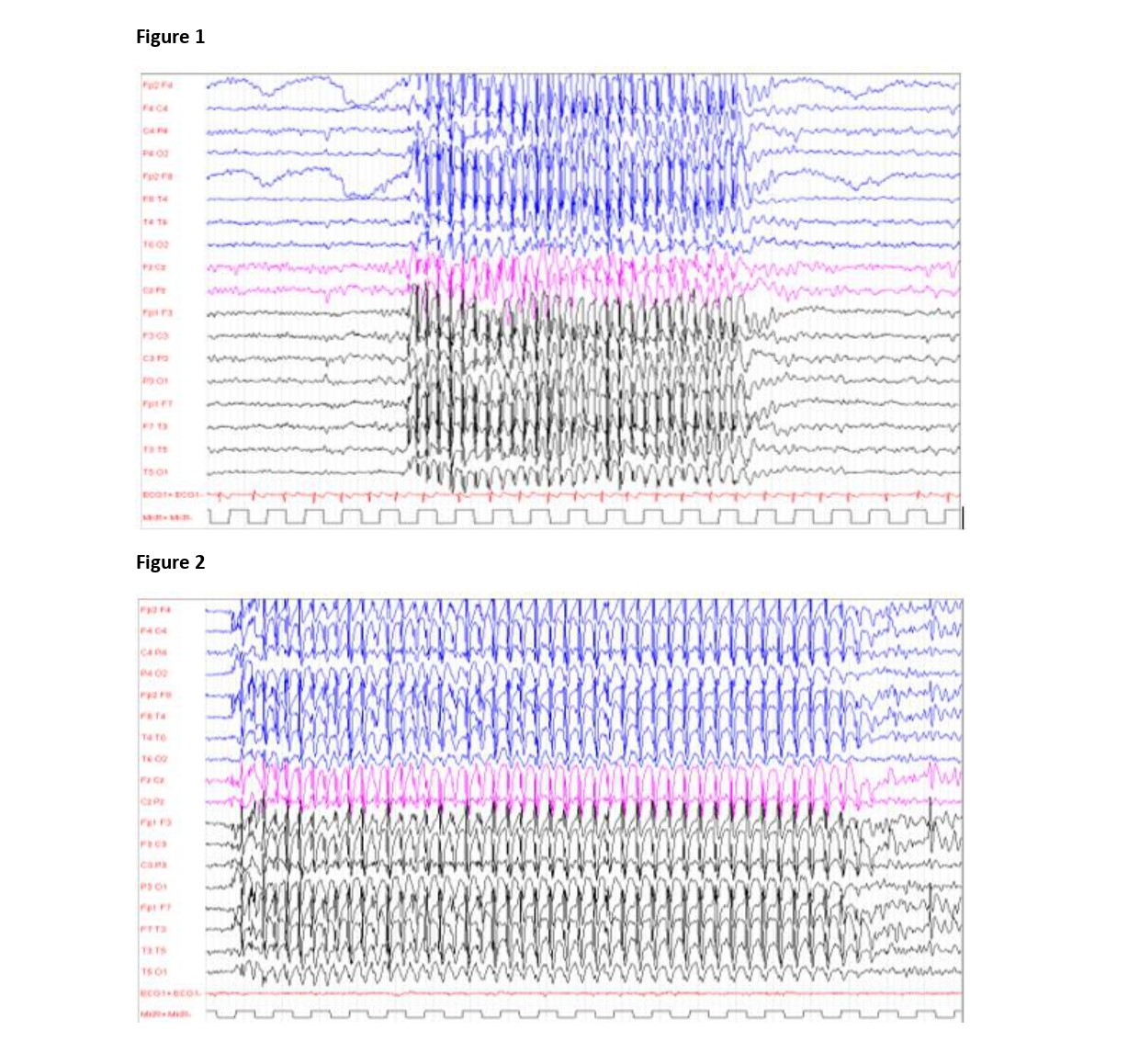
Figure 2 : Trace of absence epilepsy marked by a brief spike-wave discharge at 2-3 c/sec lasting approximately 9 seconds in the period with abrupt onset and abrupt end.
Figure 3 : Trace of absence epilepsy marked by a long paroxysmal discharge of spikes and waves at 3-5 c/sec lasting 17 seconds during the period with sudden onset and gradual end.
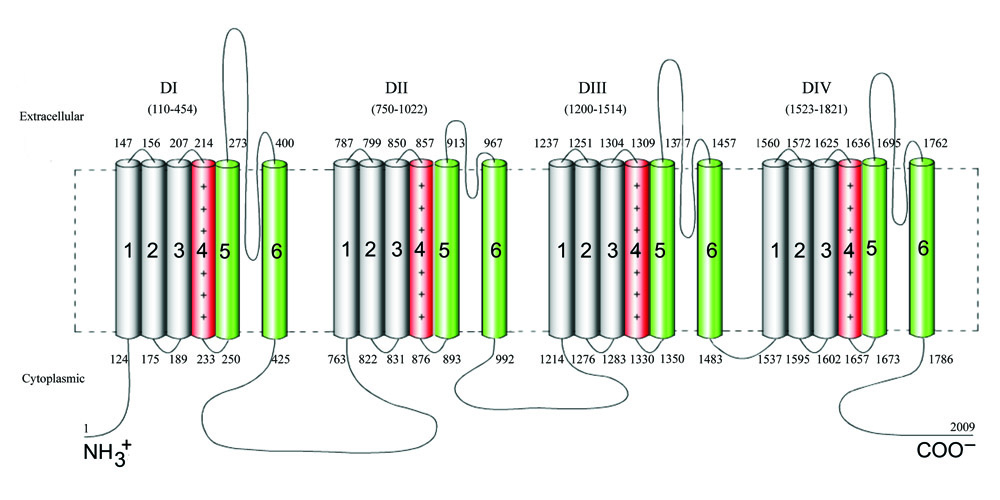
Variants in SCN1A, which encodes the alpha-1 voltage-gated sodium channel subunit, cause diverse pathologies [1-3]:
Pathogenic variants in SCN1A are typically heterozygous, de novo, and haploinsufficient. However, rare cases of bi-allelic SCN1A variants with autosomal recessive inheritance have been reported in conjunction with DS and other phenotypes. Here, we report two cases of biallelic SCN1A variants with divergent epilepsy phenotypes and review all 16 previously published cases [2, 4-10].
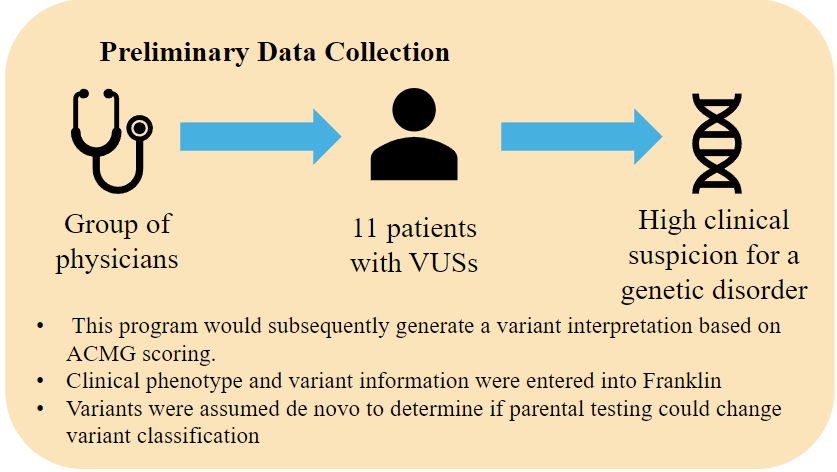
A retrospective chart review was performed with informed written consent in accordance with the research ethics board at McMaster University. Variants were classified by the American College of Medical Genetics and Genomics (ACMG) criteria [11].
A systematic literature review identified previous cases. A data search was performed using the terms “SCN1A” “Dravet” “homozygous OR homozygosity” and “recessive inheritance” in PubMed, Google Scholar, and Scopus until October 24, 2024 and 16 cases from 10 different families were identified [2, 4-10].
ID: 10-year-old male, no family history of seizures.
Epilepsy: Onset at10 months with afebrile bilateral tonic-clonic seizures (BTCs). EEG showed events associated with semi-rhythmic generalized theta. No seizures and normal EEG for four years on levetiracetam and phenobarbital. Seizures recurred at 5 years after medications weaned, repeat EEG demonstrated left temporal epileptiform discharges, and now has been seizure free on valproate for the five years since.
Neurological assessment: Normal exam except for macrocephaly and soft dysmorphic features, MRI showed benign external hydrocephalus that later resolved. Diagnosed profound global developmental delay (GDD) and autism spectrum disorder (ASD).
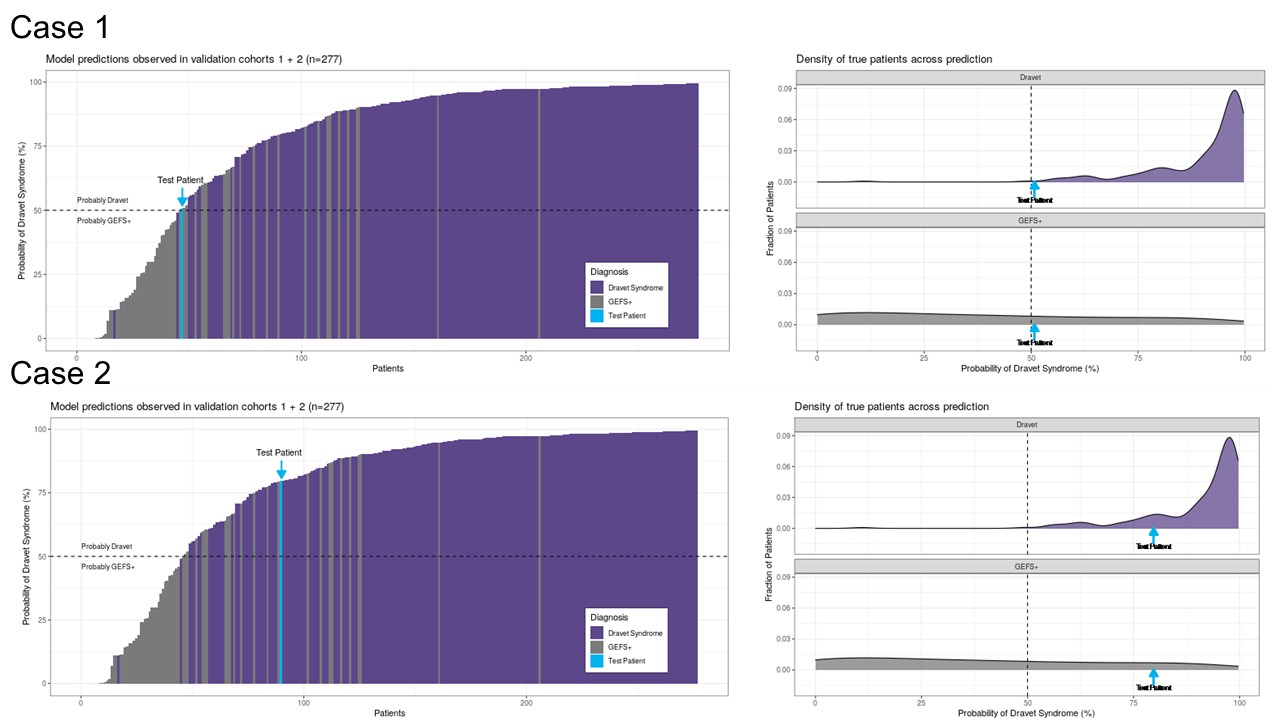
Genetics: Homozygous SCN1A variant, c.1676T>A, (p.Ile559Asn) inherited from asymptomatic parents, VUS per ACMG. It is absent from controls (gnomAD), predicted to be damaging by multiple algorithms (i.e., SIFT, polyphen-2, mutation taster), Grantham score 149, REVEL score 0.778, and DS risk 50.79% per SCN1A-Epilepsy Prediction Model [12].
ID: 7-year-old female, family history of febrile seizures
Epilepsy: Hemi-clonic seizures with onset at 6 months, occurring generally with but sometimes without fever, and complicated by recurrent status epilepticus. EEG was normal at 14 months. Seizures became controlled at 3 with maximized clobazam, phenobarbital, and valproate. Seizures wortsened at 3.5 years but have remained controlled for four years with the addition of stiripentol. Repeat EEGs demonstrated background slowing.
Neurological assessment: Notable for progressive ataxia, spastic gait, and sensorineural hearing loss. She is non-dysmorphic. MRI demonstrated a small left hippocampus with subtle T2 hyperintensity. She has moderate GDD.
Genetics: Homozygous previously reported pathogenic variant in SCN1A, c.4970G>A, (p.Arg1657His). Her parents and brother are hetrozygous and have a history of simple febrile seizures, but no other features of Dravet syndrome; she did recieve a diagnopsis of DS. The SCN1A-Epilepsy Prediction Model gave a risk of DS of 79.75% [12].
Result: 18 biallelic SCN1A variants with epilepsy
Diagnosis: 9/18 (50%) DS, 6/18 (33%) GEFS+, 3/18 (17%) afebrile epilepsy and GDD.
Seizures: 15/18 (83%) febrile, 9/18 (50%) status epilepticus, 14/18 (78%) BTC, 6/18 (33%) myoclonic.
Seizure onset: 3 – 19 months (mean = 7.3)
Treatment: 7/18 (39%) controlled on one antiseizure medication (ASM), 10/18 (56%) multiple ASMs, 1/18 (6%) untreated. 7/9 (78%) successful polypharmcy included valproate, 5/9 (56%) clobazam, 4/9 (44%) levetiracetam, and 4/9 (44%) topiramate.
Development: 5/18 (28%) normal,13/18 (72%) delayed. 2/18 ASD. 11/18 (61%) motor dysfunction.
Variants: 3/4 (75%) with variants in the pore-forming domain had DS, as well as 2/2 patients (100%) with variants in other transmembrane segments, compared to 3/7 intracytoplasmic variants (43%), and 1/5 variants (20%) in the S5-S6 linker.
1. Presentations of bi-allelic SCN1A-related epilepsy are varied, ranging from intact to normal development with easily controlled to refractory seizures. Many but not all cases evoke DS or GEFS+.
2. There may be worse clinical outcomes for truncating than missense variants and for variants in the pore/voltage sensor domains than others.
3. Valproate and clobazam may be effective.

Rationale
Research assistant could then notify the clinical team
References
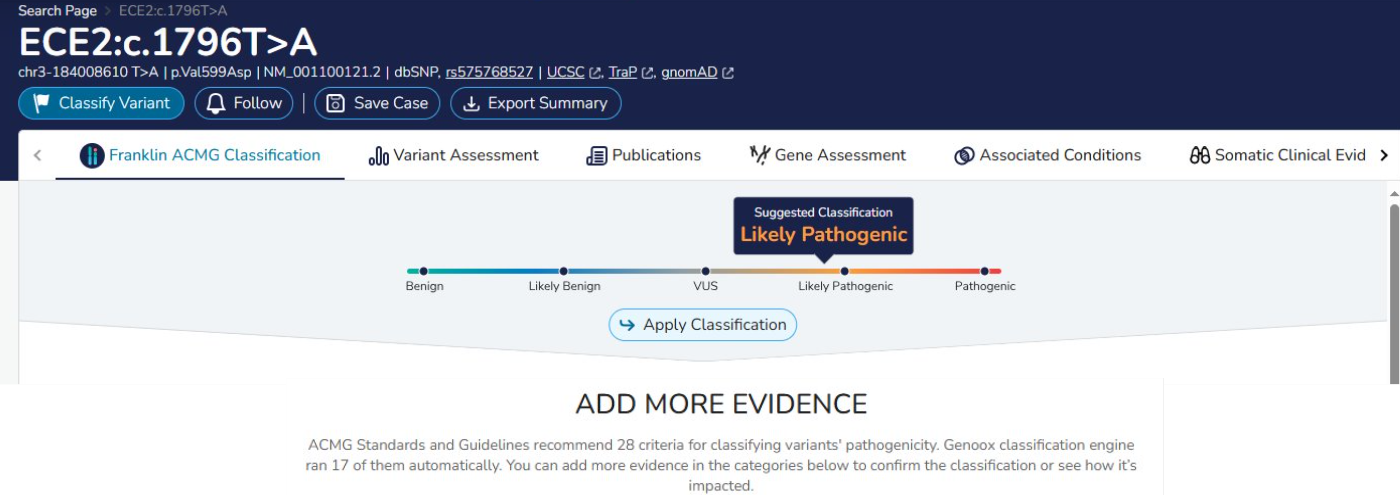
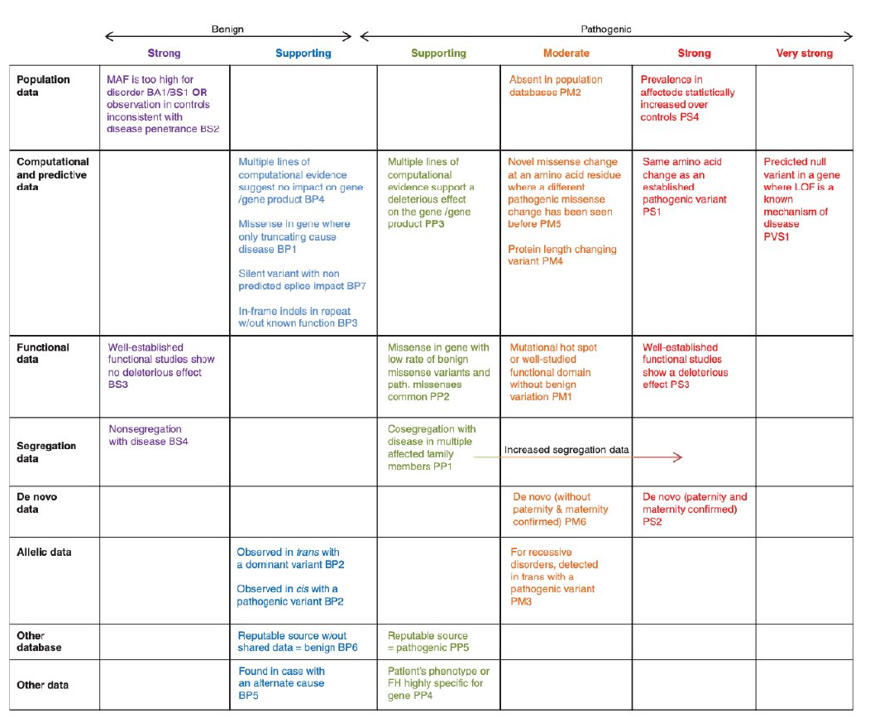
Richards, S., Aziz, N., Bale, S., Bik, D., Das, S., Gastier-Foster, J., Grody, W., Hedge, M., Lyon, E., Spector, E., Voelkerding, K., & Rehm, H. (2015). ACMG guidelines for variant interpretation and Classification. ACMG. https://www.acmg.net/docs/standards_guidelines_for_the_interpretation_of_sequence_variants.pdf

ALERT
|
Contra-indication for use of Ketogenic Diet; fatty acid oxidation deficiencies; pyruvate carboxylase deficiency and other gluconeogenesis defects; glycogen storage diseases (except type 2); porphyria; prolonged QT syndrome; liver, kidney or pancreatic insufficiency; hyperinsulinism; ketolysis and ketogenesis defects |
Introduction of the Ketogenic Diet
An admission of 4 to 5 days is required for the introduction of the ketogenic diet. During the admission parents will be involved with education involving meal preparation, monitoring of urine ketosis and blood glucose as well learning to navigate potential adverse effects.
The most common adverse effects on admission are nausea and vomiting, hypoglycemia and metabolic acidosis. The nausea and vomiting may occur on day 2 post introduction of the KD and this is most likely related to the rapid onset of ketosis. Blood gas (capillary) is monitored daily. Hypoglycemia may also occur and is usually transient and resolves within the first 3 to 4 days. Serum glucose is monitored q6hours. Metabolic acidosis can occur on day 3 -4 and usually resolves, with treatment, bicarbonate supplement, one to two months post introduction of KD.
Serum Ketones: Beta-hydroxybutyrate levels are monitored bid. Ideal Beta-Hydroxybutyrate level is between 2mmol/L to 4mmol/L.
ECG: An ECG is required during admission if not completed prior to admission. Cardiology should be consulted for any abnormalities. Selenium deficit is a potential complication of the ketogenic diet and associated risk for cardiomyopathy.
MEDICATIONS (if necessary):
| Elixir medications, chew tabs and enteric coated tablets should be avoided given their high glucose content. This includes antibiotics, analgesics, antihistamines and antiepileptic medications Consult pharmacist for an assessment of carbohydrate content of all medications prior to initiating KD. This includes antibiotics, analgesics, antihistamines and antiepileptic medications. |
Acute loss of Ketosis:
If there is an abrupt loss of ketosis, there is a risk for increased seizures. This may occur if the child receives an intravenous infusion with Dextrose, if the child receives a medication that contains glucose and/or if the child eats food products that contain large qualities of glucose.
Action: Verify serum ketones by measuring Beta-Hydroxybutyrate. Resumption of Ketogenic Diet protocol as soon as possible.
Hyperketosis:
Hyperketosis can occur during fasting, or with initiation of Ketogenic Diet. Nausea, vomiting, lethargy, tachycardia may occur.
Action: Verify serum ketones by measuring Beta-Hydroxybutyrate, or if available, using ketone-sticks and glucometer supplied by family. Treat with 30 cc orange juice PT/PO. If child unable to tolerate PO/PT insert IV and give 50cc D5W. Repeat after 20 minutes. Keep IV insitu with NS infusion for 24 hours until nausea and vomiting subside. Continue to monitor Beta-Hydroxybutyrate every 6 hours for 48 hours. If hyperketosis persists, Ketogenic Diet ratio should be modified.
| Beta-Hydroxybutyrate levels should be between 2mmol/L and 4mmo/L. For children with Glut-1 Deficiency or pyruvate dehydrogenase deficiency, Beta-Hydroxybutyrate level should be between 2 mmol/L and 3 mmol/L. Children in PICU for status epilepticus, Beta-Hydroxybutyrate can be up to 7mmol/l as long hyperketosis tolerated |
Hypoglycemia
Hypoglycemia, serum glucose less than 2.8 mmol/L, may occur when fasting or at the initiation of the Ketogenic Diet. This may result in nausea, vomiting and lethargy.
Action: On these occasions (fasting, initiation of Ketogenic Diet) serum glucose should be monitored every 6 hours. If serum glucose, less than 2.8 mmol/L give 30cc orange juice PO/PT or 50 ml Dextrose IV. Repeat serum glucose after 20 minutes. If hypoglycemia persists, Ketogenic Diet ratio should be decreased.
Metabolic Acidosis:
Metabolic Acidosis may occur with the introduction of the Ketogenic Diet. This may result in decreased PO intake, vomiting, lethargy.
Action: If the serum bicarbonate level is less than 18 mmol/L then consult nephrology protocol (in Addendum 1) and a bicarbonate supplement is usually prescribed. If despite bicarbonate supplement, metabolic acidosis persists, consult nephrology.
Selenium Deficiency:
Selenium deficiency may lead to cardiomyopathy.
Action: Prior to the introduction of the Ketogenic Diet and for the duration of the ketogenic Diet, an ECG should be completed, and then yearly thereafter. Selenium levels should be monitored, and supplementation given as needed. Selenium levels every done every 6 to 12 months.
| There are three formulas available for the Ketogenic Diet. All require RAMQ or Private insurance approval: Ketocal DIN 99113792 (all flavours), Chocolate DIN: 99113796, Vanilla 99113797, non-flavoured DIN 99114005 Ketovie:DIN 99114030 Ketovie Peptide: DIN 99113949 Ketovie and Ketovie Peptide plant based proteins and are Kosher |
Fractures: Children who are non-ambulatory are at an increased risk for fractures
Action: phosphate, calcium and vitamin D levels. Consult Bone Health Clinic at the Shriner’s Hospital.
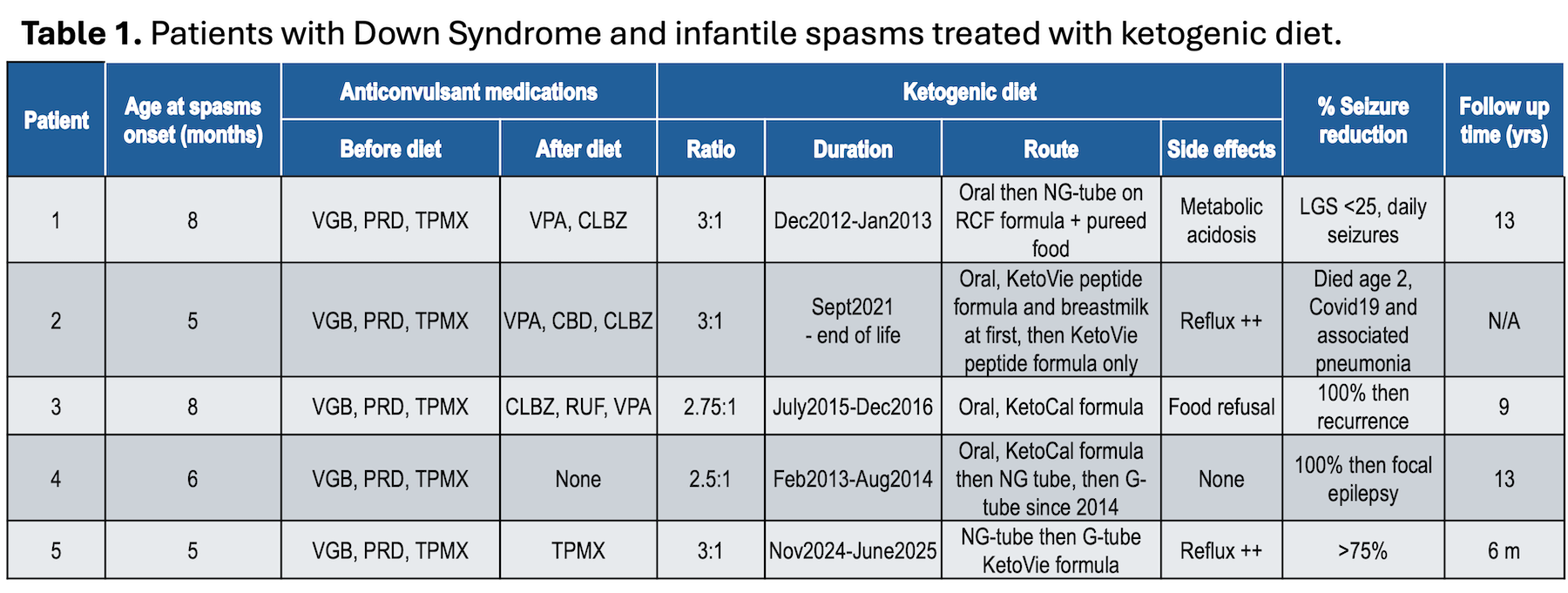


Out of 11 patients with Downs Syndrome and infantile spasms, 5 infants were treated with a ketogenic diet due to lack of clinical electroclinical response to anticonvulsants.
Patients were followed for an average of 6.5yrs (1- 15 yr). Of 6 patients who responded to medications, only one later developed refractory focal epilepsy.
Of those treated with a ketogenic diet, all remained but 1 remained on medications. 2/5 had full electroclinical response. Partial seizure reduction and electrographic improvement was observed in 1 infant. 1 patient died due to unrelated respiratory illness. None remained seizure free at >5 year follow up.
One patient had an exome sequence analysis searching for independent causes of refractory epilepsy but did not identify a pathogenic variant.
Most common side effects associated to the diet where: gastroesophageal reflux and diet tolerance at initiation required diet to be delivered via G-tube in 1 patient and by NG tube in 3 patients to avoid risk of aspiration.
In this small cohort of patients, almost half were medication refractory and of those ketogenic diet therapy at least partially effective in the majority.
No clear distinction on age at seizure onset, medications used, or MRI findings appear to correlate with lack of medication response.
Ketogenic diet is a viable potentially effective therapeutic option for infants with Down syndrome and medication refractory infantile spasms. These infants present challenges inherent to Down syndrome such as hypotonia, higher risk for aspiration which need to be considered before diet introduction.
To address this, a retrospective chart review of 122 adolescents (42 MID and 80 typical cognitive development) with epilepsy between the ages of 14 and 18, was done.
|
|
MID: ED visit over 1 year (n=10) |
MID: no ED visit over 1 year (n=32) |
Typical: ED visit over 1 year (n=47) |
Typical: No ED visit over 1 year (n=33) |
|
|
Sex |
Males |
20.0% |
81.3% |
42.6% |
45.5% |
|
|
Females |
80.0% |
18.8% |
57.4% |
54.55 |
|
Age of seizure onset (years) |
4.53 years |
6.21 years |
10.24 years |
10.52 years |
|
|
Seizure type |
Focal |
50.0% |
50.0% |
42.6% |
21.2% |
|
|
Generalized |
40.0% |
25.0% |
44.7% |
45.5% |
|
|
Both |
10.0% |
21.9% |
10.6% |
27.3% |
|
|
Unknown |
0.0% |
3.1% |
2.1% |
6.1% |
|
# of AMS |
0 |
0% |
16.1% |
2.1%% |
6.1% |
|
|
1 |
60.0% |
38.7% |
61.7% |
54.5% |
|
|
2 |
20.0% |
29.0% |
27.7% |
33.3% |
|
|
3 |
20.0% |
16.1% |
8.5% |
6.1% |
|
Seizure Frequency |
Daily |
0.0% |
3.1% |
14.9% |
6.1% |
|
|
Weekly |
0.0% |
9.4% |
2.1% |
3.0% |
|
|
Monthly |
0.0% |
0.0% |
8.5% |
3.0% |
|
|
Less often |
100% |
87.5% |
68.1% |
81.8% |
|
|
Unknown |
0.0% |
0.0% |
6.4% |
6.0% |
|
MID: ED visit over 1 year (n=10) |
MID: no ED over 1 year visit (n=32) |
Typical: ED visit over 1 year (n=47) |
Typical: No ED visit over 1 year (n=33) |
||
|
Age at ED Visit |
16.62 |
N/A |
15.95 |
N/A |
|
|
Length ED visit (Hours) |
21.41 |
N/A |
4.73 |
N/A |
|
|
Reason for visit |
Seizure |
90.0% |
N/A |
46.8% |
N/A |
|
Injury |
10.0% |
N/A |
4.3% |
N/A |
|
|
Medication |
0.0% |
N/A |
6.4% |
N/A |
|
|
Fear |
0.0% |
N/A |
8.5% |
N/A |
|
|
Other (not sz related) |
0.0% |
N/A |
29.8% |
N/A |
|
|
ED Visits (last 3 years) |
2.60 |
1.09 |
4.17 |
1.12 |
|
|
ED seizure visits (last 3 years) |
1.40 |
0.22 |
2.02 |
0.53 |
|

Common etiologies:
Genetic variants
Inborn errors of metabolism
Remote acquired brain injury
Unknown
Clinical presentation:
Gradual worsening of baseline dystonia over days/weeks, often with an identified trigger
The challenge:


2. Clinical data collection
3. Understand personal experiences with status dystonicus
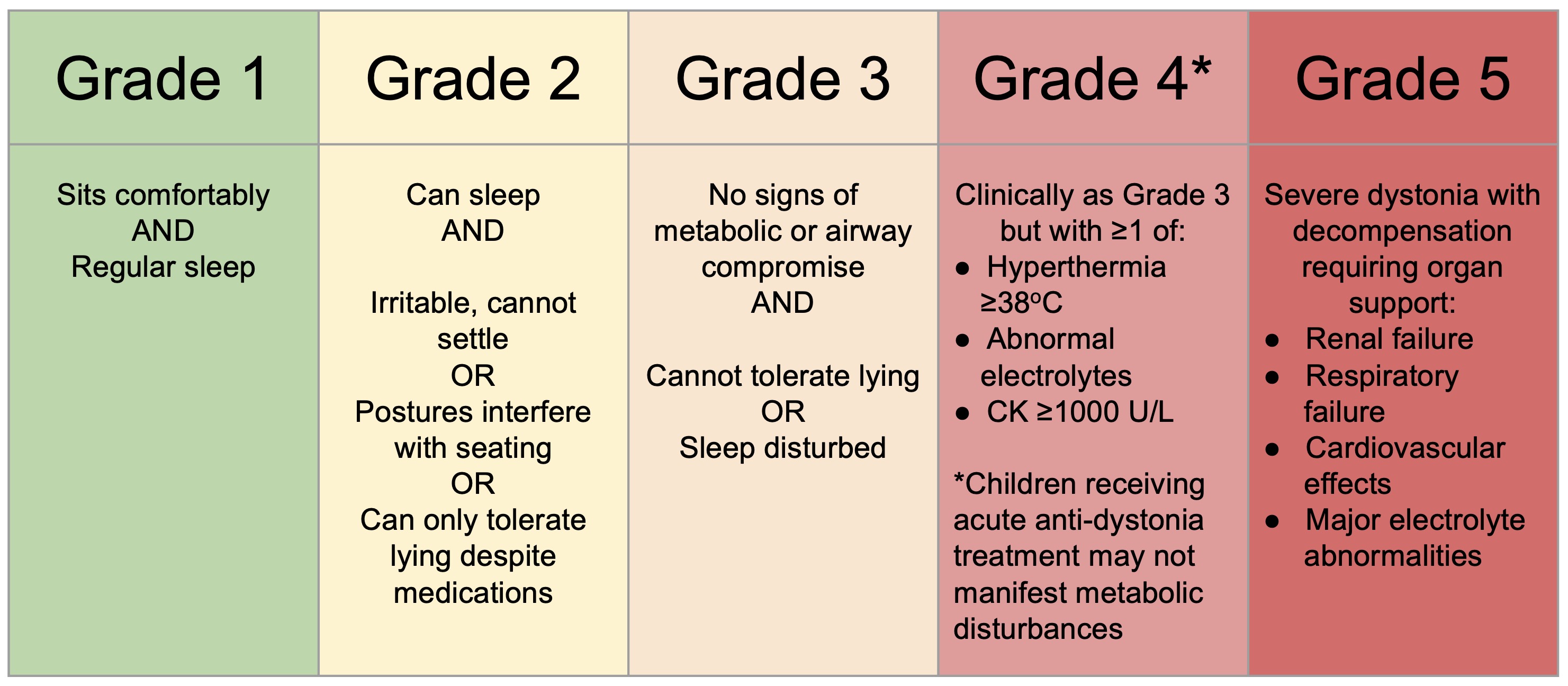
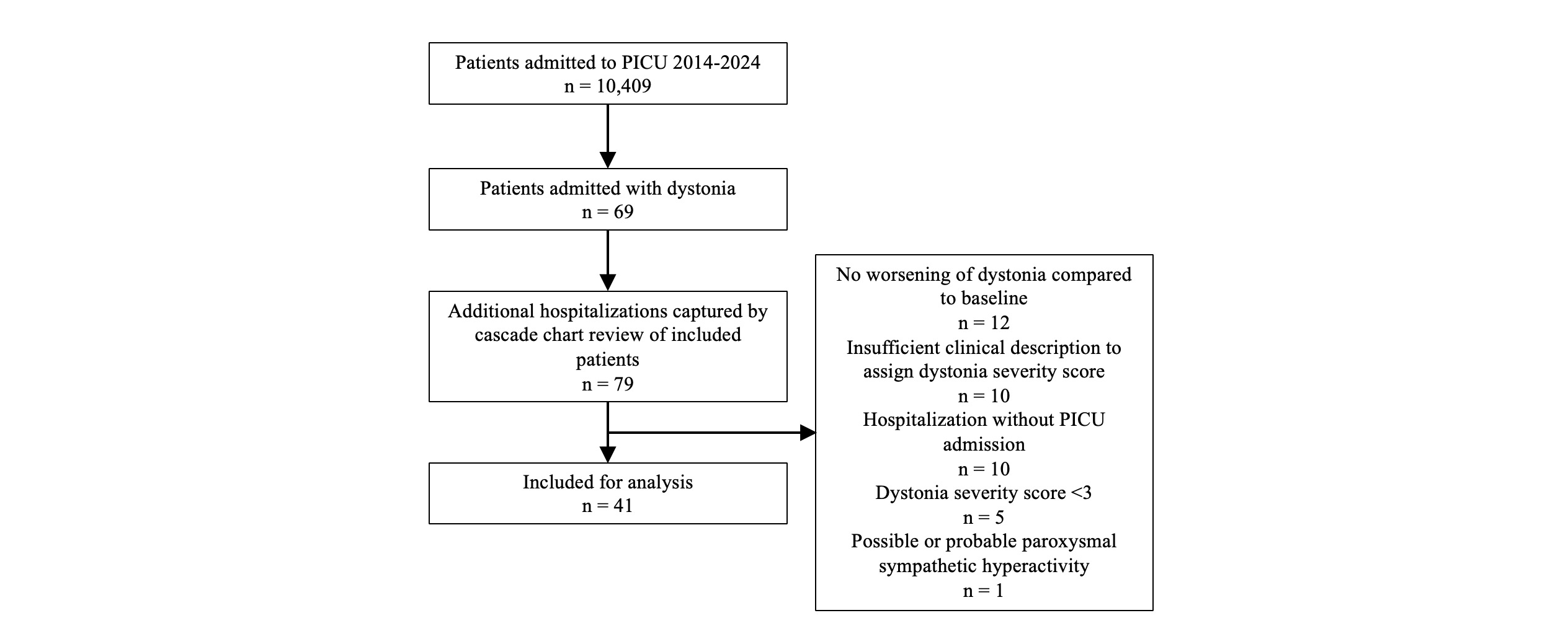
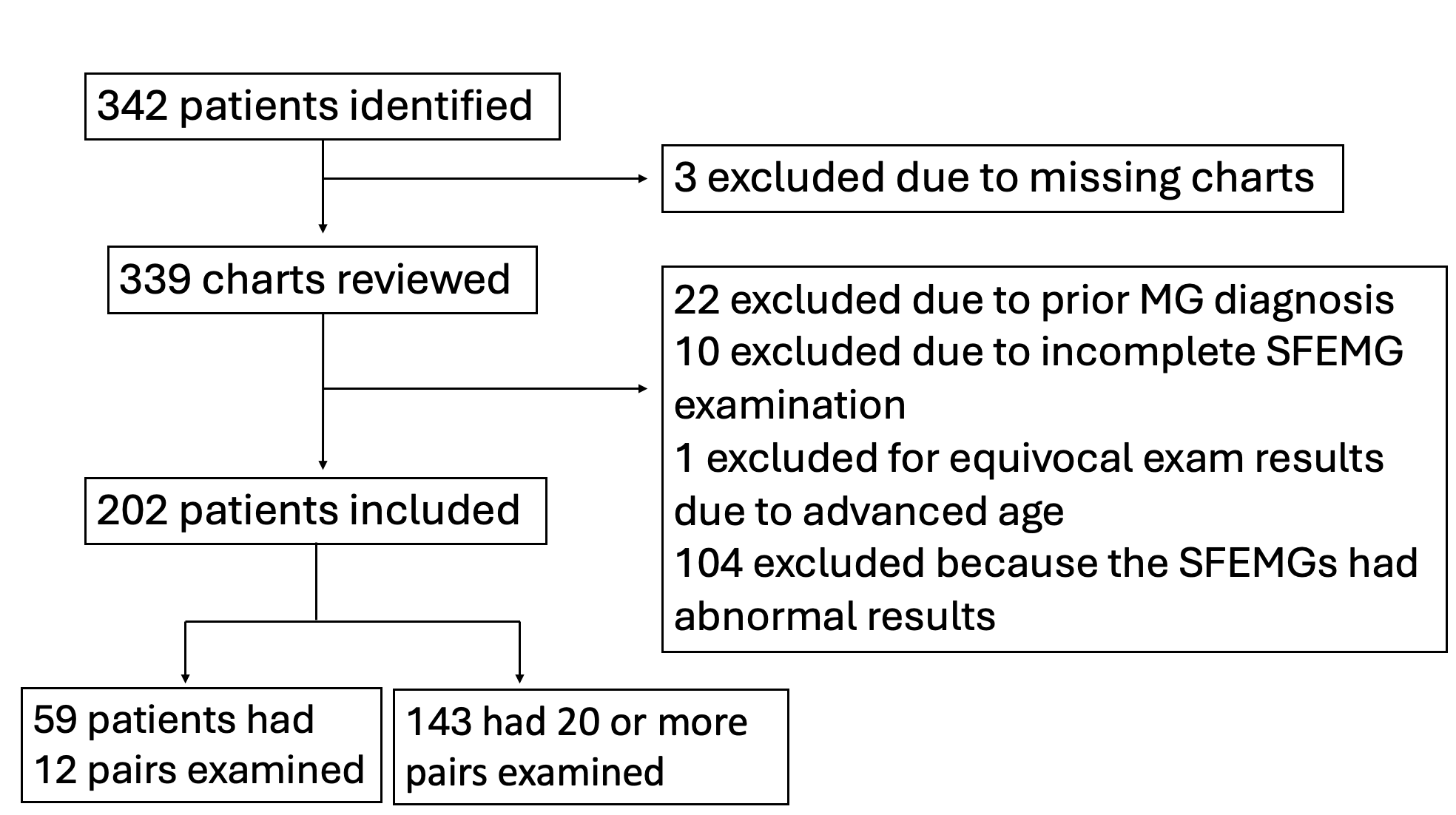
Figure 2. Flow diagram of included and excluded participants

Methods
MOXIe Part 2
Figure 1. MOXIe Part 2 Study Design5

MOXIe Part 2 (continued)
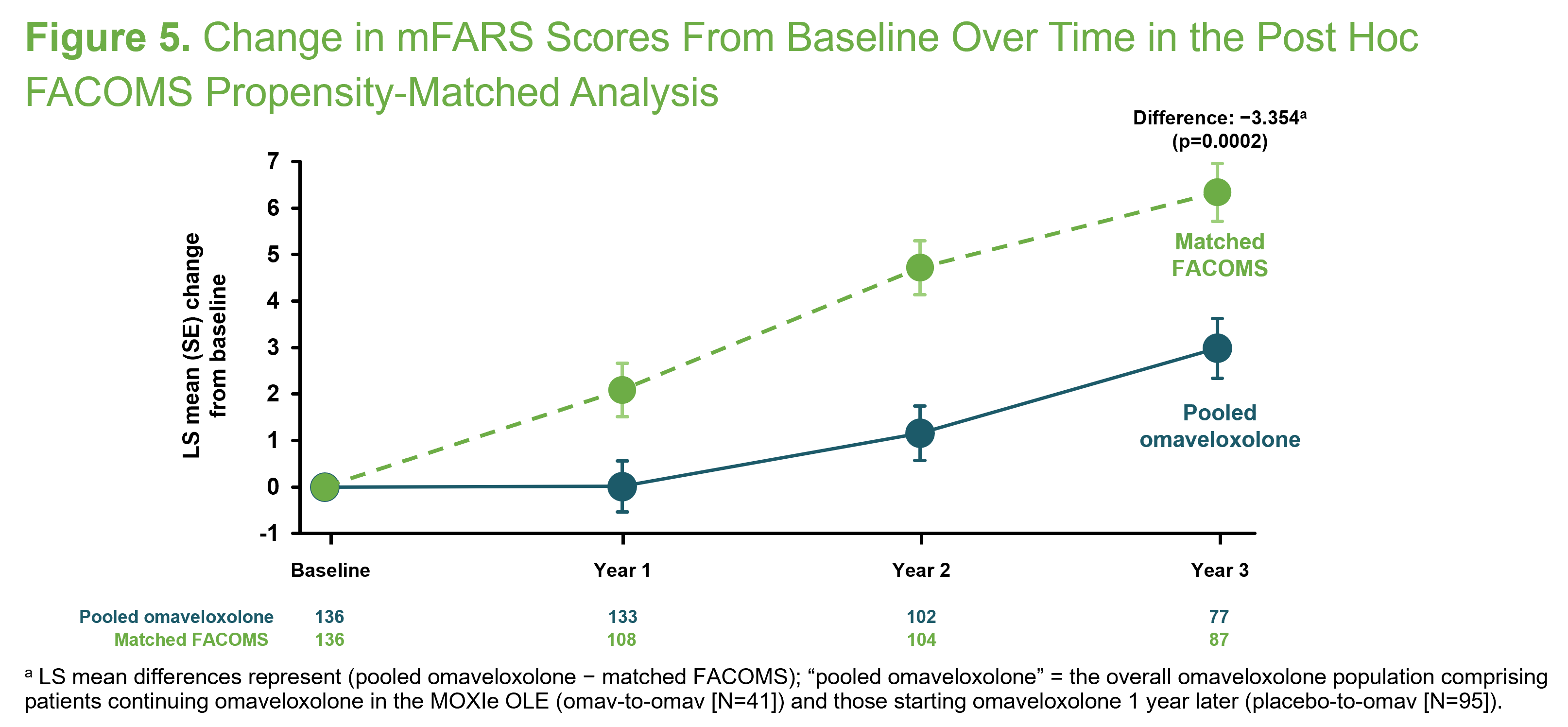
Propensity-Matched Analysis
Figure 2. Propensity Analysis Design7
Results
Baseline Characteristics

Efficacy
Figure 3. Change From Baseline in mFARS Scores in the FAS and ARP at Week 48
Safety
Safety (continued)
Table 1. Summary of Treatment-Emergent AEs in MOXIe Part 2 (All Patients)13
Figure 4. Mean (SE) Change From Baseline in Liver Enzyme (ALT and AST), Total Bilirubin, BNP, and Serum Lipid Levels Over Timea
Propensity-Matched Analysis
Figure 5. Change in mFARS Scores From Baseline Over Time in the Post Hoc FACOMS Propensity-Matched Analysis
Copyright ©2025 Biogen Inc. All rights reserved

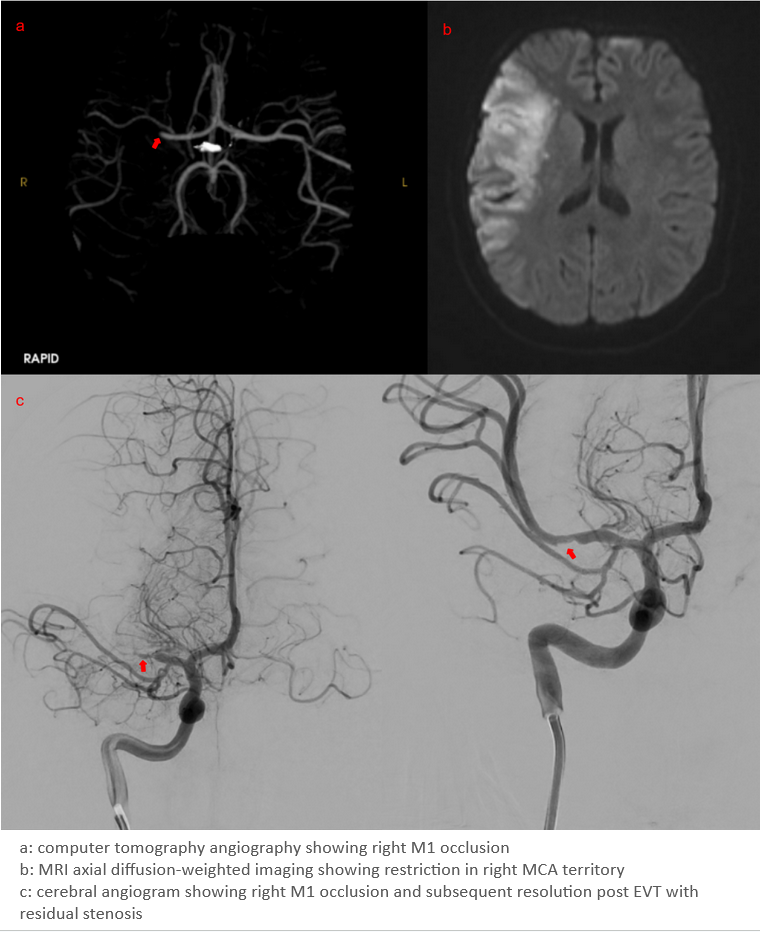
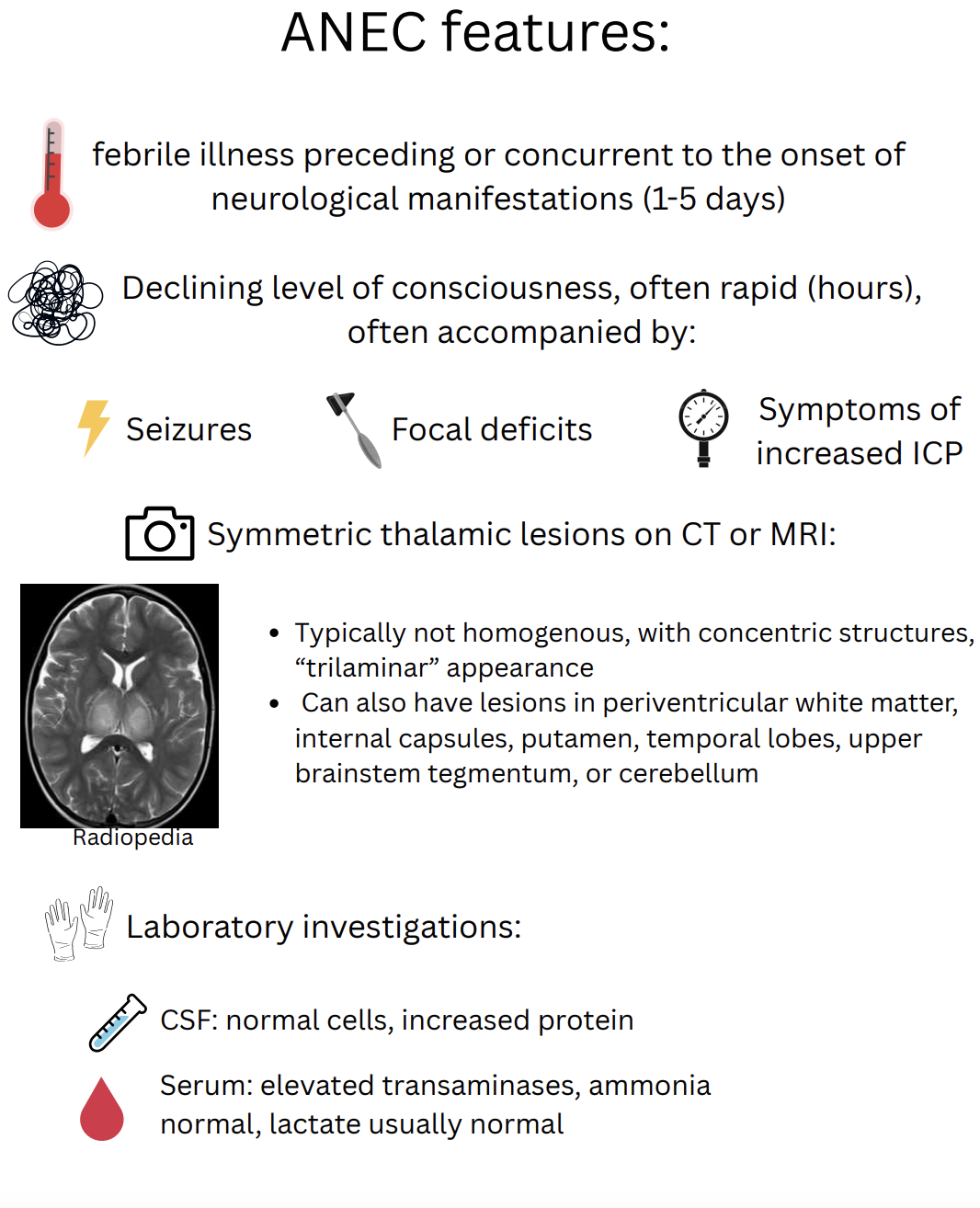
Figure 1: Notable Imaging Findings

|
Treatment |
Notes |
|
High-dose methylprednisolone (30mg/kg) x5 days |
Established evidence. Administration within 24 hours of presentation associated with improved morbidity/mortality. |
|
IV Immunoglobulins |
Commonly used adjunctive therapy |
|
Plasmapheresis |
Often used in cases with ongoing deterioration, failure to plateau within 2-3 days |
|
Tocilizumab |
IL-6 monoclonal antibody; thought to target underlying pathophysiology. Promising in small case series |

Duchenne muscular dystrophy (DMD) is a progressive neuromuscular disorder inherited in an X-linked pattern. Pathogenic variants result in the absence of dystrophin, a protein that is essential for muscle fiber integrity.
Due to absent dystrophin, patients present with weakness and gross motor delay. DMD results in the loss of independent ambulation as well as cardiorespiratory complications and premature death.
DMD patients typically present with painless muscle weakness. As such, their symptoms can potentially be misattributed to a lack of interest or proficiency in sports. This can lead to a delay to diagnosis. Language delays and cognitive difficulties are also common in DMD which also present challenges with its recognition.
Early diagnosis and intervention is important to improve motor outcomes. This is increasingly necessary given the emergence of disease modifying therapies [1].
We reviewed all medical records for children with a genetic diagnosis of DMD who were followed at CHEO over 15 years (Jan 1, 2009 to Dec 31, 2023). Data was extracted from medical records into a REDCap data collection form. REB approval was obtained prior to the start of data collection (CHEOREB# 24/43X).
Inclusion criteria included: 1) genetic diagnosis of DMD; 2) participants must have had an onset of symptoms < 6 years of age and; 3) received ongoing clinical care at CHEO. Subjects were excluded if there was any family history of DMD (e.g. sibling, uncle) as this may have influenced the recognition of symptoms and time of diagnosis.
The results from this single institution will be combined with data from two other centres (BC Children’s Hospital, Bloorview Holland Rehabilitation Hospital) when their data is available.
We identified 72 DMD patients of which, N=49 met inclusion / exclusion criteria. Subjects were excluded for: incomplete data (N=10; e.g. diagnosis at another centre); symptom onset >6 yo (N=4); family history of DMD (N=9).
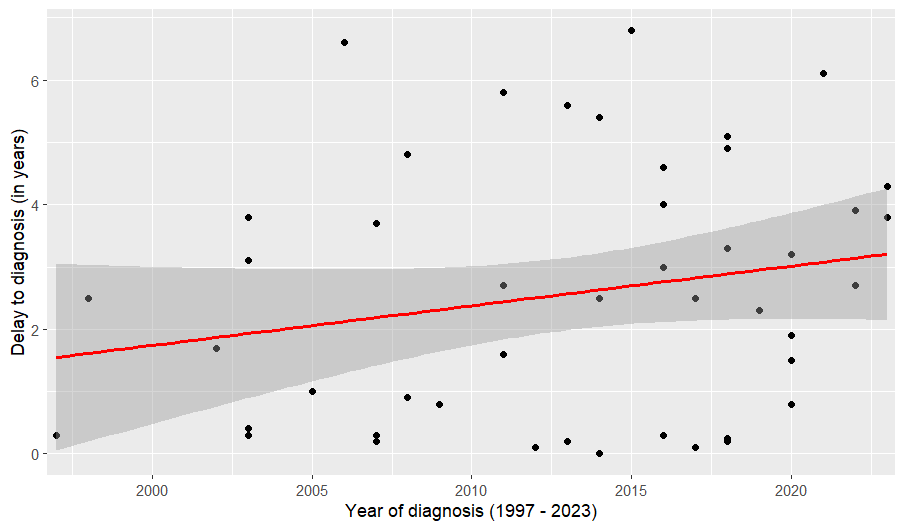
First symptoms were reported by a parent, caregiver or teacher at a mean age of 2.61 yo (range: 0 to 5.9 yo). The mean age of DMD diagnosis was 5.17 yo (range: 0.5 to 9.6 yo). This represented a mean delay of 2.56 years (range: 0.5 to 6.8 years; Figure 1).

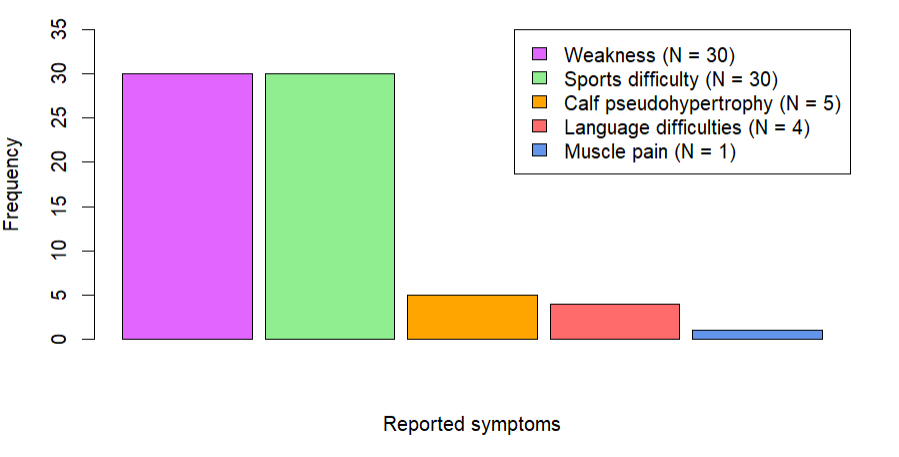
Initial symptoms included: weakness (61.2%), sports difficulty (61.2%), calf pseudohypertrophy (10.2%), language difficulties (8.2%) or muscle pain (2.0%; Figure 3). Learning disability was reported in 36 (73.5%) subjects with 7 (14.3%) having autistic spectrum disorder although in most children this was not the reason for DMD diagnostic testing.
The mean delay from symptom-onset to diagnosis was 2.56 years after a parent, caregiver or teacher first noted symptoms attributable to potential DMD (i.e. weakness, sports difficulty, etc).
Our study reveals a delay to diagnosis that is similar to what has been reported in the United Kingdom [2].
Our findings noted muscle pain to be an infrequent presenting symptom (only 1/49; 2% patients) which we believe may have contributed to the delay in many cases. In 8/49 (16.3%) of cases, the diagnosis of DMD was suspected after serum CK was noted as unexpected finding on a surveillance blood test.
1. Koeks Z et al. Clinical Outcomes in Duchenne Muscular Dystrophy: a Study of 5345 Patients from the TREAT-NMD DMD Global Database. J Neuromuscul Dis 2017;4:293–306.
2. Ciafaloni E et al. Delayed diagnosis in Duchenne muscular dystrophy: data from the muscular dystrophy surveillance, tracking and research network (MD STARnet). J Pediatr. 2009: 155(3): 380-385.

- Spinal muscular atrophy (SMA) is a severe progressive neuromuscular disease caused by biallelic mutations of the Survival Motor Neuron 1 (SMN1) gene on 5q13.2, leading to loss of motor function and reduced life expectancy.
- Survival motor neuron (SMN) protein is crucial during early stages of human development. A delay of SMN induction of weeks or months can substantially reduce achievement of motor milestones.
- Currently there are 3 approved SMA therapies (nusinersen, onasemnogene abeparvovec, and risidiplam) with potential in halting disease progression; the best outcomes were seen among infants who were treated presymptomatically.
To describe clinical outcomes of infants diagnosed with SMA through the Alberta Newborn Screening (NBS) program over the past 3 years. This study was approved by the University of Calgary.
- The Alberta SMA newborn screening program was launched on Feb 27, 2022. DNA extracted from dry blood spot (DBS) cards were analysed using a multiplex qPCR assay to detect deletions in exon 7 of SMN1 for SMA, in combination with screening for severe combined immunodeficiency (SCID).
- Screen-positive infants underwent multiplex ligation-dependent probe amplification (MLPA) using a separate blood sample to confirm the diagnosis and determine SMN2 copy number.
Baseline Characteristics:
- From 28 February 2022 to 31 December 2024, there were 147,085 live births in Alberta.
- 12 infants were screened positive for SMA, and subsequently confirmed to have SMA.
- Median age at positive screen was 6 days (range=3-9), and at diagnosis, 15 days (range=11-27).
- Two had 2 SMN2 copies, six had 3 SMN2 copies, 3 had 4 SMN2 copies, and 1 had 5 SMN2 copies.
Timing of SMA Treatment:
- Median Age at 1st SMA treatment was 30 (range 18-142) days.
- For 2 neonates with 2 SMN2 copies, median age was 20 (range 18-22) days.
Types of SMA Disease Modifying Treatment:
. 7 infants received onasemnogene abeparvovec.
. 2 received nusinersen (Day 22) or risdiplam (Day 72) due to maternal transferred antibodies to AAV9; they received onasemnogene abeparvovec at Day 48 and 111, respectively after repeat AAV9 antibodies came back negative.
. 2 infants with 4 SMN2 copies received risdiplam after 3 months of age; 1 infant with 5 SMN2 copies was not eligible for treatment.
. 1 infant was symptomatic at 1st treatment initiation at 72 days of life; the rest were all presymptomatic when treated.
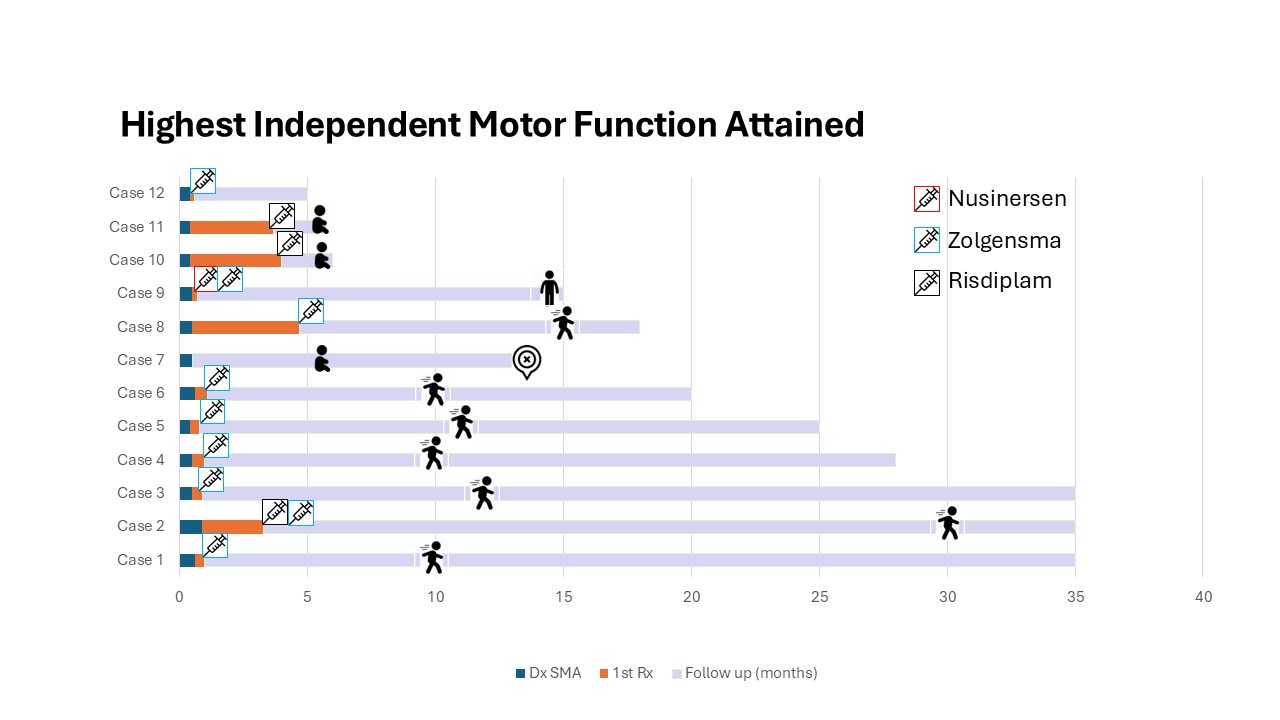
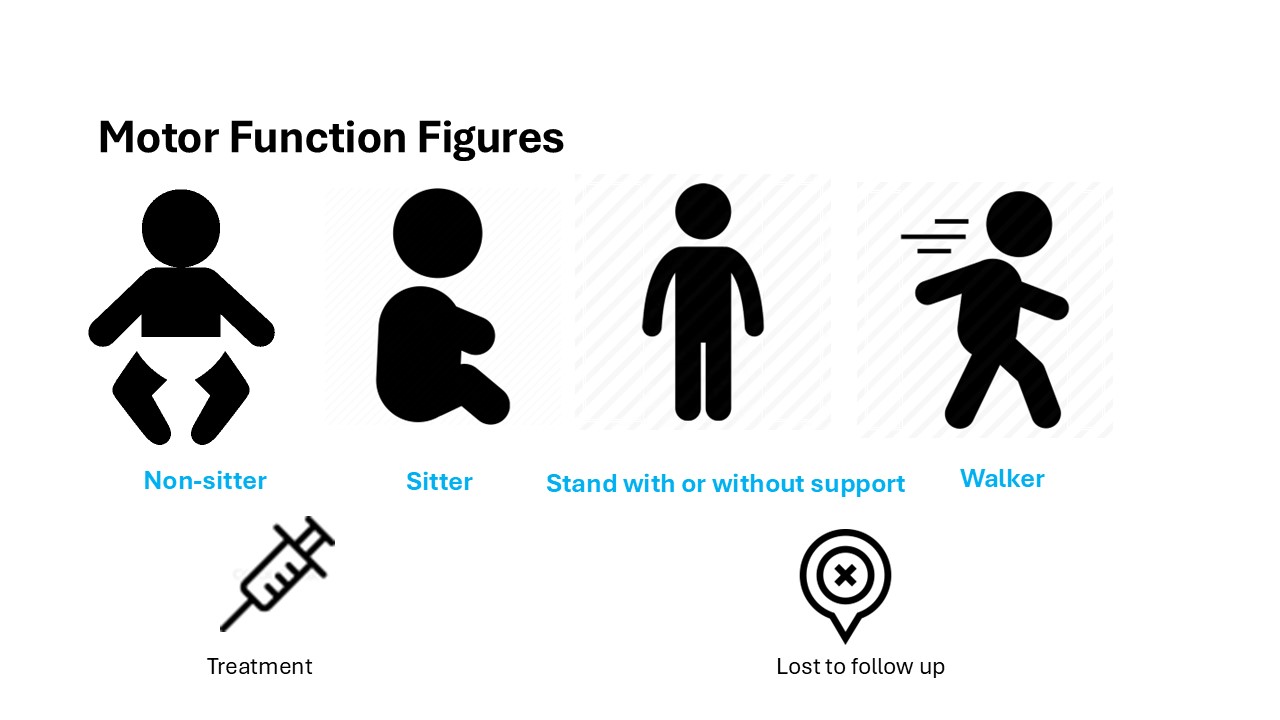
Post-treatment evaluations showed ongoing motor milestone achievements in all 12 children.
- The birth prevalence of SMA in Alberta during 2022-2024 was 8.2 (95%CI: 3.5-12.8) cases per 100,000 live births, compared to our earlier report of 10.6 per 100,000 live births during the first year of the program (Niri et al 2023). Our results are within the range of frequencies reported in other recent studies (Dangouloff et al 2021).
- Treatment initiation after newborn screening was much earlier when compared to children diagnosed with SMA prior to availability of newborn screening (data not shown).
- All 12 children are doing well so far; longterm follow up is required to monitor their growth and development, as well as symptoms and signs of SMA.
- Meanwhile, to shorten the age at treatment initiation, especially for infants with SMA and two to three SMN2 copies, we will advocate for use of risdiplam or nusinsersen as a "bridging" treatment before onasemnogene abeparvovec, as soon as the diagnosis is confirmed.
- We will also advocate for uniform coverage and early treatment of infants with SMA and four SMN2 copies (McMillan et al 2025).
Introduction
Cerebral palsy (CP) is an umbrella term for a group of neurological disorders caused by disturbances in the developing brain in early life, leading to impairments of movement and posture. This results in infants or children who may have differences in function and a visible physical disability.
Body image research in young people with physical disabilities like CP has received very little attention. Body image is a central theme in adolescence, and one may hypothesize that being a youth with CP could weigh particularly heavily on a child’s self-perception.
Methods
We designed a pilot study to learn the perspectives of body image directly from children and adolescents with CP. We were dedicated to include all children and adolescents from 7-18yo with CP, of any communication ability and GMFCS level. As a reminder, the GMFCS is a scale that categorizes children with CP depending on their self-initiated motor ability.
Part I: Pre-structured interview with a child/adolescent with CP to gather their thoughts. An inductive thematic analysis extracted core themes.
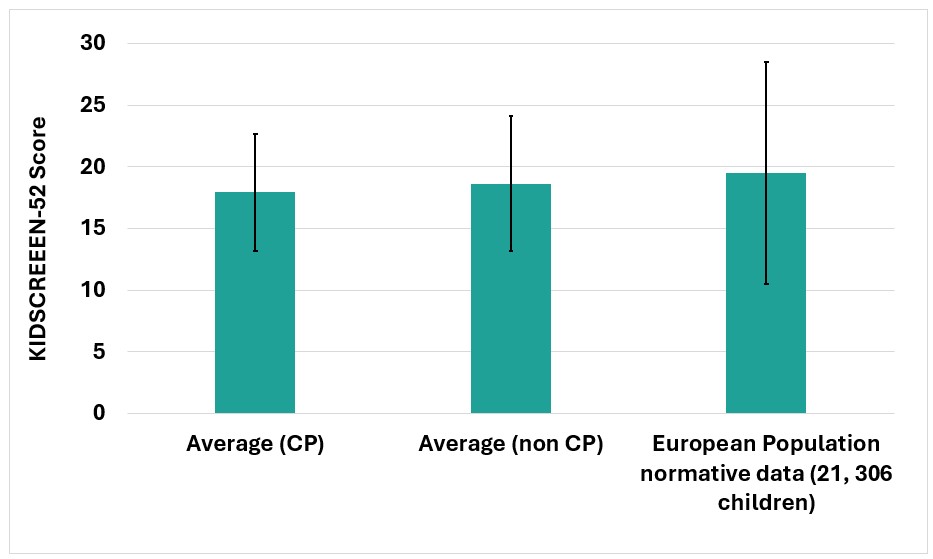
Part II: Administration of a validated quality-of-life (QOL) questionnaire entitled the KIDSCREEN-52, which interrogates about body image, to all participating children along with siblings/twins in the same family group as controls.
Results
Twelve youths with CP (7 male, 5 female) filled out questionnaires and sat for an interview. Three other youths with CP filled out questionnaires but were not available for interview. Thirteen siblings (most of whom were twins/triplets) acted as the control group and completed questionnaires.
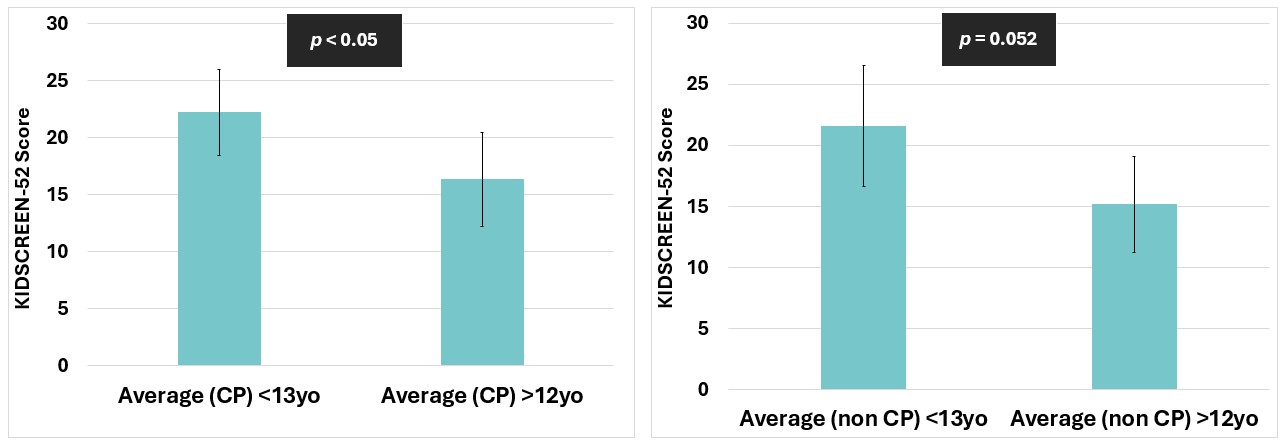
A higher score on the questionnaire represents a more positive body image. The average score among our participants with CP was 17.93 / 25 (SD 4.73), and for those without CP; 18.62 / 25 (SD 5.45). There were higher scores for males compared to females, and higher scores for those <13yo compared to 13-18yo.
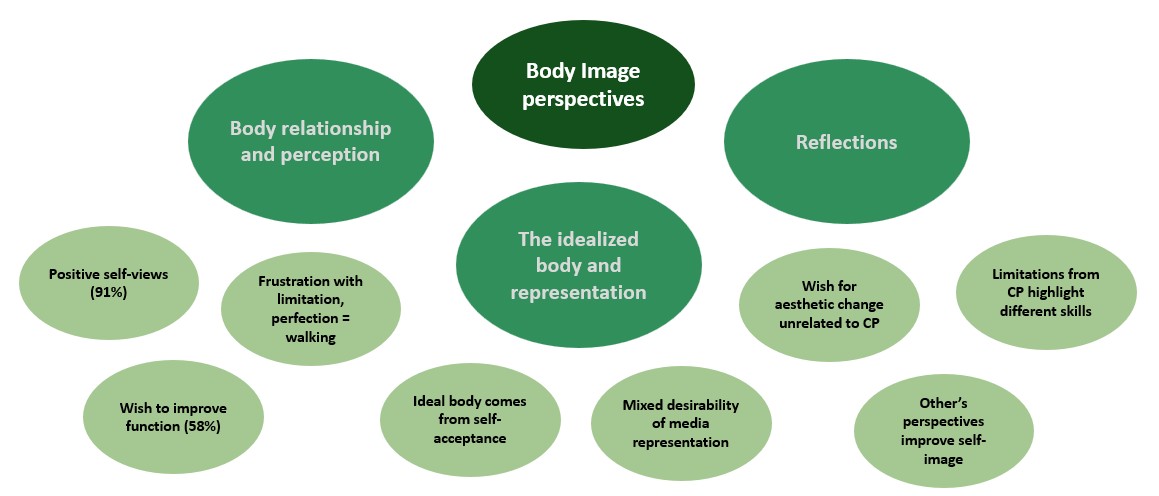
Interviews with participants uncovered some core themes, which included:
- Frustration with functional limitation
- The ability to walk is linked to a positive body association
- The ideal body image comes from self-acceptance
- Pride in the CP identity
- Mixed desirability of media representation
Discussion
Within the bounds of this pilot study, there is a greater difference in the QOL measure of body image between age groups than there is between those with and without CP.
There is an important recurring theme of functional capacity (especially walking) linked to body image, however most participants relayed a positive self-image even in the face of challenges.
We have learned that children with CP have similar concerns about their body image as those without CP, and we can relieve the concerns of caregivers who may feel that a child with CP is especially vulnerable to negative self-image.
Statistical Analysis
Figure 1. Mean HC by age groups compared to WHO mean for males and females
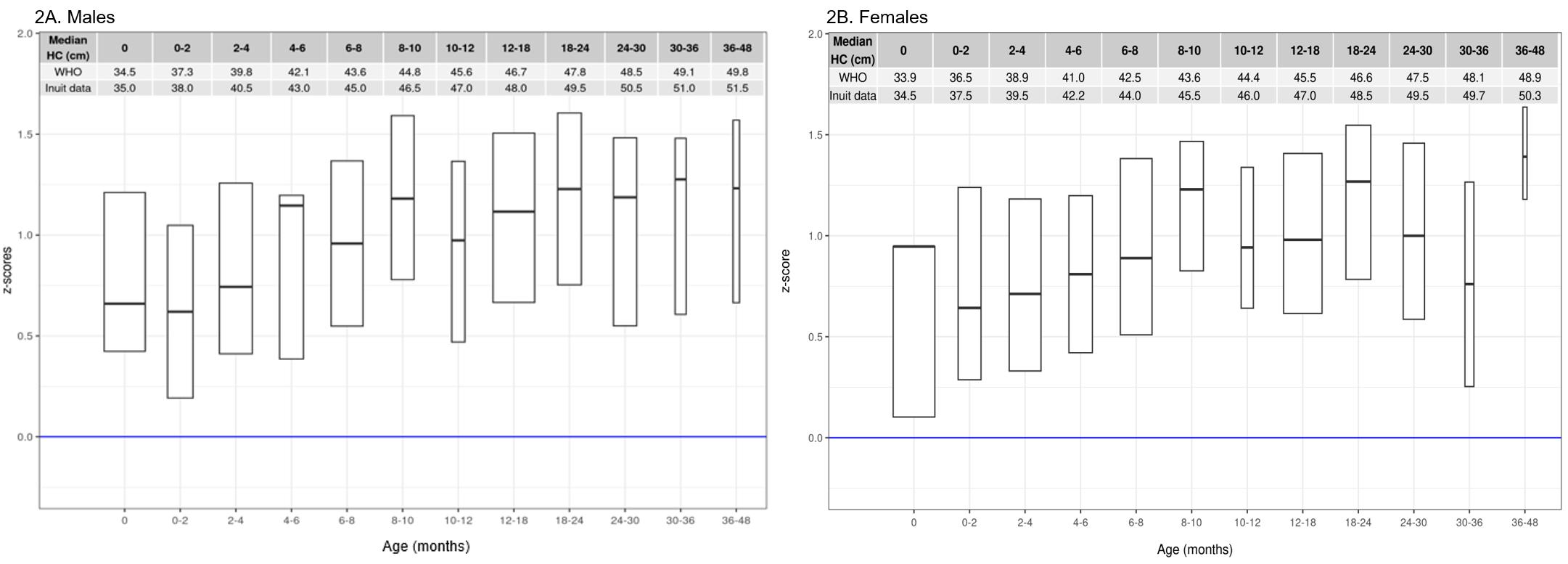
Figure 2. Percentile curves for head circumference
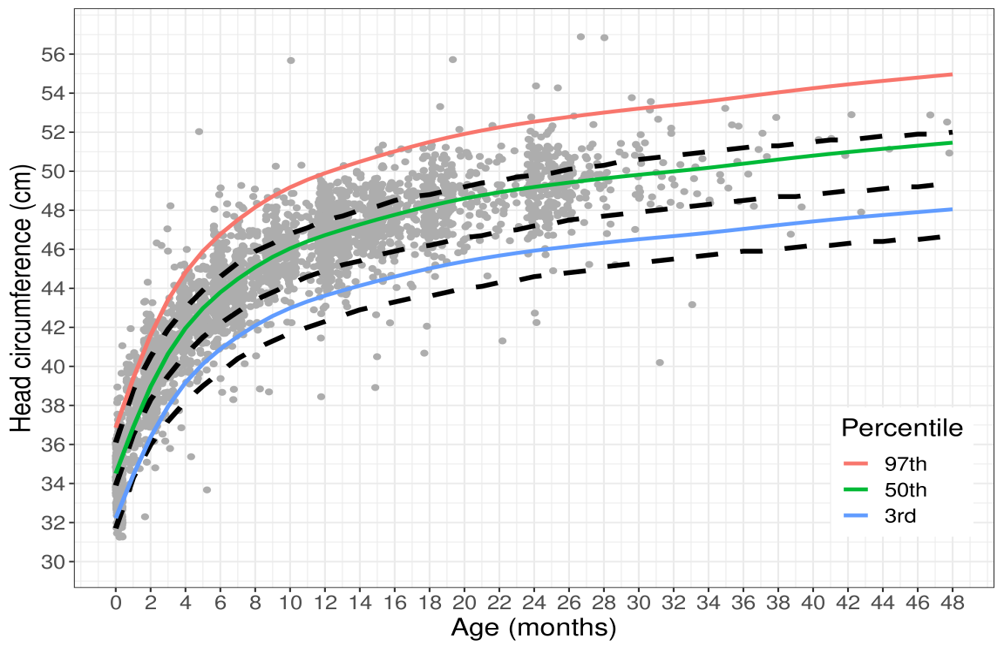
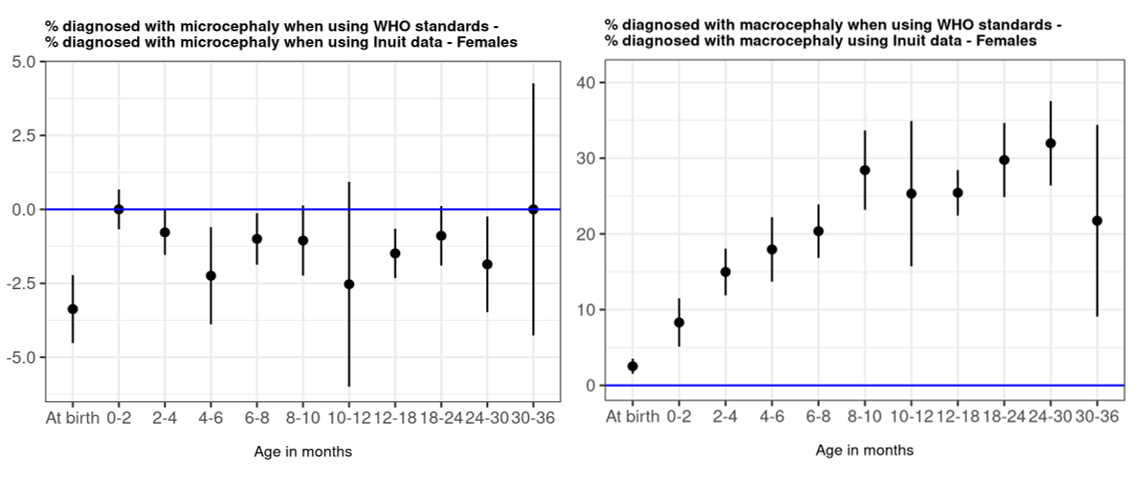
Figure 3. Difference in proportion of children below the 3%ile and above 97%ile based on Inuit population measurements vs. WHO standards

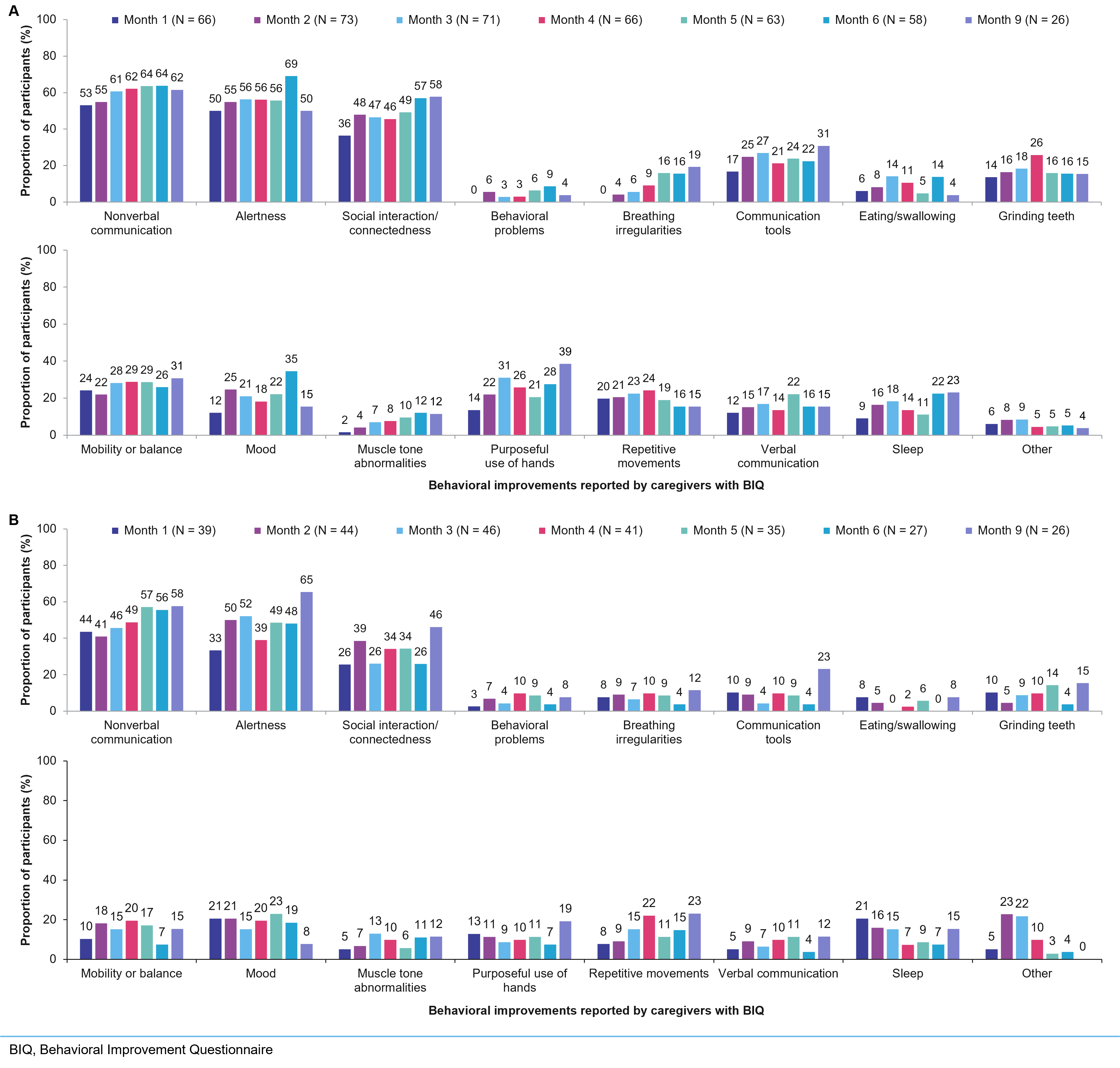
Behavioral Improvements
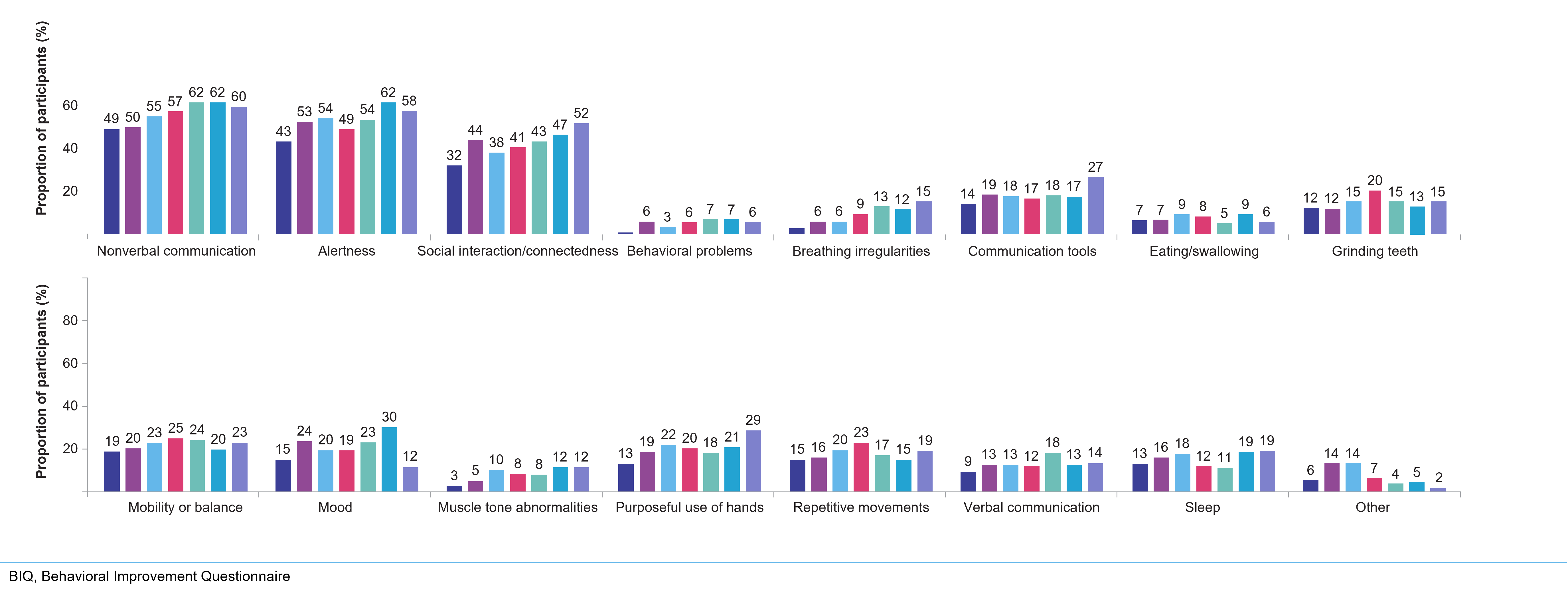
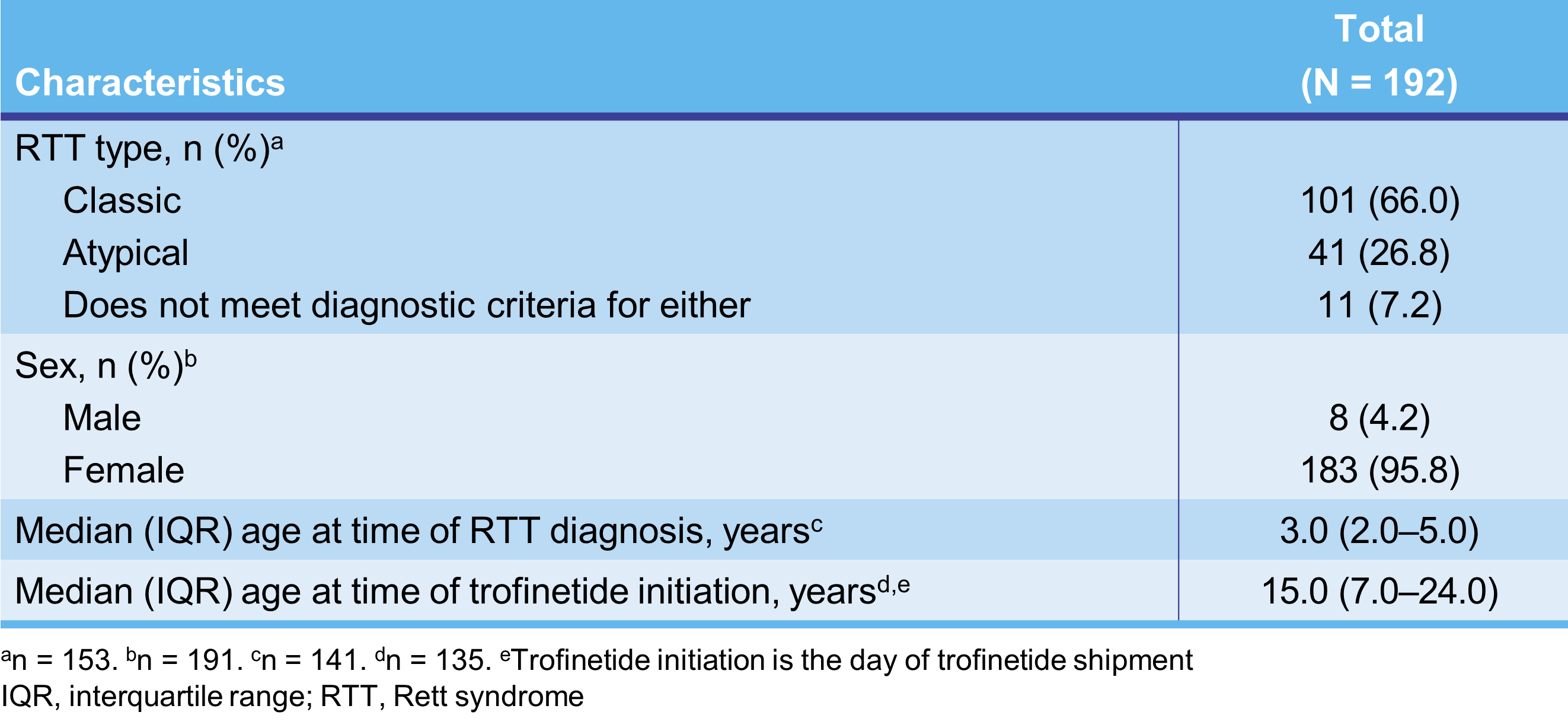
To characterize the benefits and tolerability of trofinetide in pediatric and adult patients with RTT using real-world 12-month follow-up data from the ongoing LOTUS study
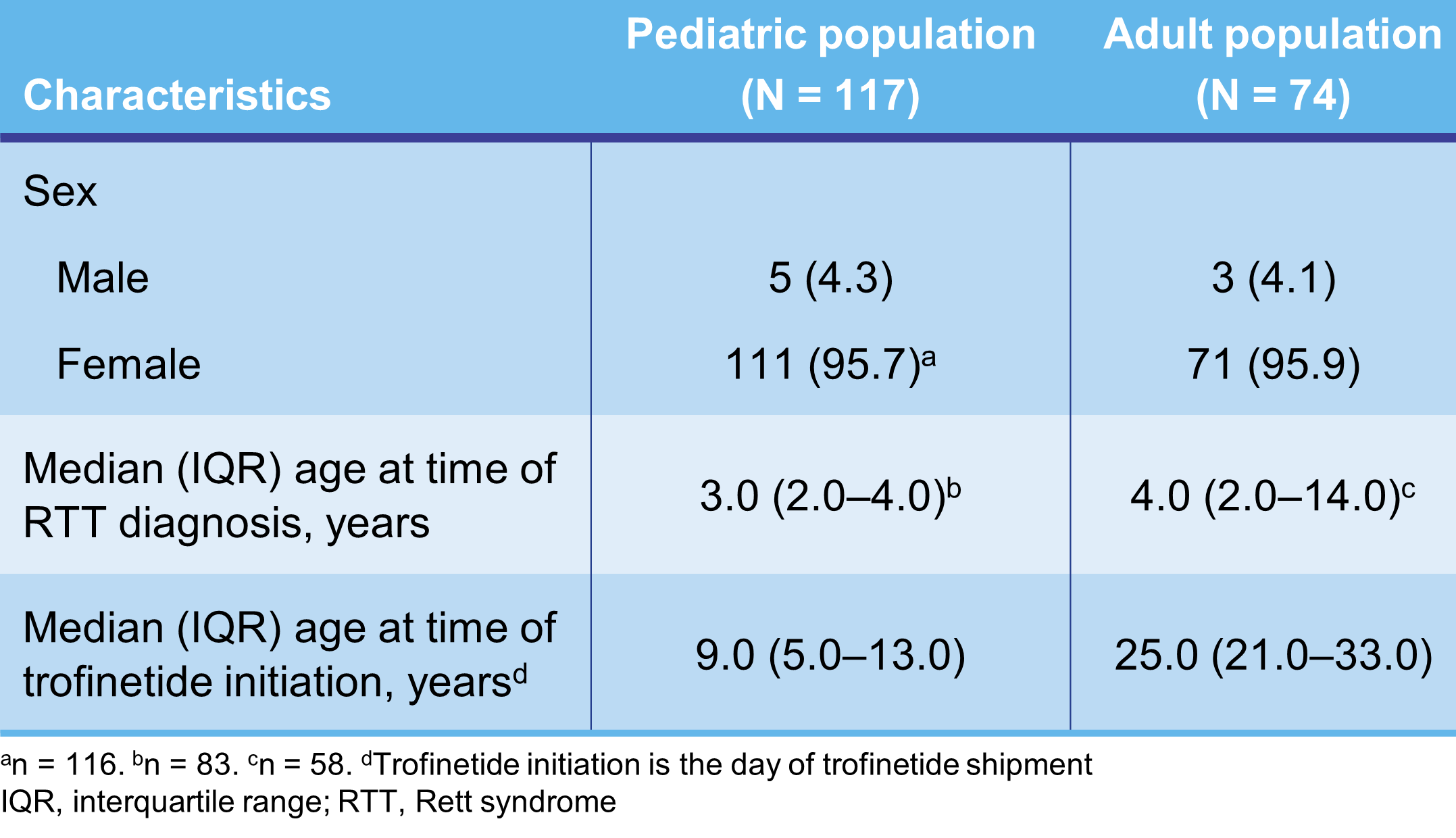
Demographics and Baseline Characteristics
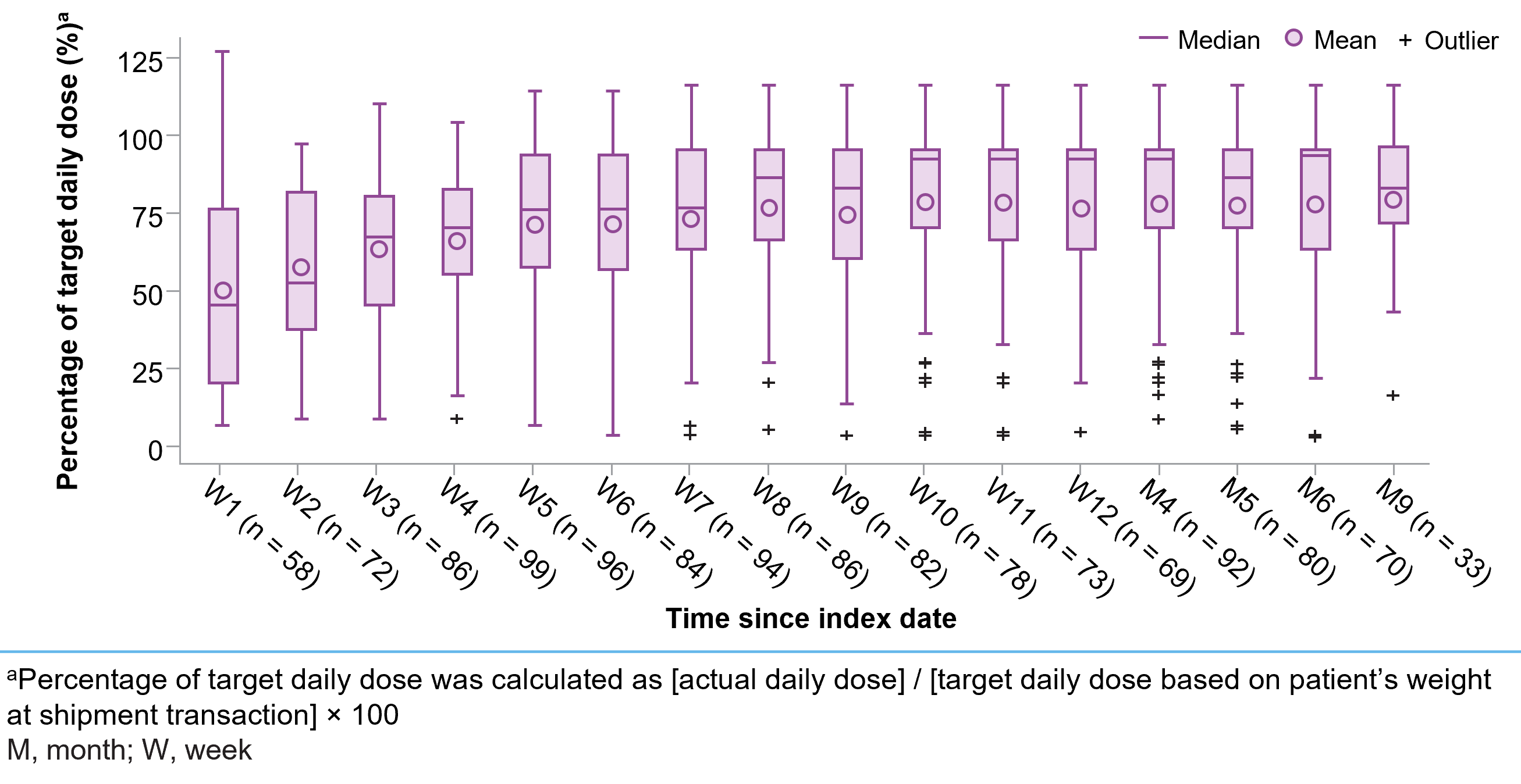
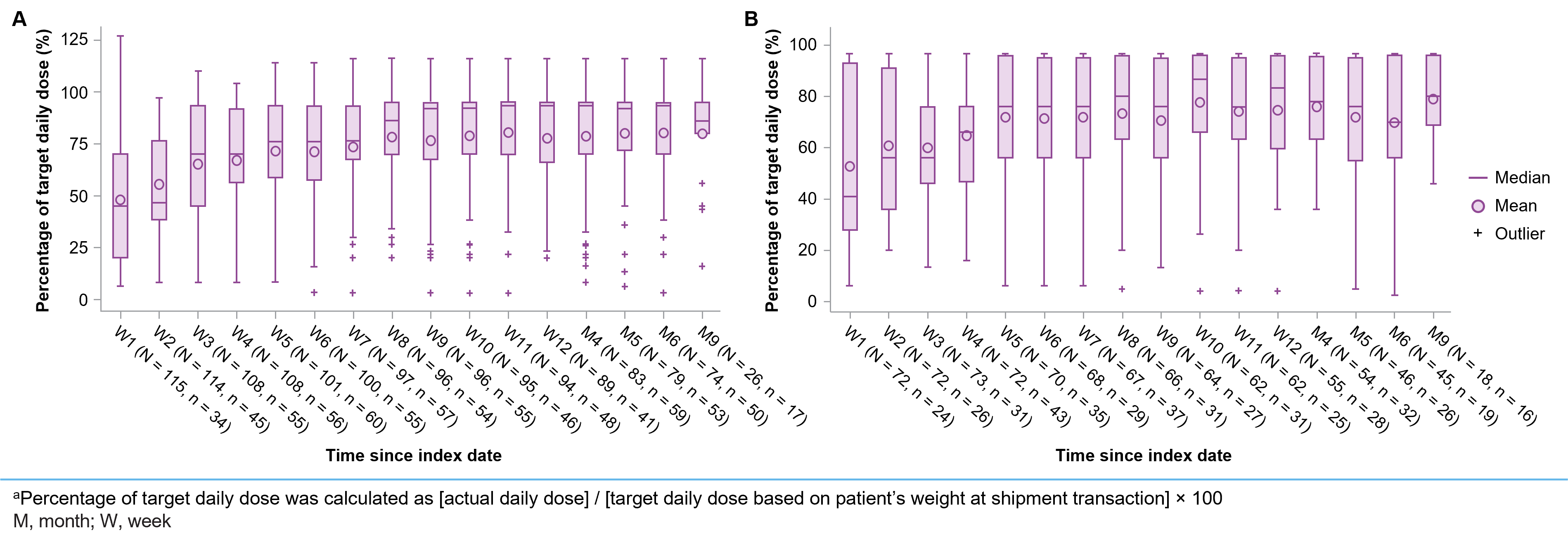
Trofinetide Dosing
Behavioral Improvements
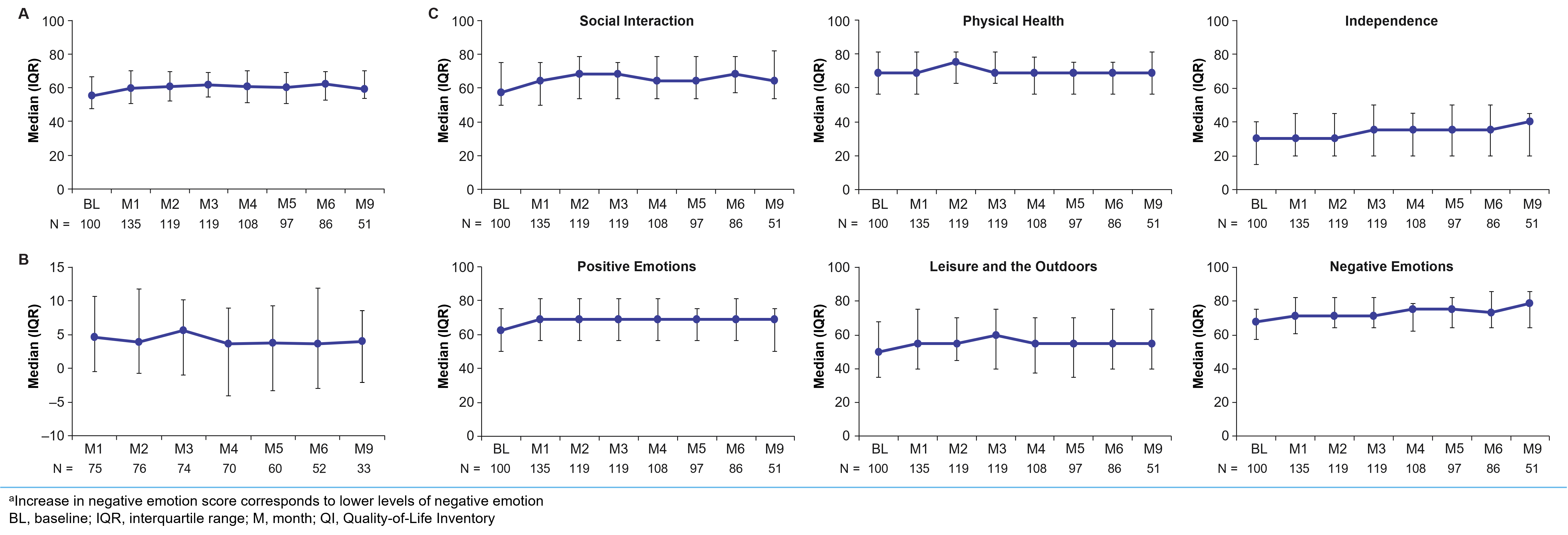
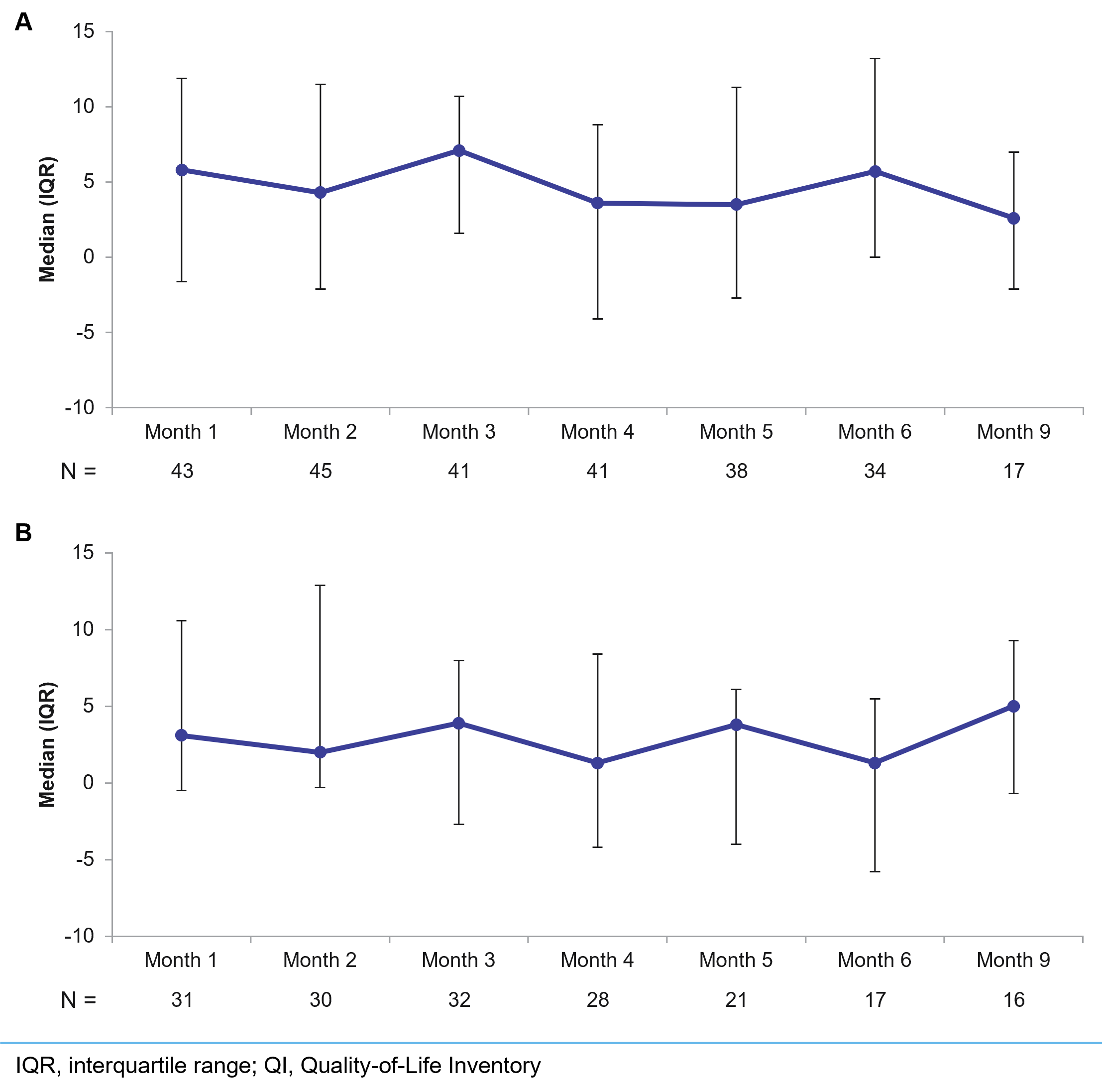
Quality-of-Life Improvements
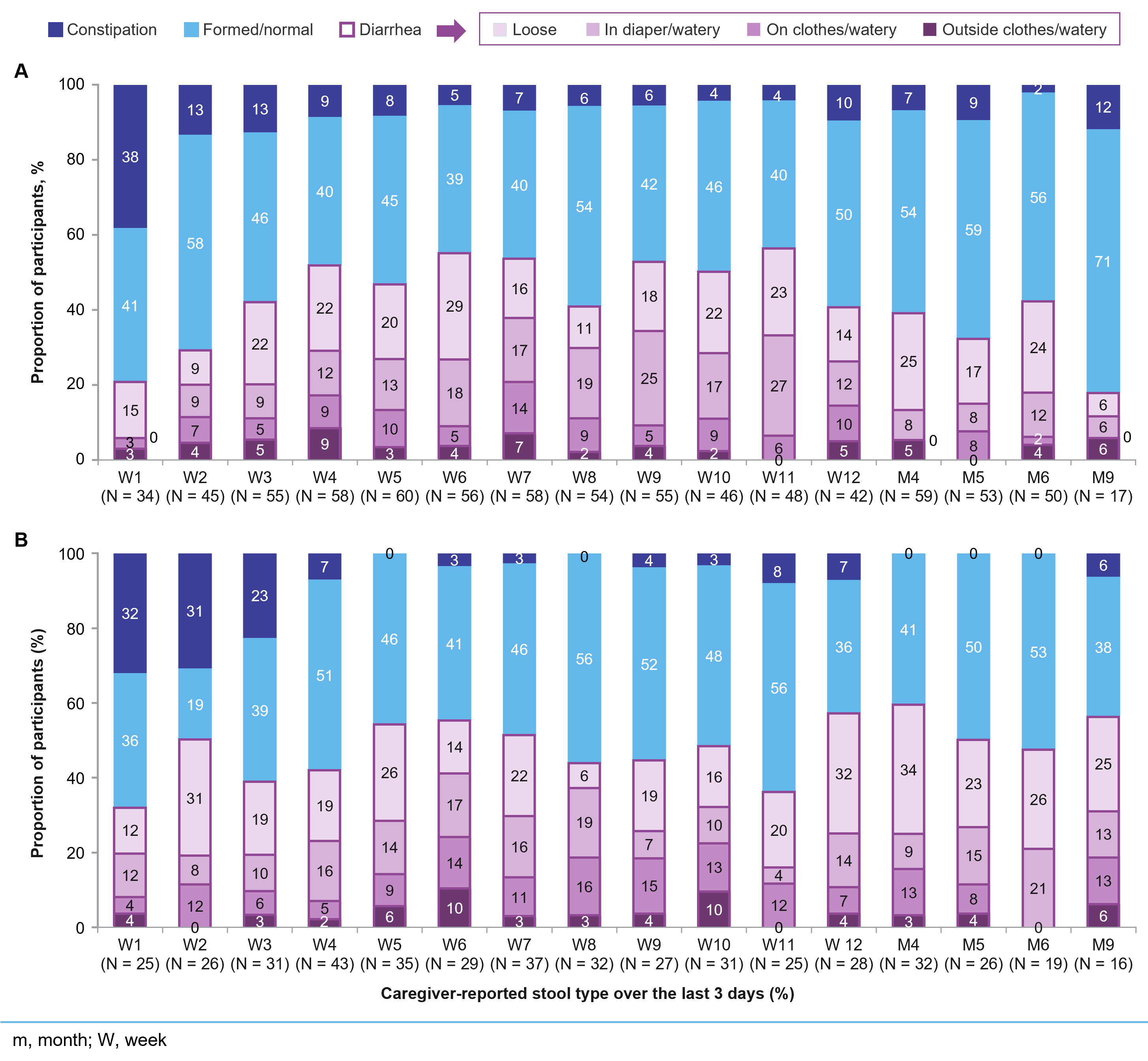
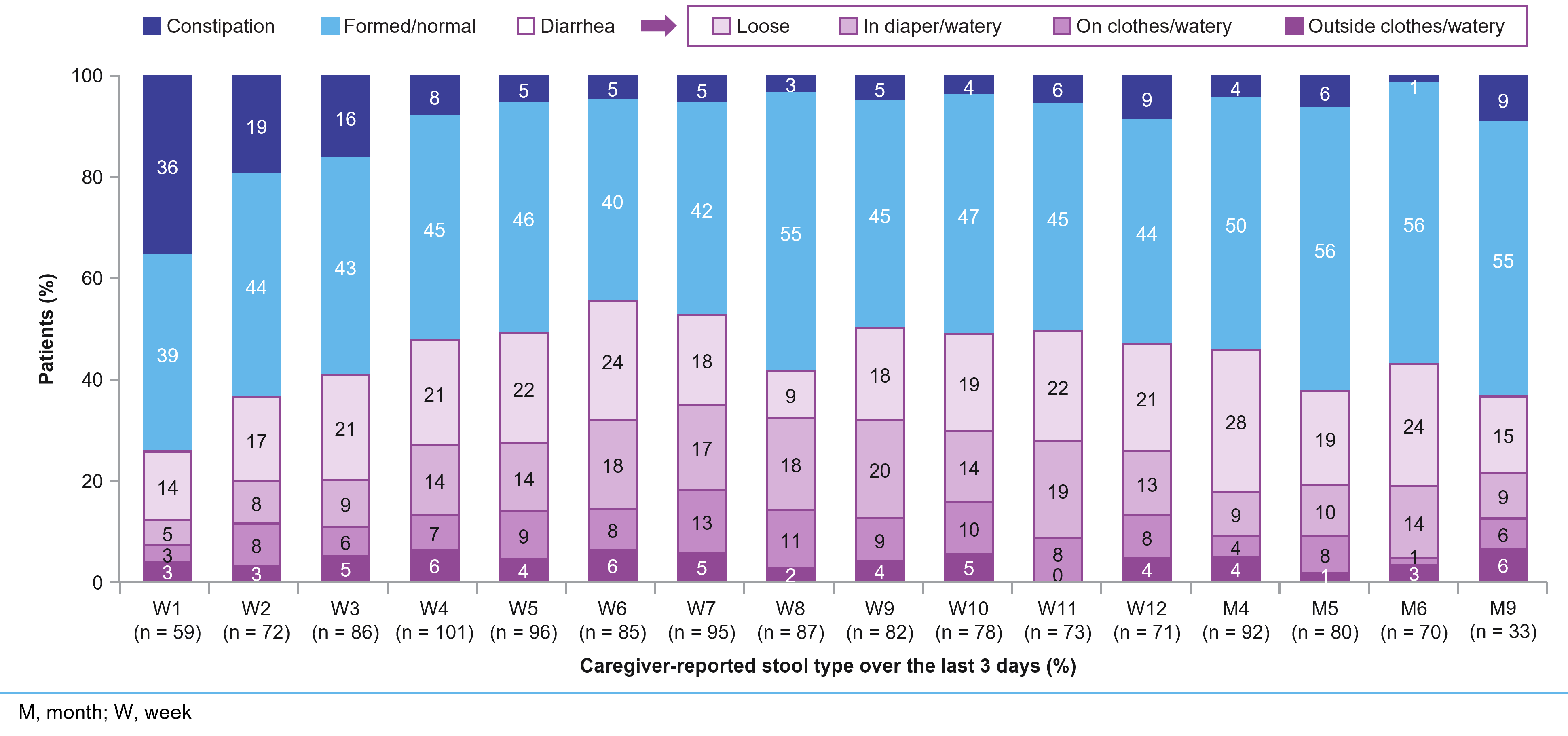
GI Health After Initiation of Trofinetide
Figure 1. Comorbidities of cases with RTT
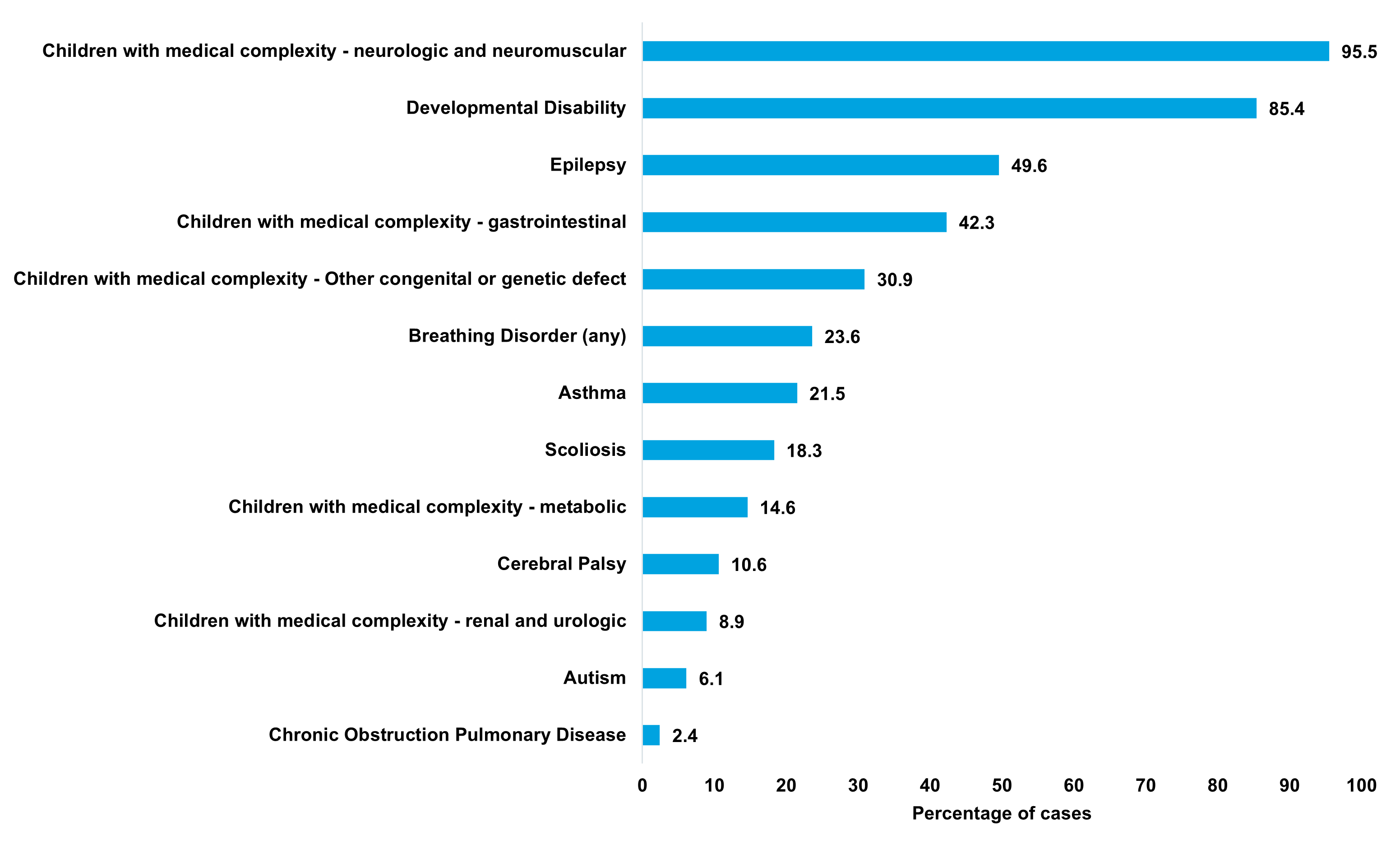
Figure 2. Incidence and prevalence of RTT

Figure 3. Healthcare resource utilization of cases with RTT in Ontario
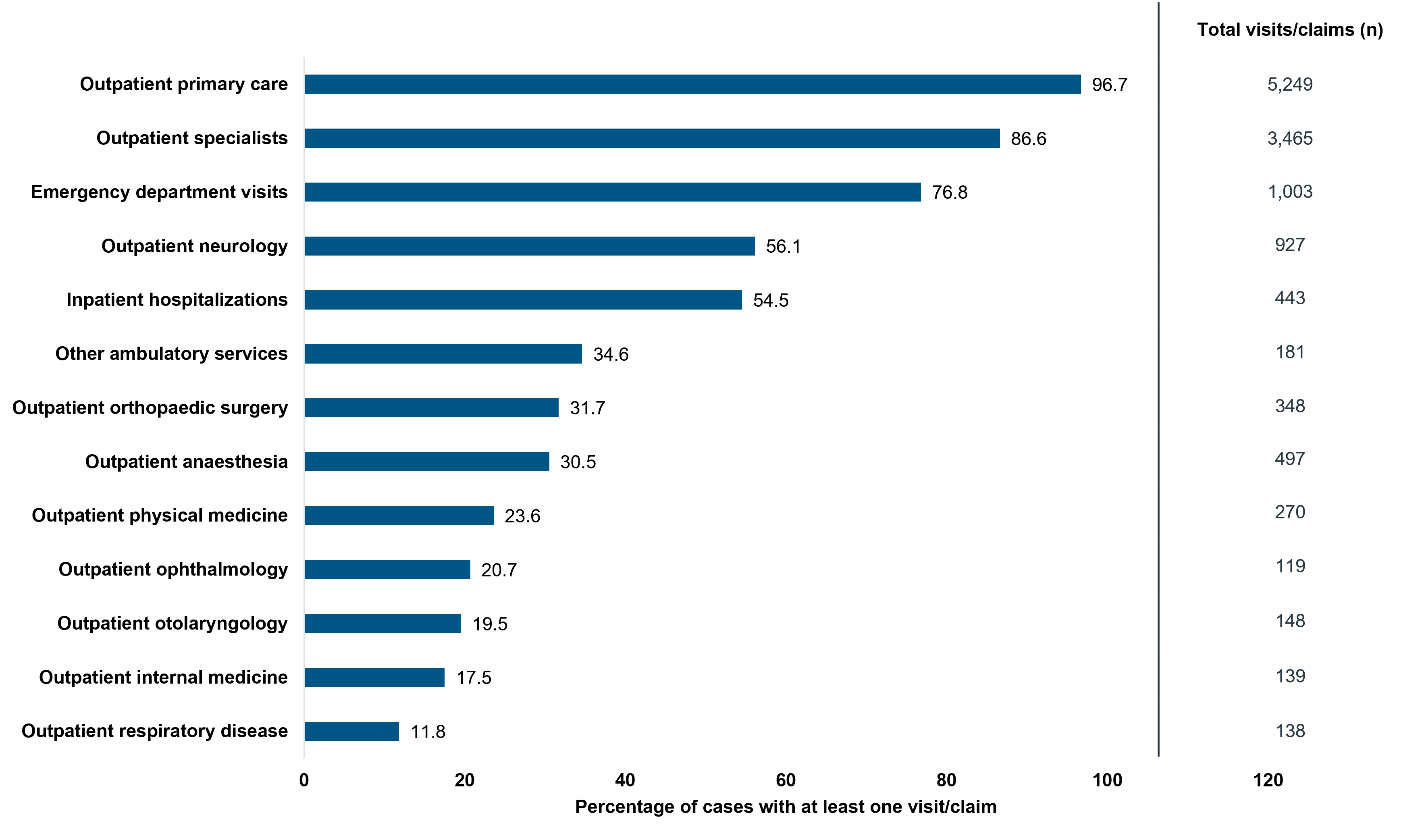
Figure 4. All-cause drug claims for RTT cases in Ontario
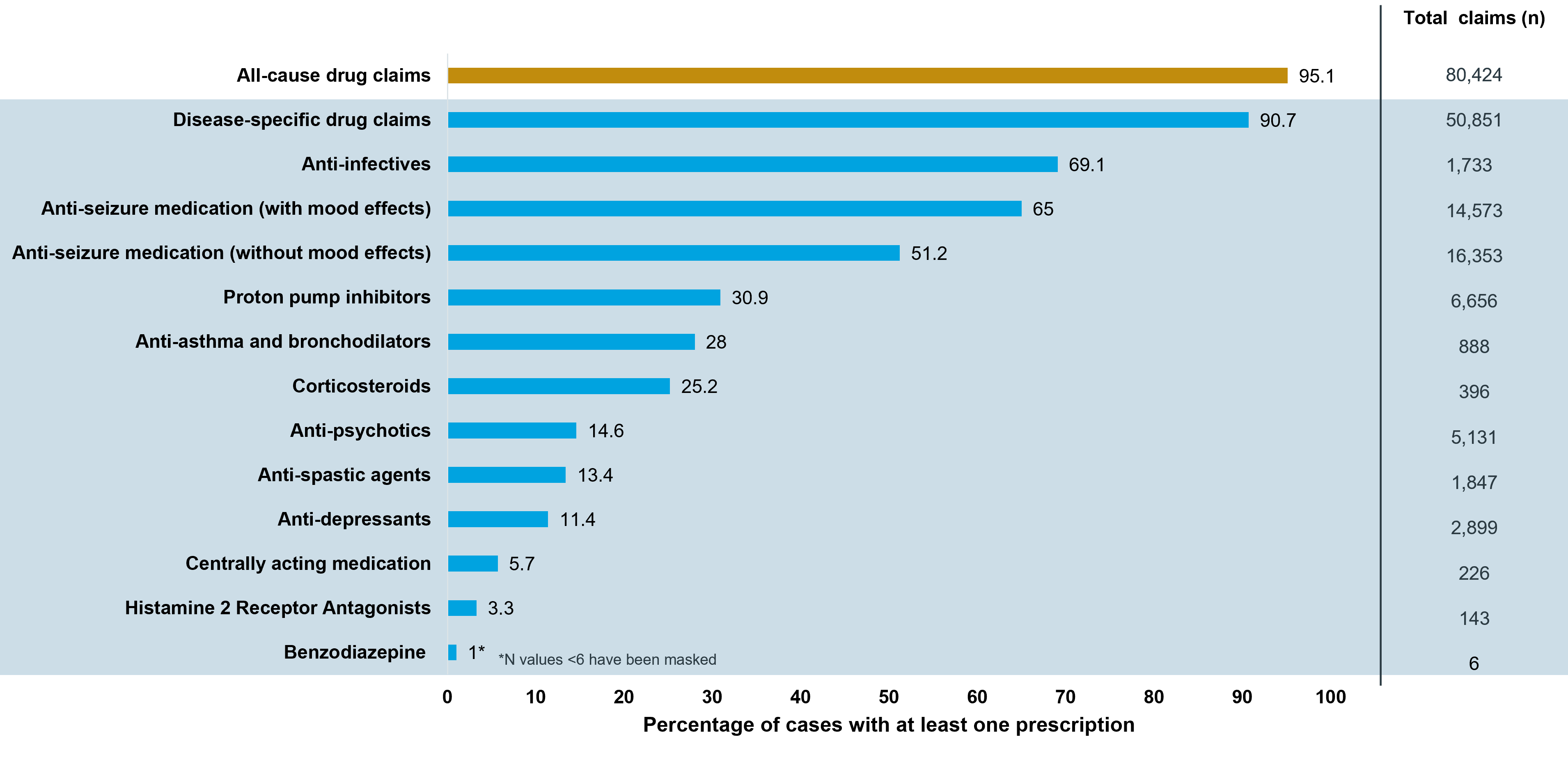



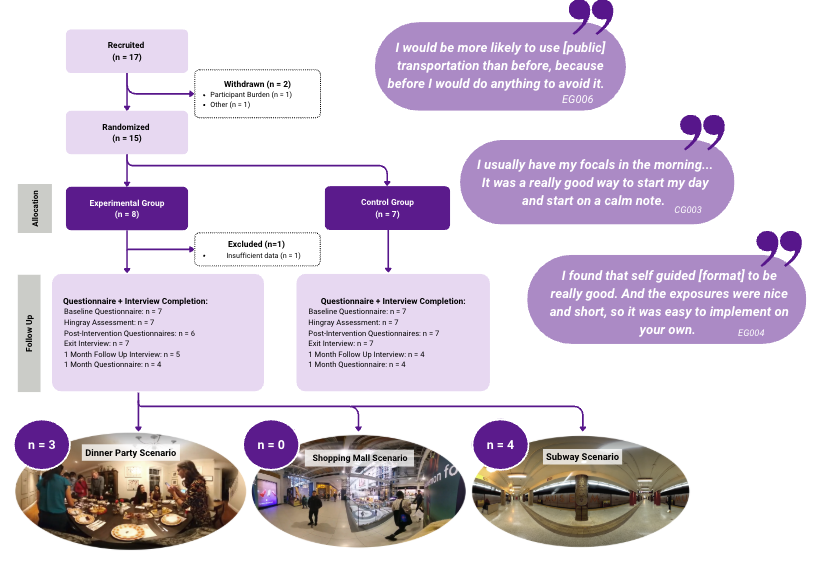


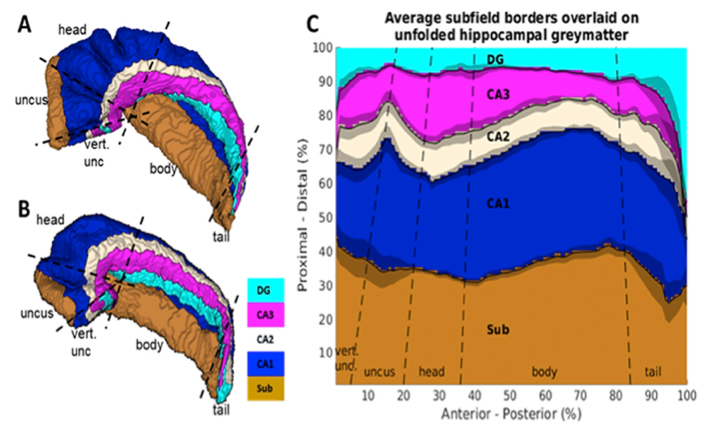
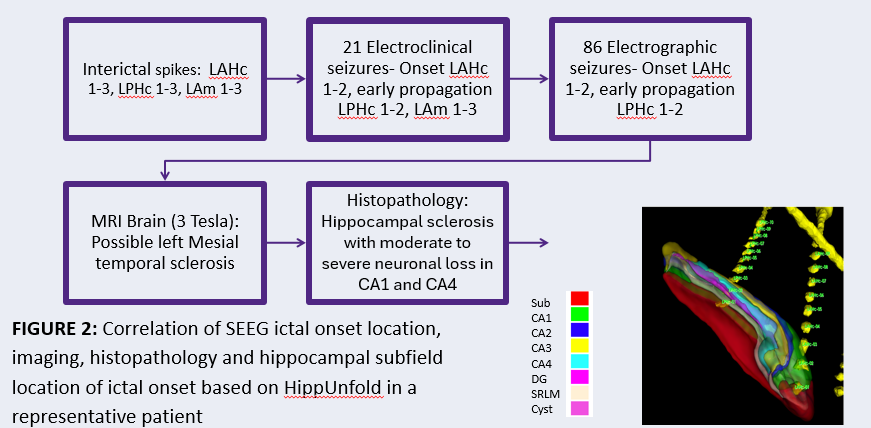
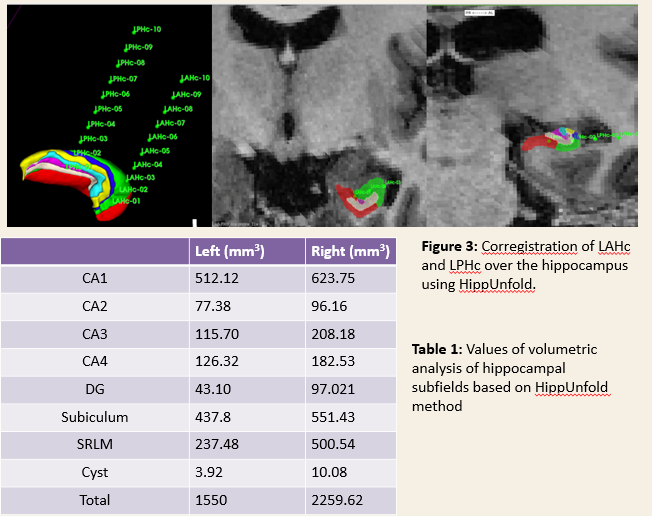
Figure 1: a-b HippUnfold representation of the hippocampus with segmentation of the different regions. c. Unfolded hippocampus reconstruction.
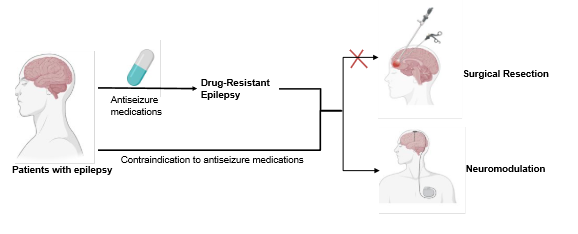
1) Drug-resistant temporal lobe epilepsy
2) SEEG investigation
2) High-resolution MRI (3T or 7T)
3) Mesial temporal epilepsy captured with SEEG
4) Underwent temporal lobectomy with a minimum of 6 months follow-up.
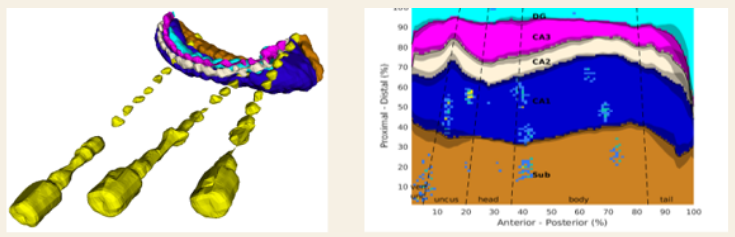
From the 167 consecutive patients investigated with SEEG, so far, we have collected 25 patients who fulfil the criteria.
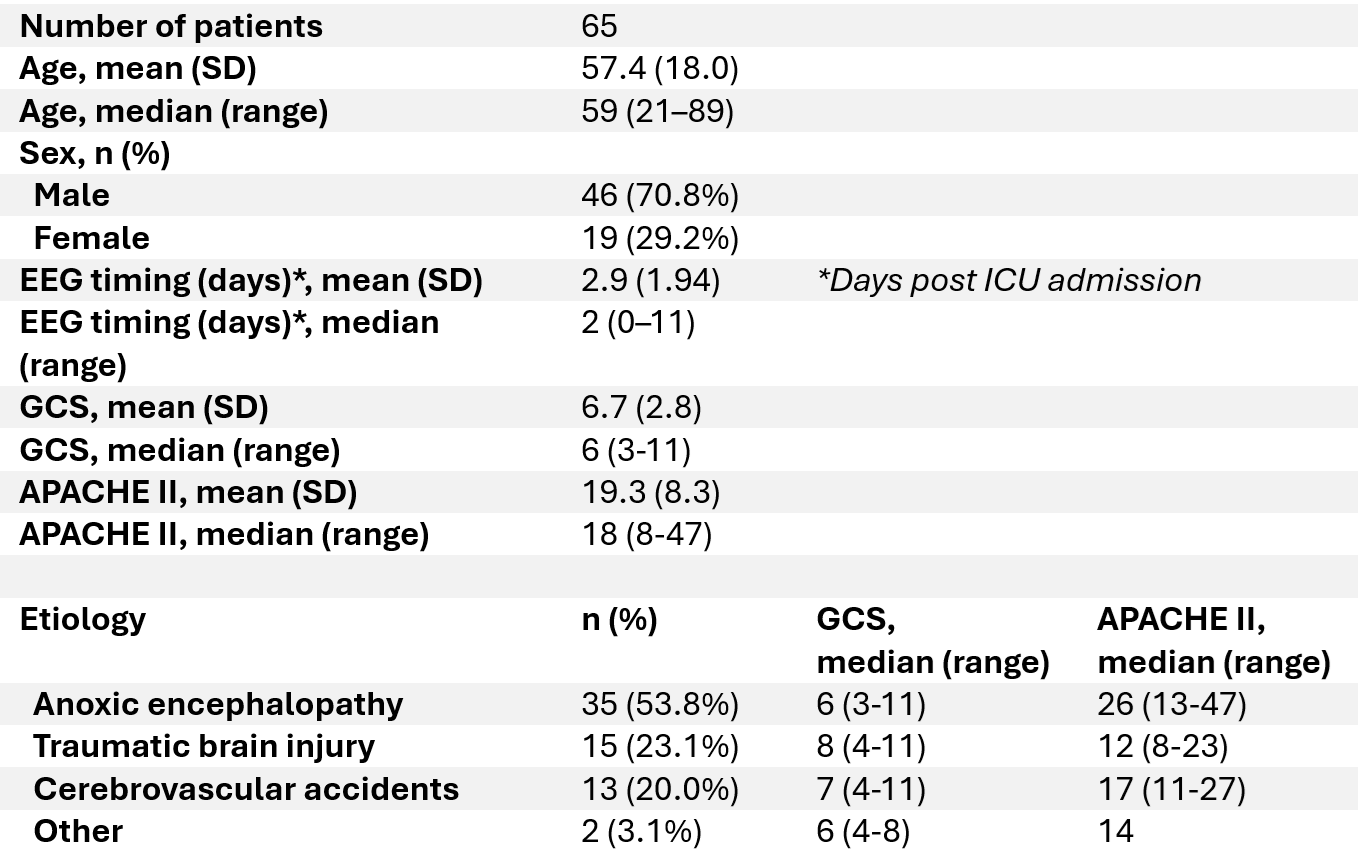
Predicting neurological recovery in patients with severe brain injury remains challenging. Continuous EEG monitoring can detect malignant patterns but is resource-intensive, and its role in long-term functional outcome prediction is unclear. This study evaluates the utility of parameterized short-segment EEG, acquired via EEG cap, in predicting neurological recovery.
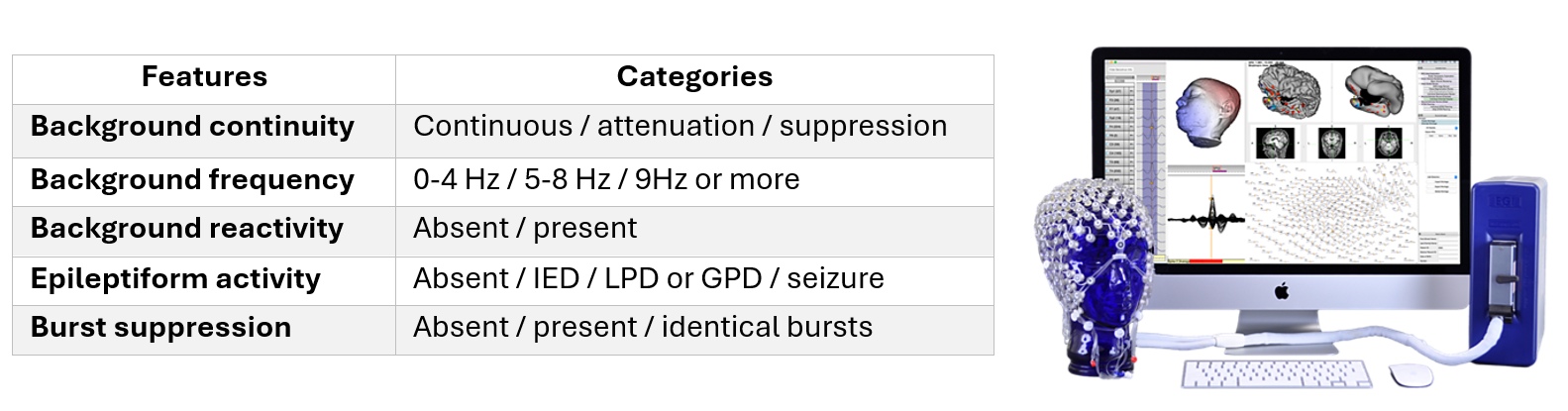
We analyzed short-segment high-density EEGs from 65 patients in the NET-ICU cohort1 who presented with acute neurological injury and a disorder of consciousness. EEGs were recorded using a 128-channel system (Electrical Geodesics Inc., Eugene, OR, USA) with sponge-based electrode nets, enabling rapid setup in approximately 10 minutes. Data were subsequently downsampled to the standard 19-channel bipolar montage and preprocessed into conventional clinical formats. Five visual EEG features, selected based on their established associations with neurological outcomes, were extracted according to the 2021 ACNS Critical Care EEG terminology.2,3
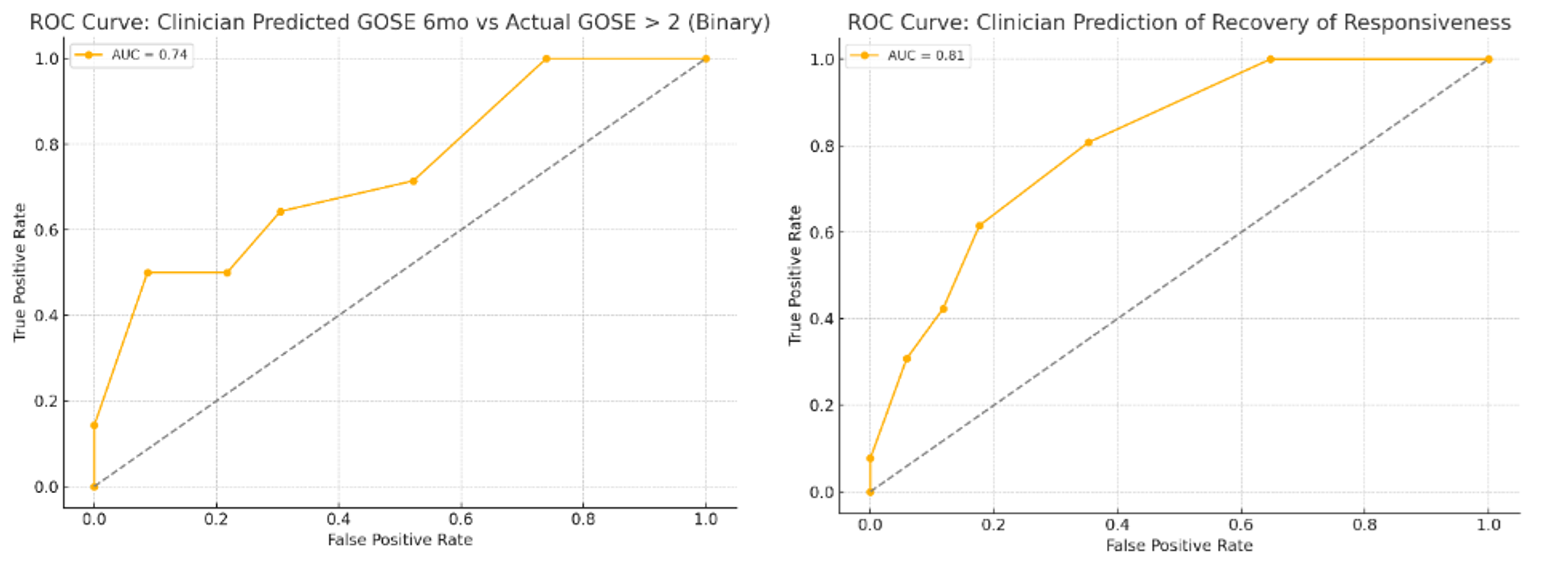
Logistic regression (LR) and random forest classifier (RFC) models were developed to predict two outcomes: (1) recovery of responsiveness (defined as the ability to follow 1- or 2-step commands during or after ICU admission) and (2) 6-month outcome on the Glasgow Outcome Scale – Extended (GOSE). Models were trained using EEG features alone or in combination with clinician-predicted outcomes. We hypothesized that incorporating EEG features would enhance the discriminative power of neuroprognostic models. Given the anticipated nonlinearity and interdependence among EEG features, we further hypothesized that the RFC model would outperform LR in predictive performance.
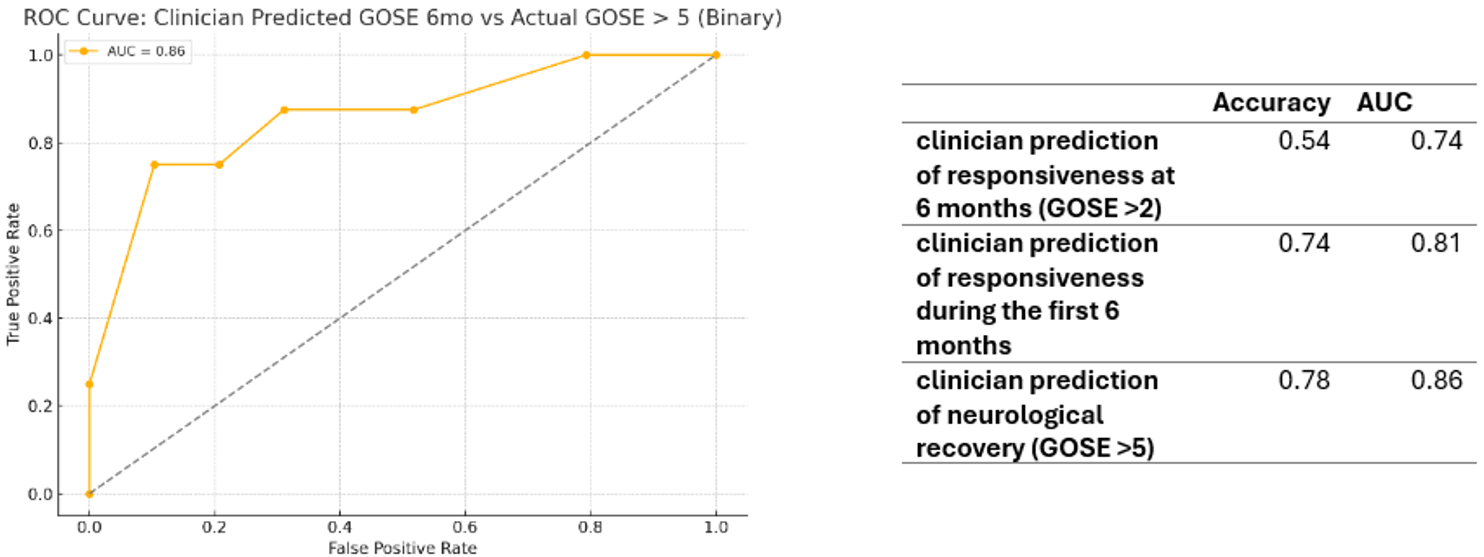
Clinician predictions showed good discriminative ability for recovery of responsiveness (AUC 0.74 for GOSE >2; 0.81 for recovery of responsiveness), and higher accuracy when predicting more favorable long-term outcomes (AUC 0.86 for GOSE >5).
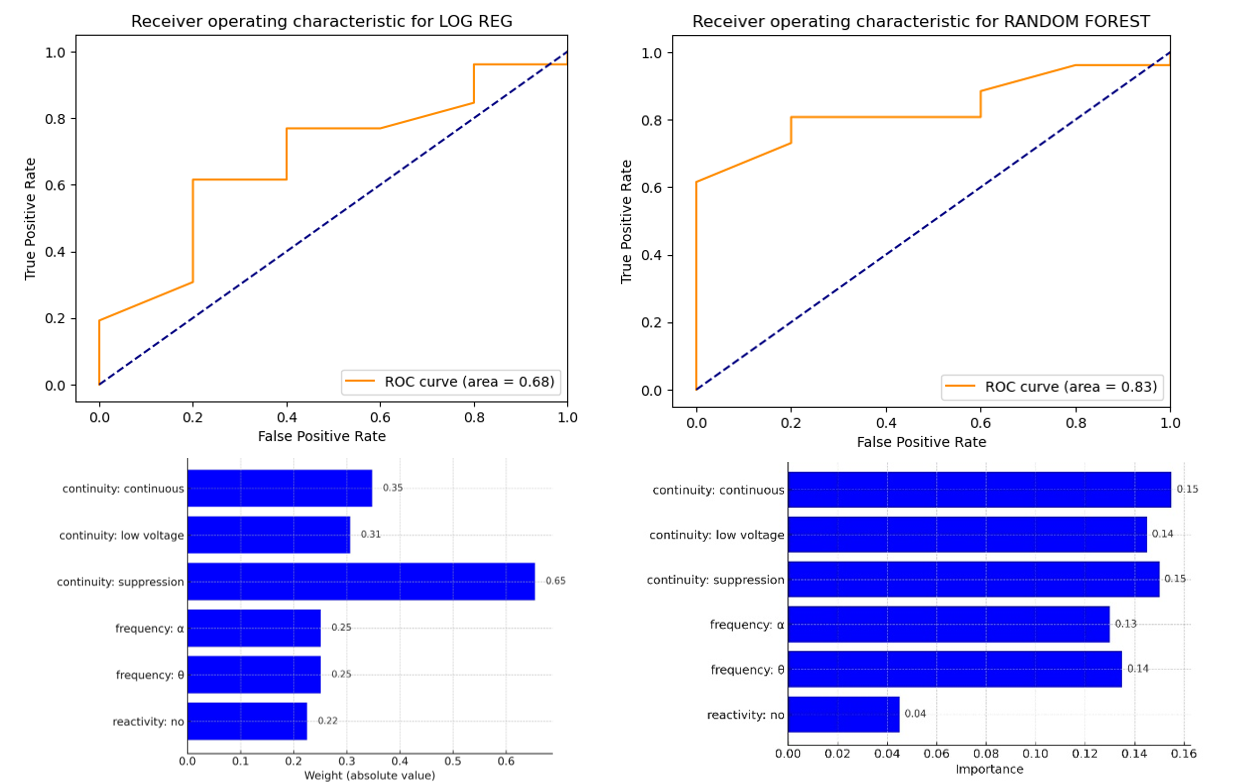
Combining clinician prediction of Glasgow Outcome Scale–Extended (GOSE) scores with EEG features improved overall predictive performance (accuracy 0.87-0.96; AUC 0.93-1).
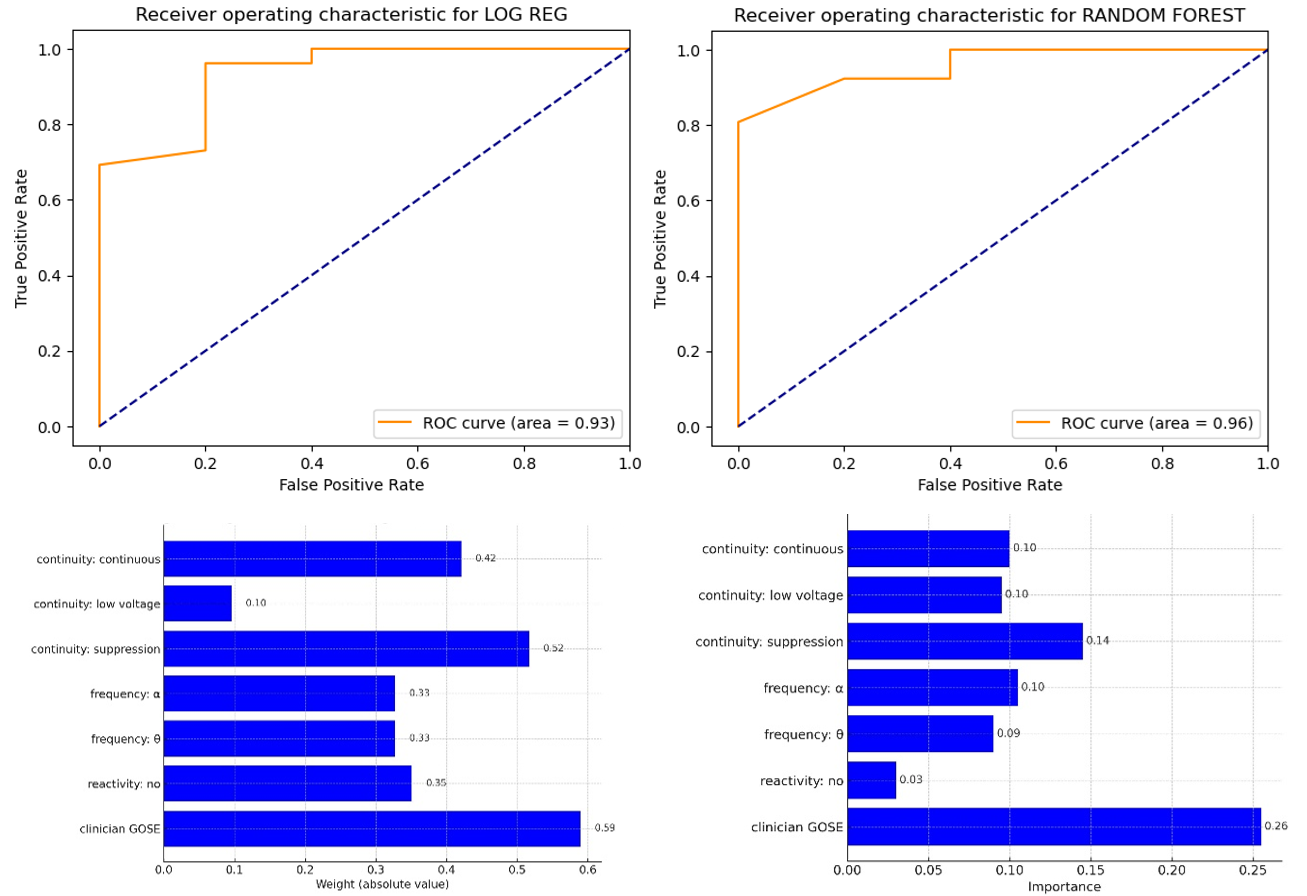
Standardized EEG features collected using caps that require minimal training and technician support can improve the accuracy of neurological recovery predictions in patients with acute severe brain injury. Among these features, background continuity and frequency—both readily extractable using existing EEG preprocessing software—carry the most prognostic weight. These findings support the use of machine learning approaches that account for nonlinear relationships among features. Together, these results suggest that accessible EEG implementations, combined with robust machine learning models, can provide clinically meaningful and scalable prognostic information for critical care environments.

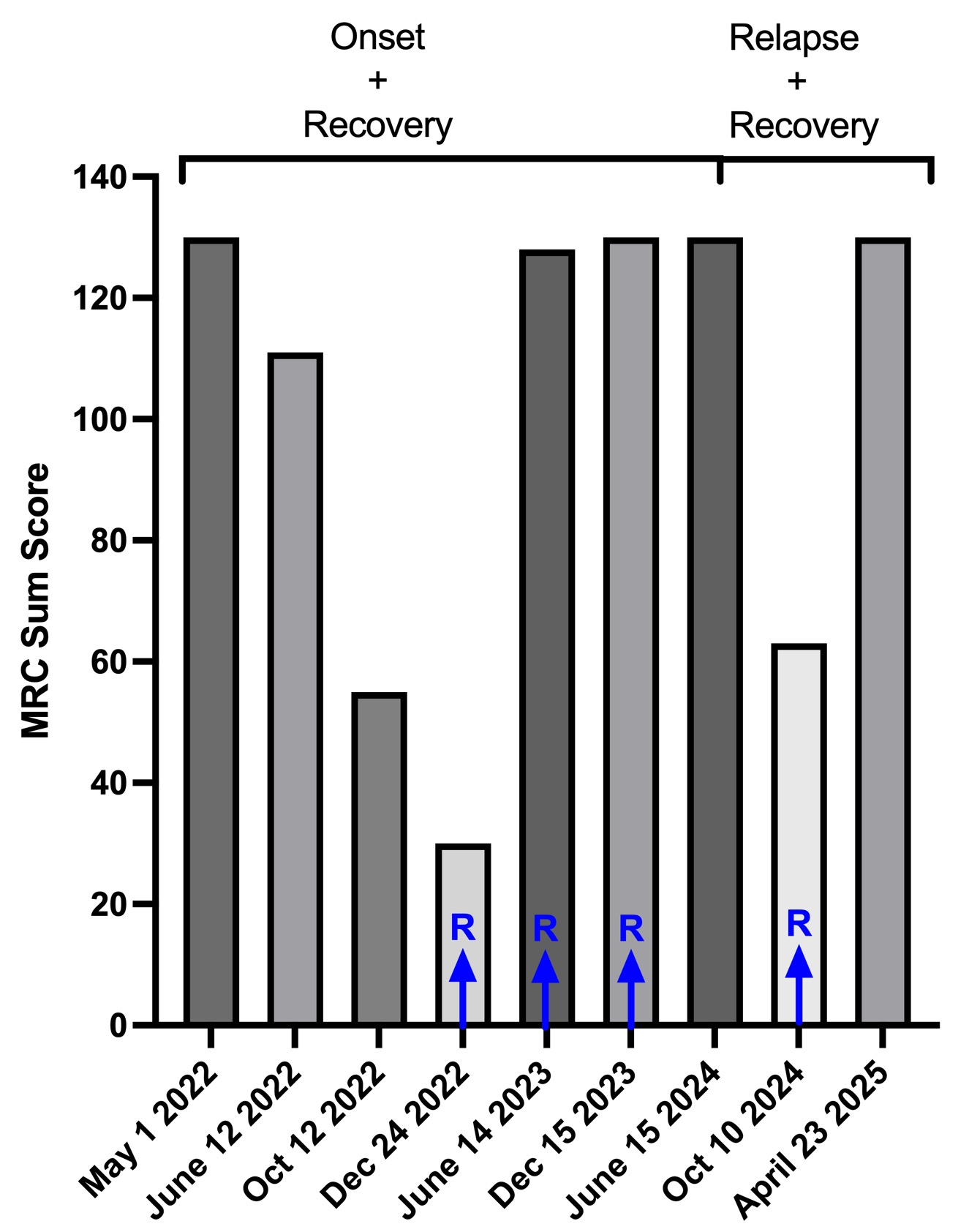
Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) is a rare, acquired auto-inflammatory polyneuropathy with an estimated incidence of up to 2 per 100,000. It generally presents in a symmetric, proximal and distal, sensorimotor fashion (1). Immunosuppression and immunomanipulation are treatment modalities. Pediatric CIDP has distinguishing features:
(1 ) 5-fold rarer compared to adult disease (0.4/100,000),
(2) motor predominant,
(3) relapse-prone,
(4) rapidly progressive, and
(5) a more favorable long-term prognosis.
We present a case of a 14-year-old male with severe progressive CIDP who became refractory to steroid and IVIg but responded to rituximab. Upon withdrawing therapy at age 16 he had a severe relapse which subsequently responded to the reinstitution of rituximab.



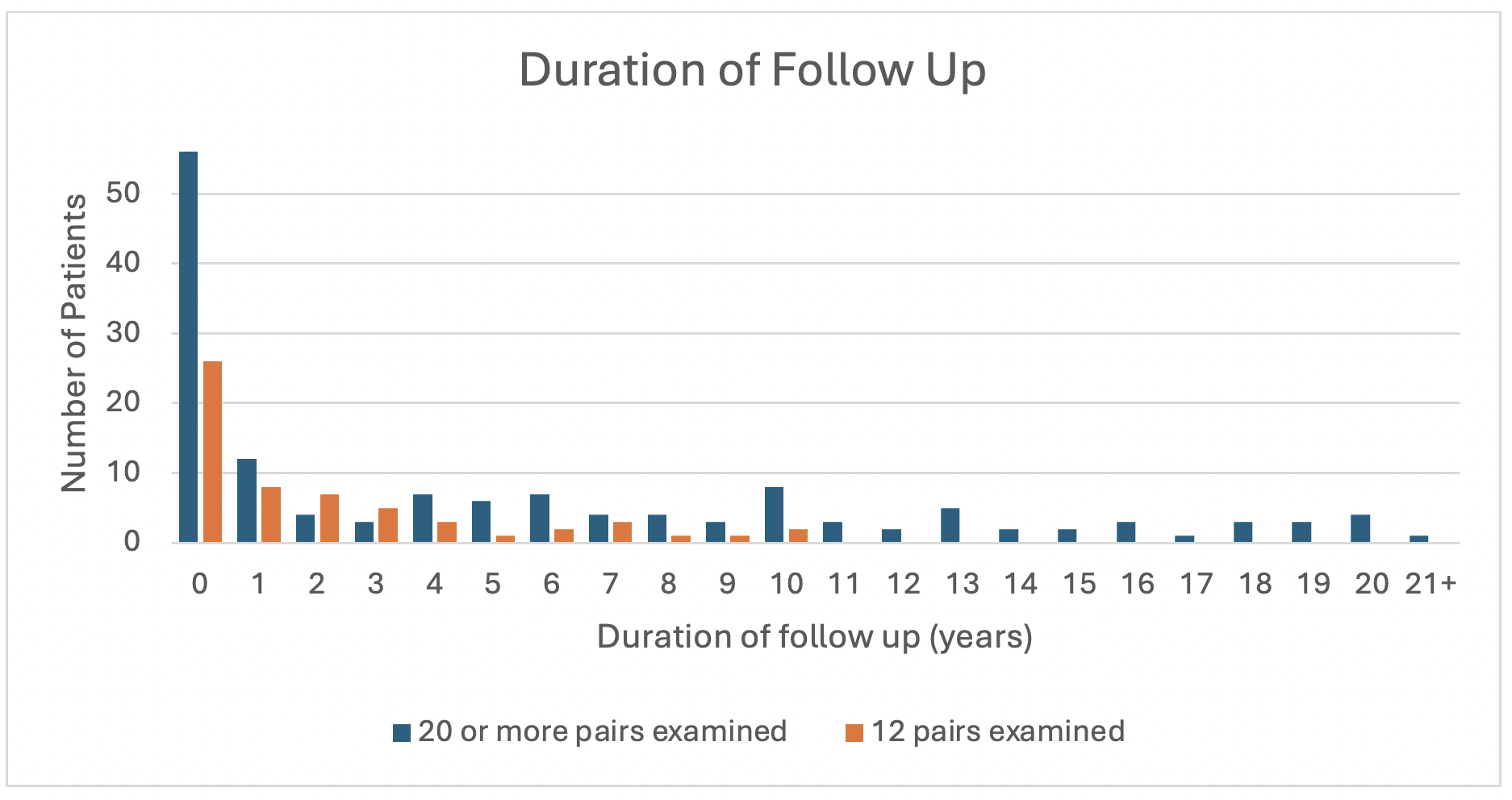
Analysis of 20 muscle fiber action potential pairs is the traditional standard when using single fiber EMG (SFEMG) to diagnose myasthenia gravis (MG). Some studies show that fewer pairs are needed if results are normal. We examined what impact this might have on long-term outcomes.
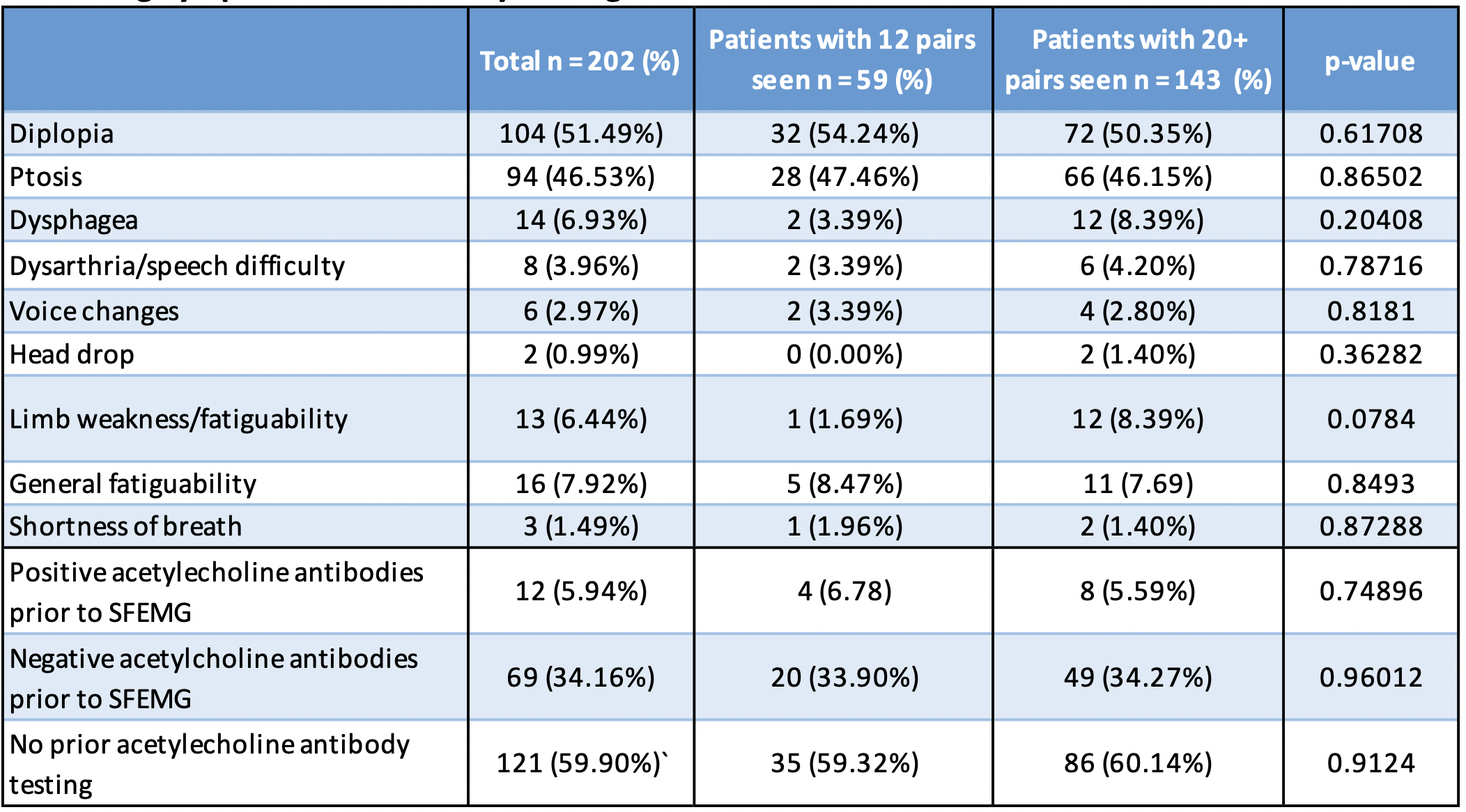
Presenting Symptoms and Antibody Testing Status
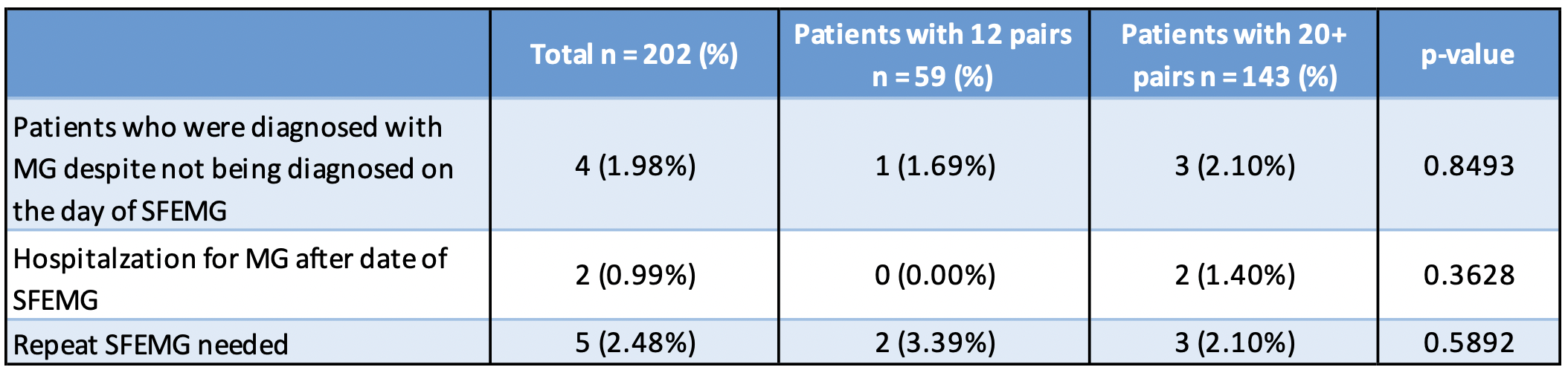
MG Diagnosis Outcome

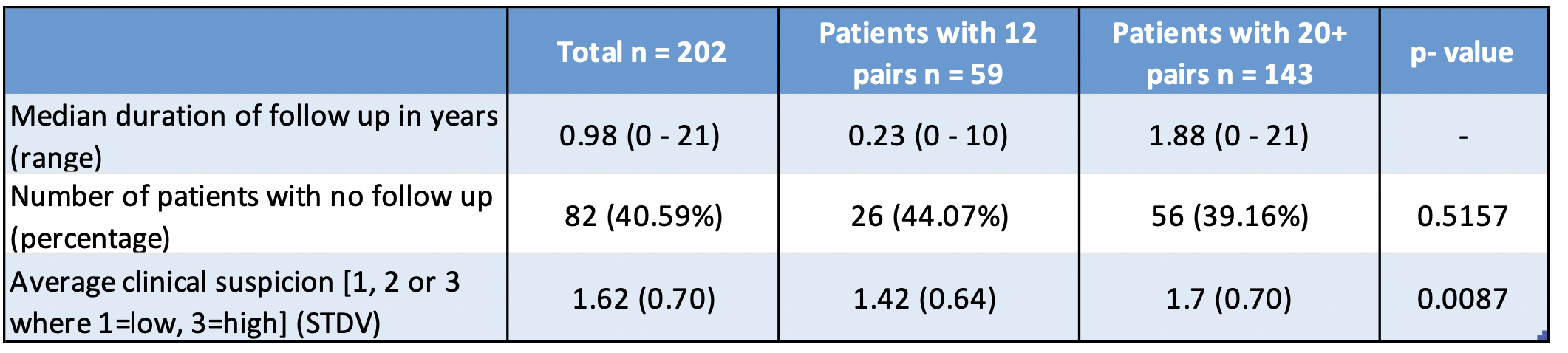
Discussion
Conclusion
|
Subset |
Value |
Metric |
|
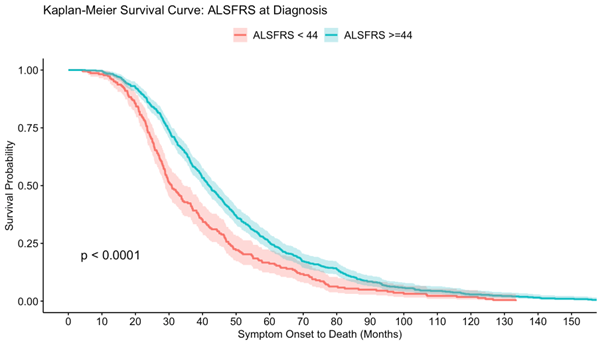
ALSFRS-R at Diagnosis |
44.7 (5.46) |
Mean (SD) |
|
ALSFRS-R >=44 |
1131 (72.3%) |
N (%) |
|
ALSFRS-R <44 |
434 (27.7%) |
N (%) |
|
FVC % Predicted at Baseline |
84.2 (23.3) |
Mean (SD) |
|
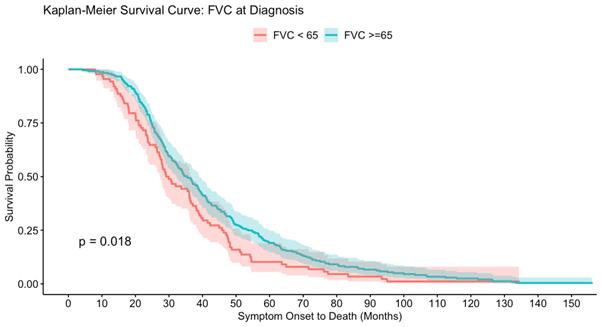
FVC (%) >=65 |
548 (78.3%) |
N (%) |
|
FVC (%) <65 |
152 (21.7%) |
N (%) |
|
Time from Sx Onset3 |
116 (51.5) |
Mean (SD) |
|
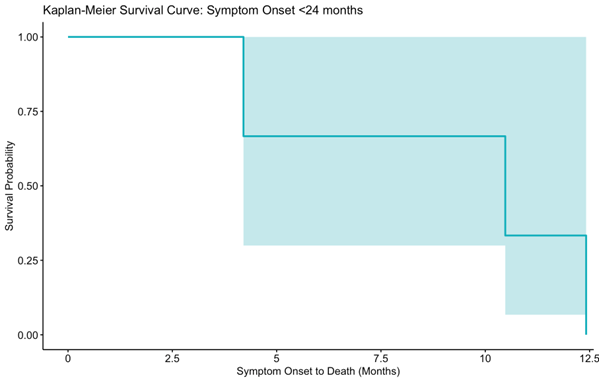
Time <24 months |
52 (3.34%) |
N (%) |
|
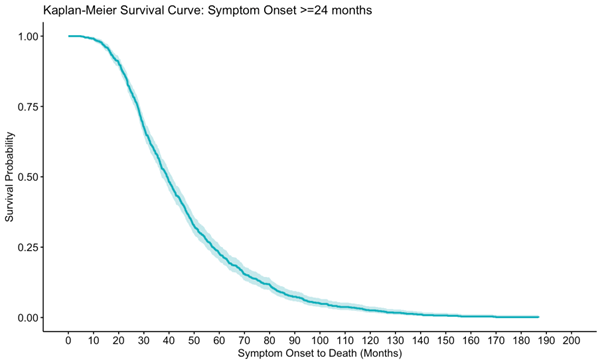
Time >=24 months |
1507 (96.7%) |
N (%) |
|
Grouping |
Mean (SD) |
Median (0.95 LCL, UCL) |
|
Symptom Onset |
|
|
|
<24 Months (N=3) |
9.03 (2.02) |
10.5 (4.20, NA) |
|
>=24 Months (N=826) |
46.2 (0.95) |
39.3 (37.1, 41.3) |
|
ALSFRS at Diagnosis |
|
|
|
ALSFRS <44 (N=242) |
36.6 (1.74) |
30.9 (28.8, 34.5) |
|
ALSFRS >=44 (N=579) |
50.8 (1.46) |
41.8 (39.7, 44.6) |
|
FVC at Diagnosis |
|
|
|
FVC <65 (N=88) |
35.5 (2.27) |
29.5 (27.2, 36.5) |
|
FVC>=65 (N=241) |
42.9 (1.67) |
35.4 (32.3, 39.0) |
Rationale and Background
Objective
Methods
Table 1. Physician-reported gMG patient demographics and clinical characteristics
|
|
n = 46 |
|
Age at time of survey (years); mean (SD) |
58.1 (14.7) |
|
Gender; Male; n (%) |
24 (52.2) |
|
Ethnicity; White/Caucasian; n (%) |
38 (82.6) |
|
Total number of patients with a known time since diagnosis of gMG (years); n* |
45 |
|
Time since diagnosis of gMG (years); mean (SD) |
3.4 (3.1) |
|
Antibody status, AChR+; n (%) |
41 (89.1) |
|
Antibody status, MuSK+; n (%) |
5 (10.9) |
|
Total number of patients with employment status reported; n* |
45 |
|
Main employment status at time of survey, working part-time, on sick leave, unemployed, retired; n (%) |
29/45 (64.4) |
|
Patients with employment status reported as working part-time, on sick leave, unemployed, retired due to gMG; n (%) |
6/45 (13.3) |
|
gMG; Generalized myasthenia gravis, SD; Standard Deviation, AChR+; Acetylcholine receptor positive, MuSK+; Muscle-specific kinase positive *n=1 don’t know excluded |
|
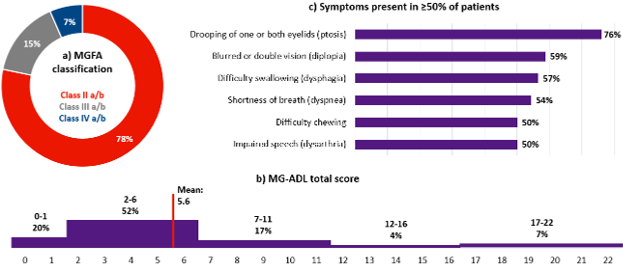
Figure 1. Physician-reported MGFA classification (a), MG-ADL total score (b) and most frequent symptoms of gMG patients (c)
Results
Figure 2. Myasthenic crises and symptom exacerbations experienced by gMG patients (n=43)
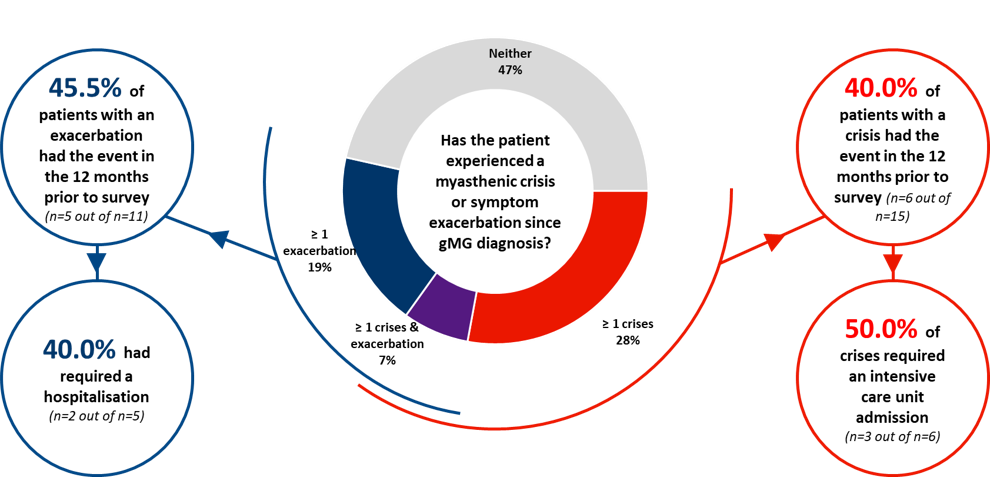
gMG: generalised myasthenia gravis; n=3 don’t knows excluded
Table 2. gMG treatment overview (n=46)
|
Number of maintenance treatment lines, mean (SD) |
1.8 (0.9) |
|
Maintenance treatment lines since diagnosis, n (%) |
|
|
1 line |
22 (47.8) |
|
2 lines |
14 (30.4) |
|
3 lines |
9 (19.6) |
|
4 lines |
1 (2.2) |
Treatment line was determined by the physician as the start, stop or switch of any individual therapy, gMG: generalised myasthenia gravis, SD; Standard Deviation
Figure 3. gMG maintenance treatment at time of survey (n=45)
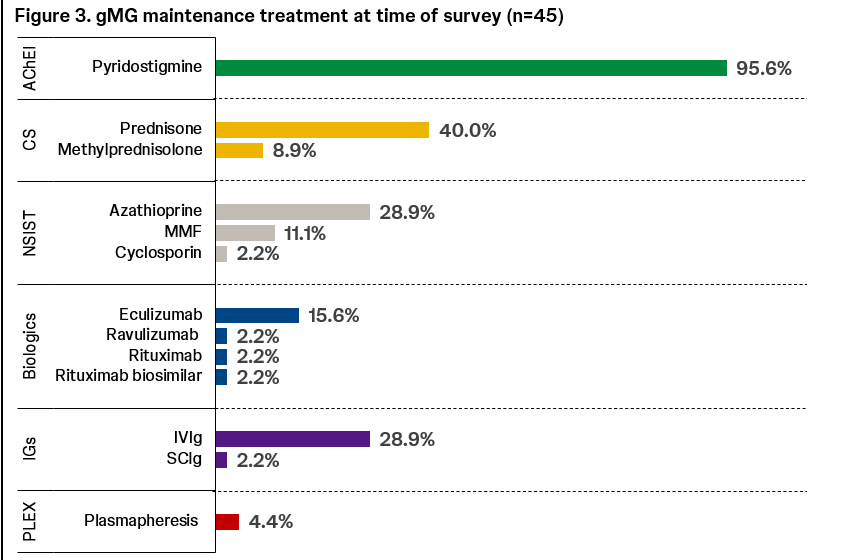
Treatments prescribed specifically for maintenance / chronic use only as reported by the physician at the time of survey. gMG: generalised myasthenia gravis, AChEI: acetylcholinesterase inhibitors, CS: corticosteroids, NSIST: non-steroidal immunosuppressants, MMF: mycophenolate mofetil, IVIg: intravenous immunoglobulins, SCIg: subcutaneous immunoglobulins; PLEX: plasmapheresis
METHODS
RESULTS
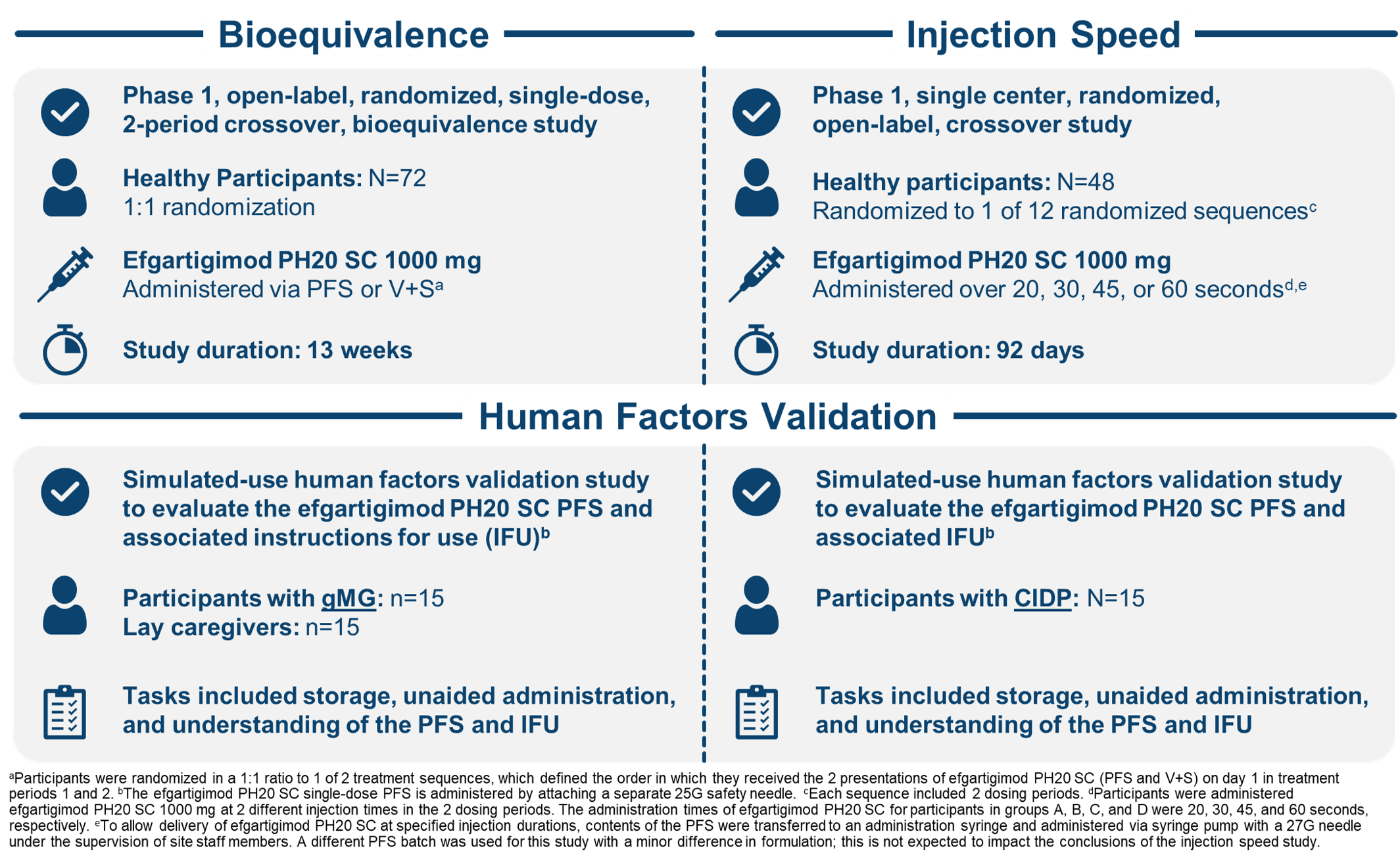
Bioequivalence Study in Healthy Participants
Design: Healthy participants were randomized to receive a single injection of efgartigimod PH20 SC via PFS or V+S, and switched to receive the other treatment ≥2 weeks after the initial 3-week treatment period (≥5 weeks total between injections)
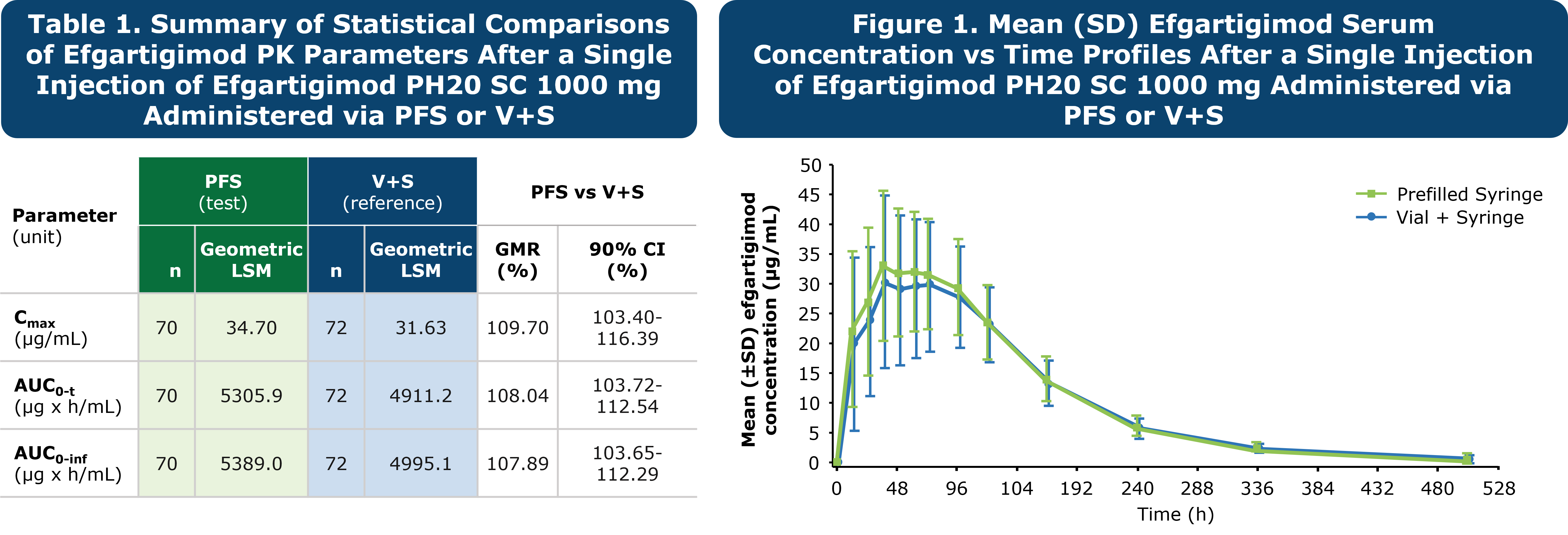
Results: Following a single administration of efgartigimod PH20 SC via PFS or V+S, efgartigimod serum concentrations indicated that the 90% CI around the GMR of Cmax and AUC0-inf was within the
predefined bioequivalence criteria of 80.00% to 125.00% (Table 1; Figure 1)
Safety: The frequency of AEs was similar between participants in both groups. The majority of
AEs were mild to moderate in severity; most frequently reported AEsa were injection site discoloration,
injection site reaction, and injection site hemorrhage. No SAEs or deaths were seen in the study
aOccuring in ≥10% of participants in either treatment group.
Injection Speed Study in Healthy Participants
Design: Healthy participants were randomized to receive efgartigimod PH20 SC 1000 mg in 1 of 12 injection sequences, each with 2 dosing periods. In each dosing period, participants received
injections over 20, 30, 45, or 60 secondsa
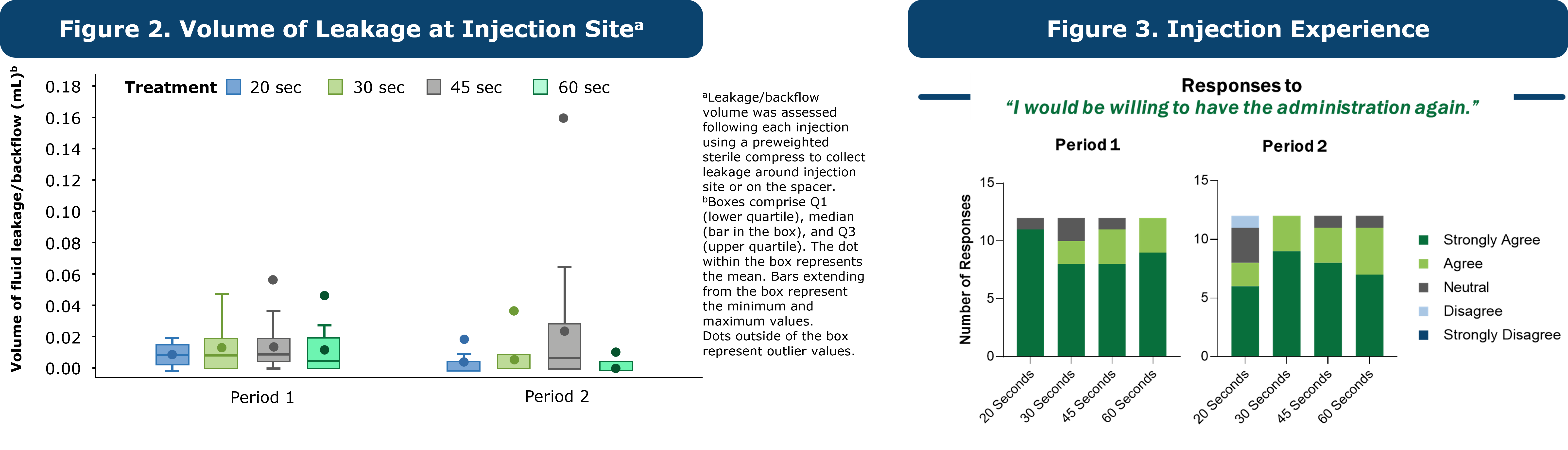
Results: There was no meaningful difference in the mean fluid leakage/backflow volume at the injection site across the injection time groups (Figure 2). All participants received at least 90%b of the entire injection volume across the injection time groups. Overall, the majority (>87%) of participants either strongly agreed or agreed to have the administration again 1 hour after injection (Figure 3). No clear preference toward an injection time group was concluded
Safety: All AEs were mild in severity, except for 2 moderate AEs of dysuria and pericoronitis in 2 (4.2%;
2 events) participants. No participants died during the study. Local injection-site scoring was similar and consistent across the injection time groups for the 3 assessed categoriesc at all time points
aTo allow delivery of efgartigimod PH20 SC at specified injection durations, contents of the PFS were transferred to an administration syringe and administered via syringe pump with a 27G needle under the supervision of site staff members.
A different PFS batch was used for this study with a minor difference in formulation; this is not expected to impact the conclusions of the injection speed study. b90% of efgartigimod PH20 SC volume administered is considered an entire dose. cThe 3 assessed categories of local tolerability included erythema, swelling, and induration.
Human Factors Validation Studies in gMG and CIDP
Design: In a simulated-use environment mimicking a home setting, participants (N=30 in the gMG study [n=15 patients with gMG and n=15 lay caregiversa]; N=15 in the CIDP study) were given access to the IFU and materials supplied with the PFS. No training was provided. Participants were then tasked with performing an unaided injection and were questioned on their knowledge of the PFS (Table 2)
Results: 100% of participants (N=30/30 in the gMG study; N=15/15 in the CIDP study) were successful in preparing and delivering the full dose in an average of 30 seconds. Participants and lay caregivers had no difficulty handling the syringe and successfully identified critical information on the instructions. Residual risks were as low as possible and were not tied to the design of the prefilled syringe or instructional materials
aAdults who care for a family member with gMG (n=12) or CIDP (n=3).
CIDP is a rare immune-mediated demyelinating neuropathy that has significant phenotypic variability.1 Despite extensive efforts, a unifying immunopathological mechanism remains elusive, likely due to etiological heterogeneity among the variant presentations.2 This is best exemplified by the identification of nodal/paranodal antibodies, such as neurofascin 155 (NF155) in a small subgroup of CIDP patients, who present with a distinct phenotype and embody a poor response to IVIG.3–5
We present the case of a 39-year-old male who presented with a 2-year history of progressive stocking-glove sensory loss and sensory ataxia. Electrodiagnostics confirmed an acquired demyelinating neuropathy, with serum anti-NF155 IgG4. His case was refractory to standard immunomodulatory therapy, including adequate trials of IVIG, steroids, azathioprine, and rituximab. He also had a non-therapeutic trial of PLEX, methotrexate, and tacrolimus.
A 39 y/o male was initially seen in 2018 for a 2-year history of glove and stocking distribution sensory disturbance. He was previously healthy with the exception of sleep apnea. He was born in the Philippines without any significant family history of neuromuscular disorders. He did not have any weakness at that time, but he did have difficulty with sports, particularly running, jumping, and endurance. His sensory examination revealed a length-dependent decrease in his vibration sense up to his ankles and pinprick sensation up to his mid-shins. His Achilles reflex was 0 bilaterally; otherwise, biceps, triceps, and patellar reflexes were noted to be 2+. His tandem walking and Romberg were normal on initial assessment.
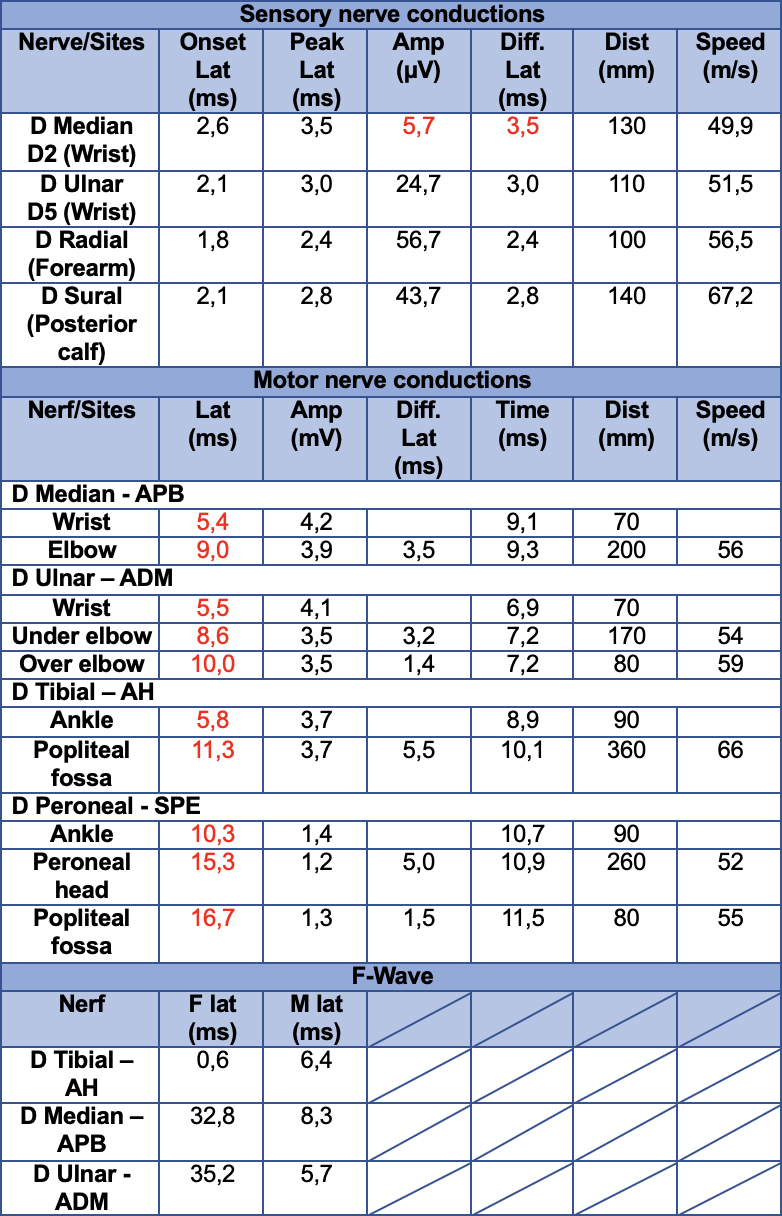
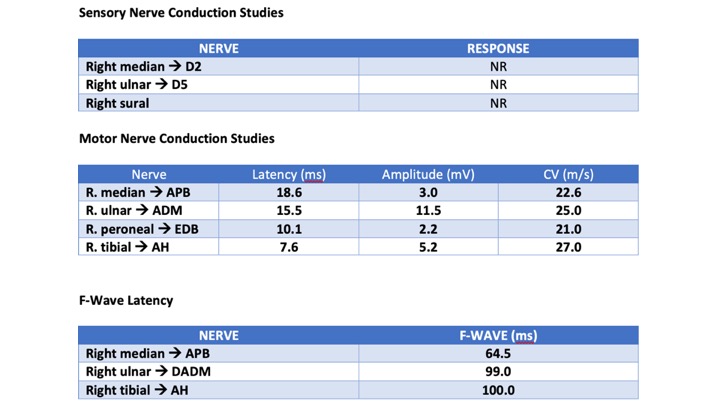
His initial nerve conduction studies (NCS) (Table 1) were consistent with an acquired demyelinating process.
Given his presentation, suspicion was high for an acquired demyelinating neuropathy. Extensive workup was pursued, including blood work, lumbar puncture, genetic testing to rule out CMT 1, and imaging of his plexus. CSF analysis revealed albuminocytological dissociation with elevated protein of 3.72 g/L. Matching oligoclonal bands were present in both CSF and serum. Genetic testing was non-contributory. Serum testing for anti-NF155 IgG and anti-contactin 1 IgG antibody via ELISA was performed by the University of Sydney Brain and Mind Center. This was positive for anti-NF155 IgG4.
The patient was trialed on several immunomodulatory therapies, summarized in the following list:

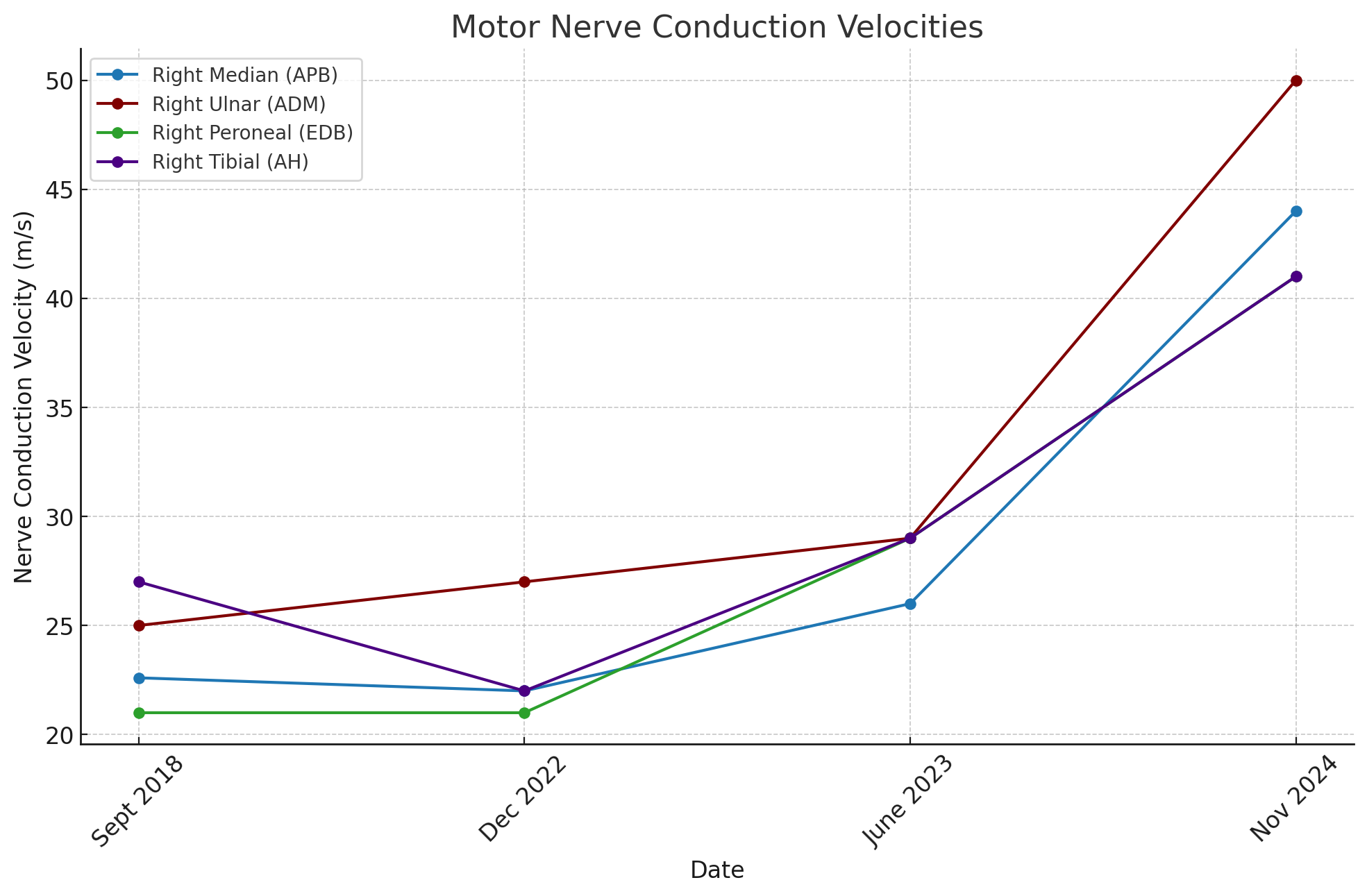
The patient did not have any improvement post IVIG/steroids and was only able to complete a brief trial of PLEX due to the COVID-19 pandemic. He started rituximab in Sept 2021, and did not have any clinical or electrophysiological benefit after more than a year of treatment. The decision was made to discontinue rituximab in Sept 2022. Repeat EMG in June 2023 did not show any change in electrophysiological findings. A brief trial of Tacrolimus was also started in Nov 2023, but discontinued due to chest and back pain.
On follow-up in Nov 2024, the patient presented with spontaneous clinical and electrophysiological recovery.
1. Van den Bergh PYK, van Doorn PA, Hadden RDM, et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint Task Force—Second revision. European Journal of Neurology. 2021;28(11):3556-3583. doi:10.1111/ene.14959
2. Mathey EK, Park SB, Hughes RAC, et al. Chronic inflammatory demyelinating polyradiculoneuropathy: from pathology to phenotype. J Neurol Neurosurg Psychiatry. 2015;86(9):973-985. doi:10.1136/jnnp-2014-309697
3. Devaux JJ, Miura Y, Fukami Y, et al. Neurofascin-155 IgG4 in chronic inflammatory demyelinating polyneuropathy. Neurology. 2016;86(9):800-807. doi:10.1212/WNL.0000000000002418
4. Kira J ichi. Anti-Neurofascin 155 Antibody-Positive Chronic Inflammatory Demyelinating Polyneuropathy/Combined Central and Peripheral Demyelination: Strategies for Diagnosis and Treatment Based on the Disease Mechanism. Front Neurol. 2021;12:665136. doi:10.3389/fneur.2021.665136
5. Shelly S, Klein CJ, Dyck PJB, et al. Neurofascin-155 Immunoglobulin Subtypes: Clinicopathologic Associations and Neurologic Outcomes. Neurology. 2021;97(24):e2392-e2403. doi:10.1212/WNL.0000000000012932
6. Benedetti L, Briani C, Franciotta D, et al. Rituximab in patients with chronic inflammatory demyelinating polyradiculoneuropathy: a report of 13 cases and review of the literature. J Neurol Neurosurg Psychiatry. 2011;82(3):306-308. doi:10.1136/jnnp.2009.188912
7. Roux T, Debs R, Maisonobe T, et al. Rituximab in chronic inflammatory demyelinating polyradiculoneuropathy with associated diseases. J Peripher Nerv Syst. 2018;23(4):235-240. doi:10.1111/jns.12287
8. Doneddu PE, Cocito D, Fazio R, et al. Prospective open-label trial with rituximab in patients with chronic inflammatory demyelinating polyradiculoneuropathy not responding to conventional immune therapies. J Neurol Neurosurg Psychiatry. 2024;95(9):838-844. doi:10.1136/jnnp-2023-332844

Objectives: to evaluate the clinical features, findings of EEG and brain imaging in psychiatric patients with epilepsy in Razi Psychiatric Hospital
Methods: This retrospective descriptive-analytical study was performed on epileptic patients with psychiatric disorders in Razi Psychiatric Hospital affiliated to University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
Results: Out of 94 epileptic patients, 9.6% had focal epilepsy, 26.6% had diffuse epilepsy, 36.1% had focal-diffuse epilepsy and 26.8% had unknown epilepsy. About 12% had a structural etiology and 88% had an unknown etiology
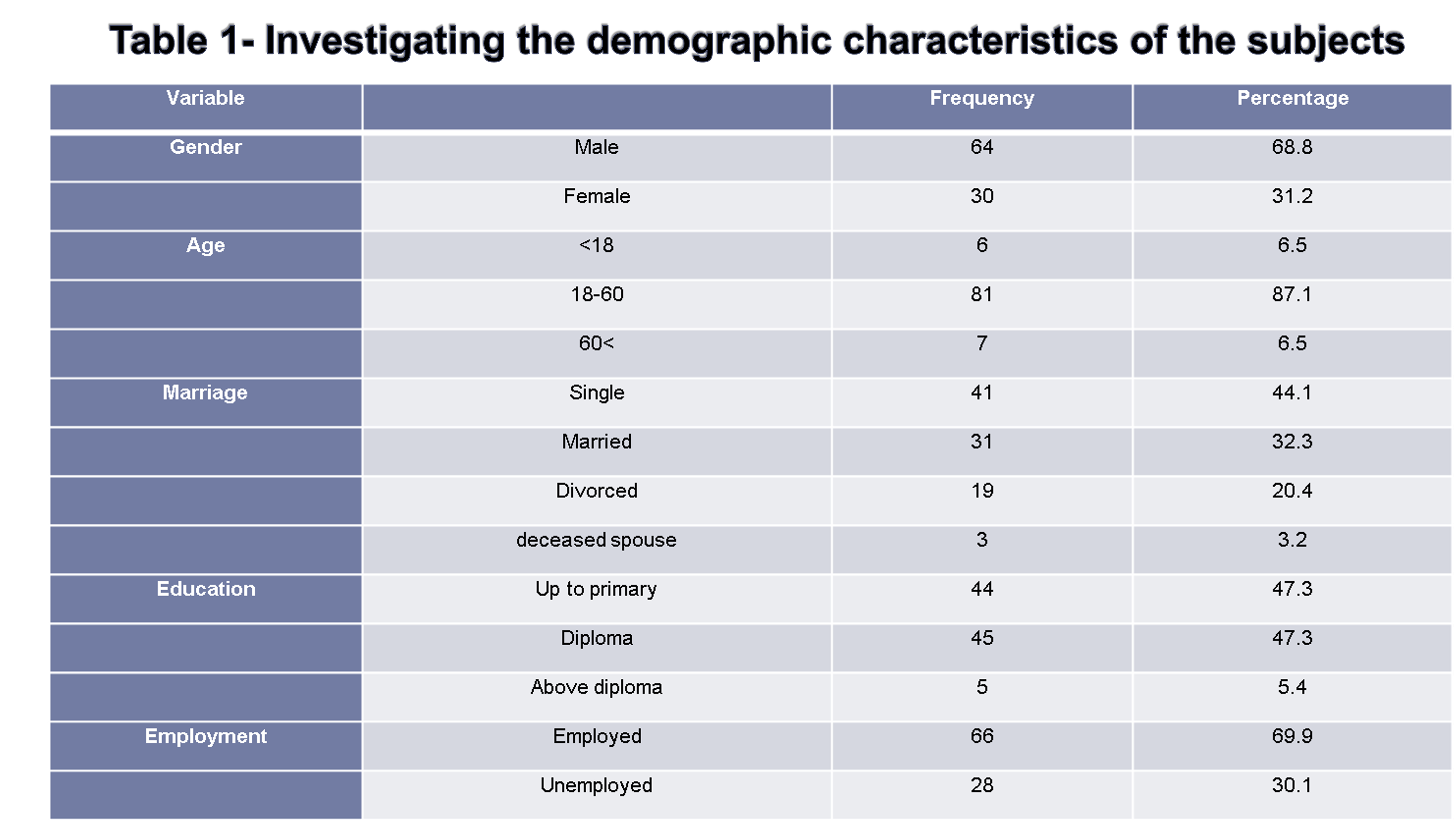
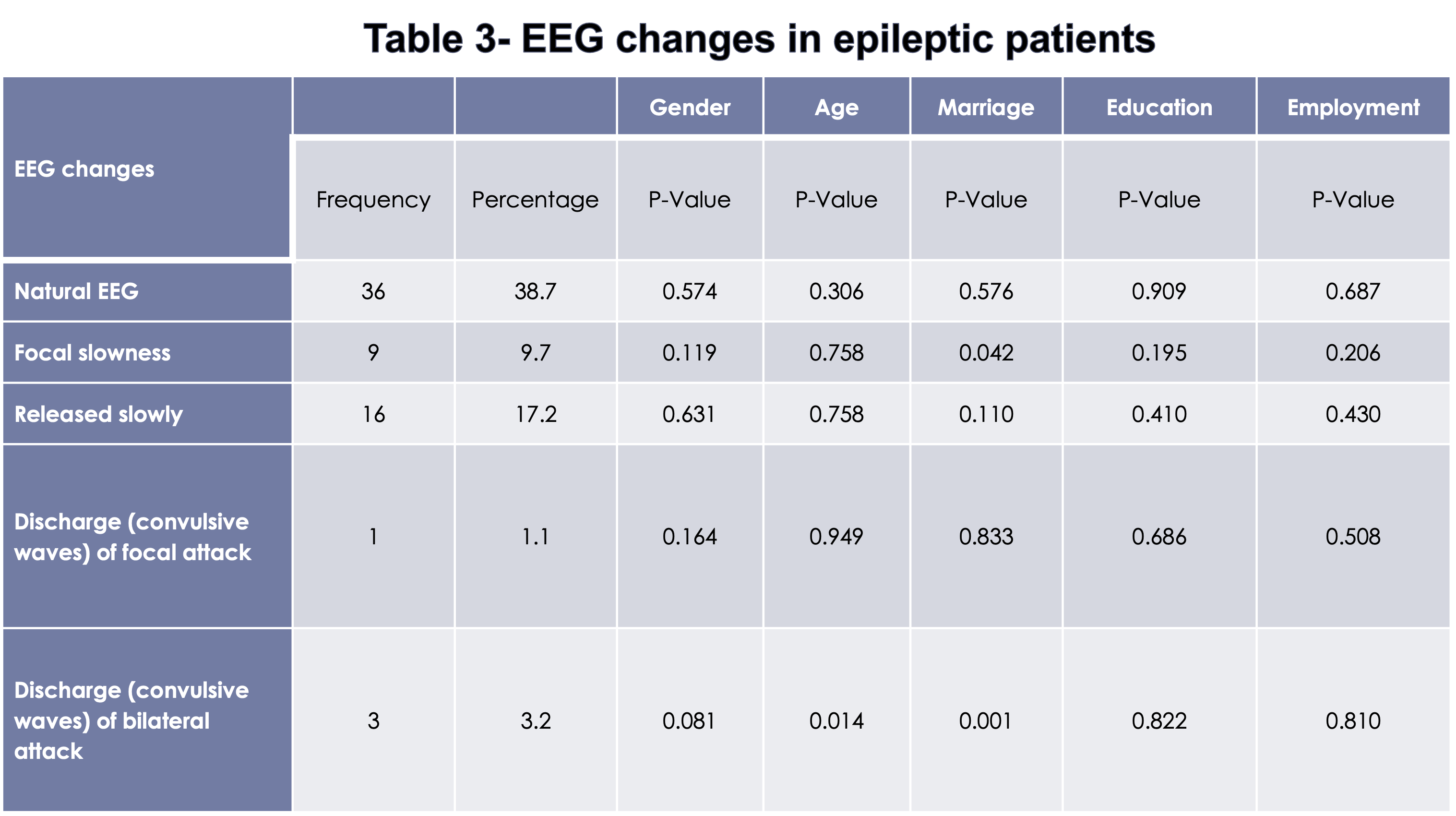
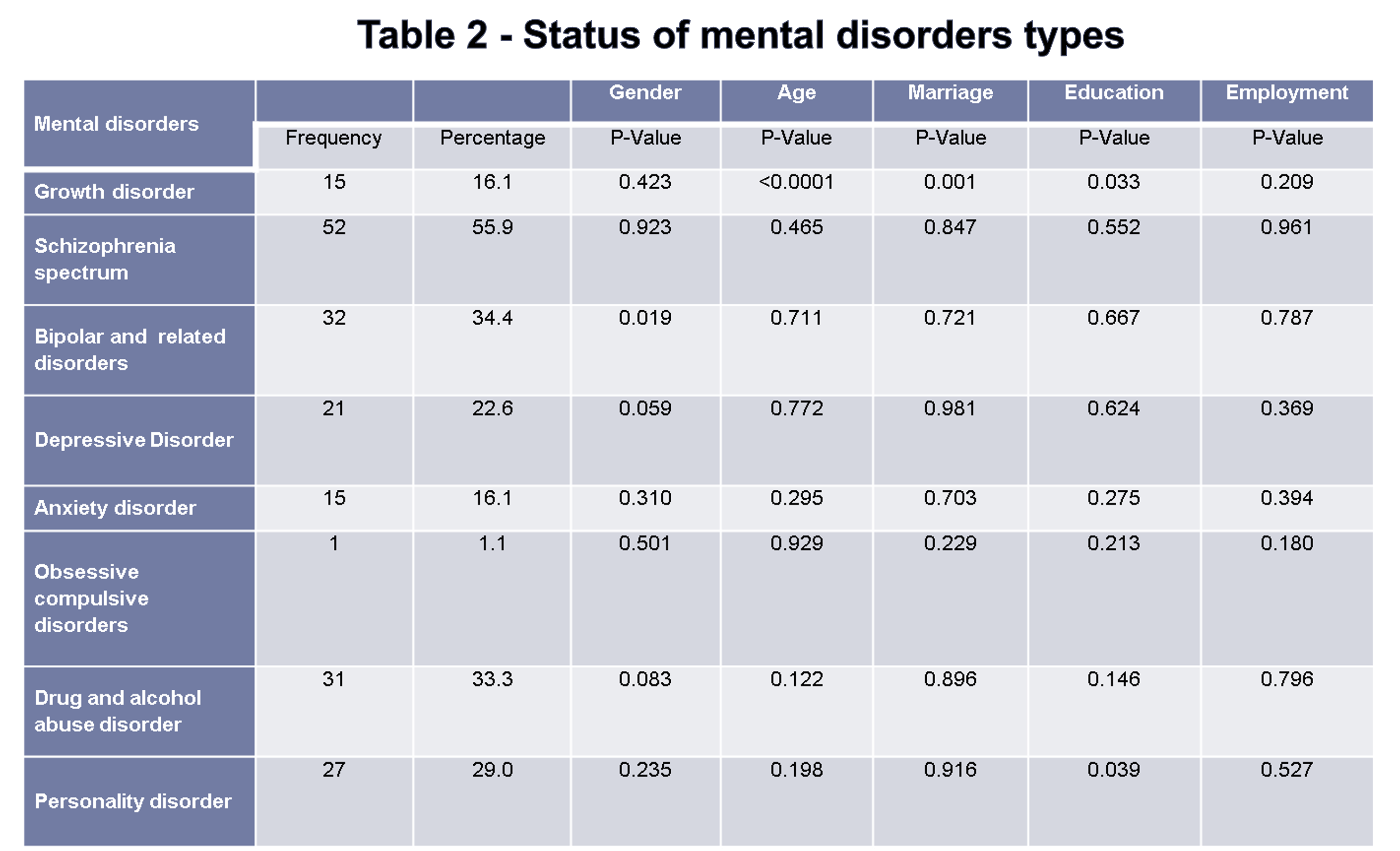
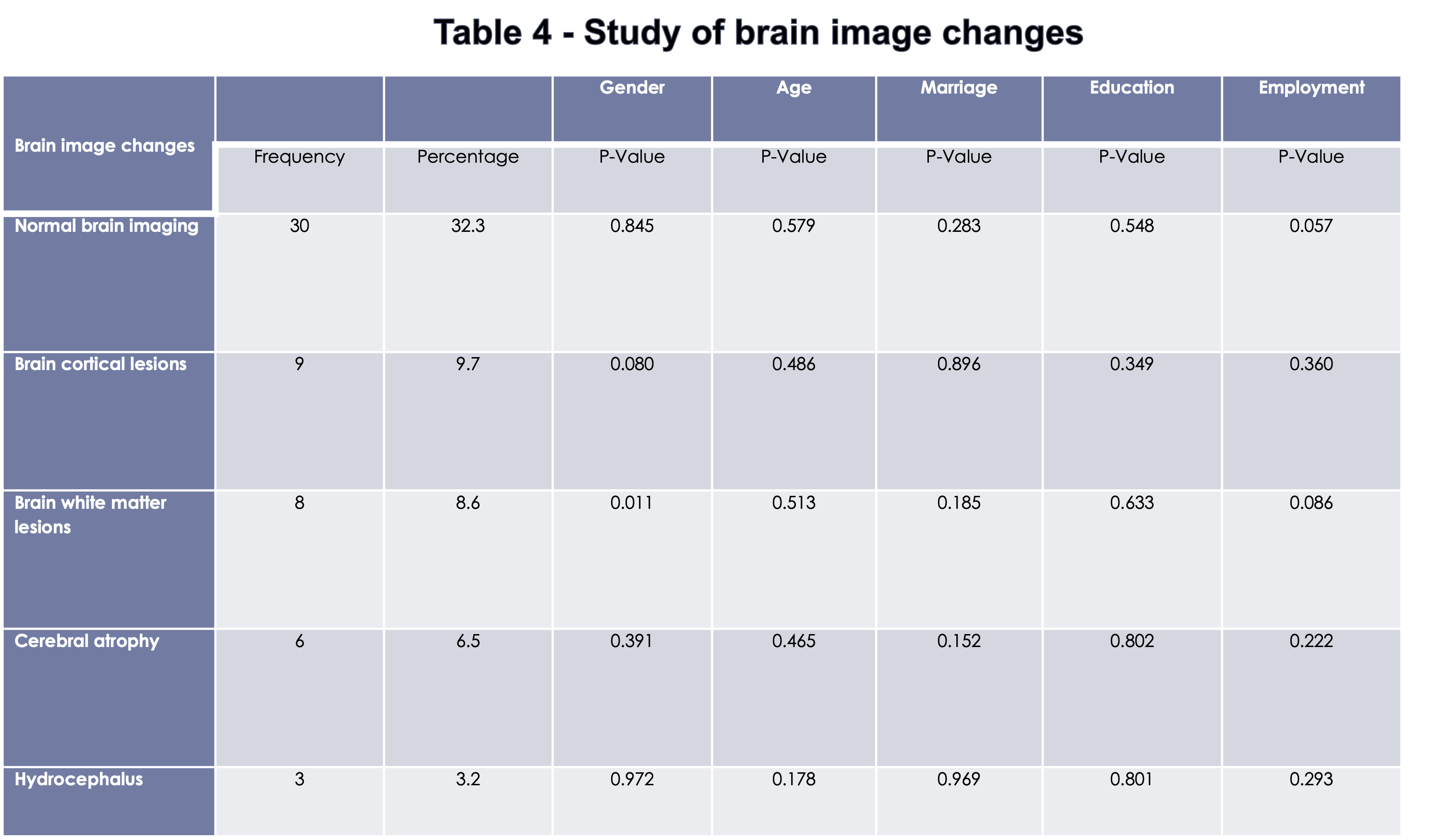
Conclusion:
and causes psychiatric disorders in them.

Background
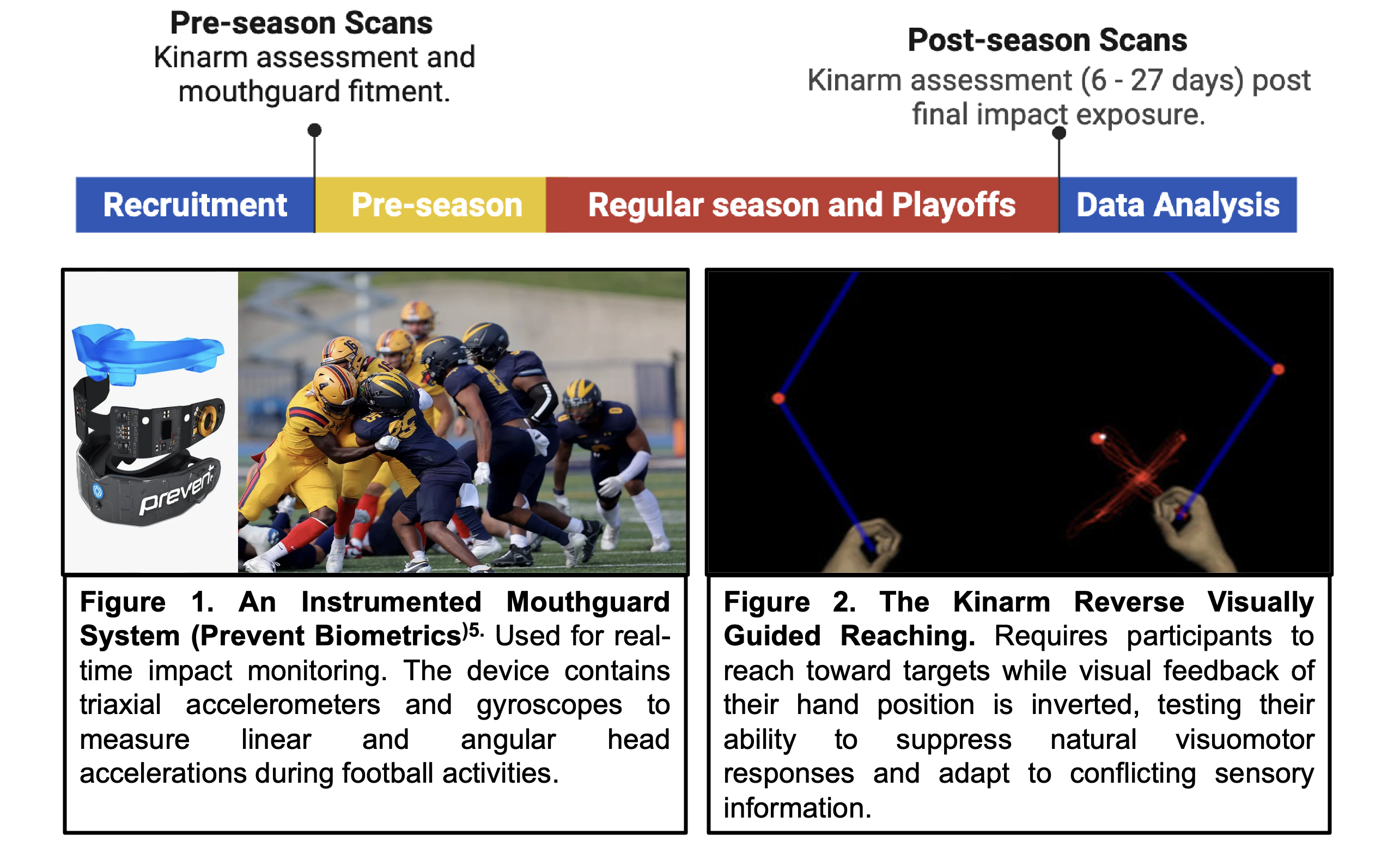
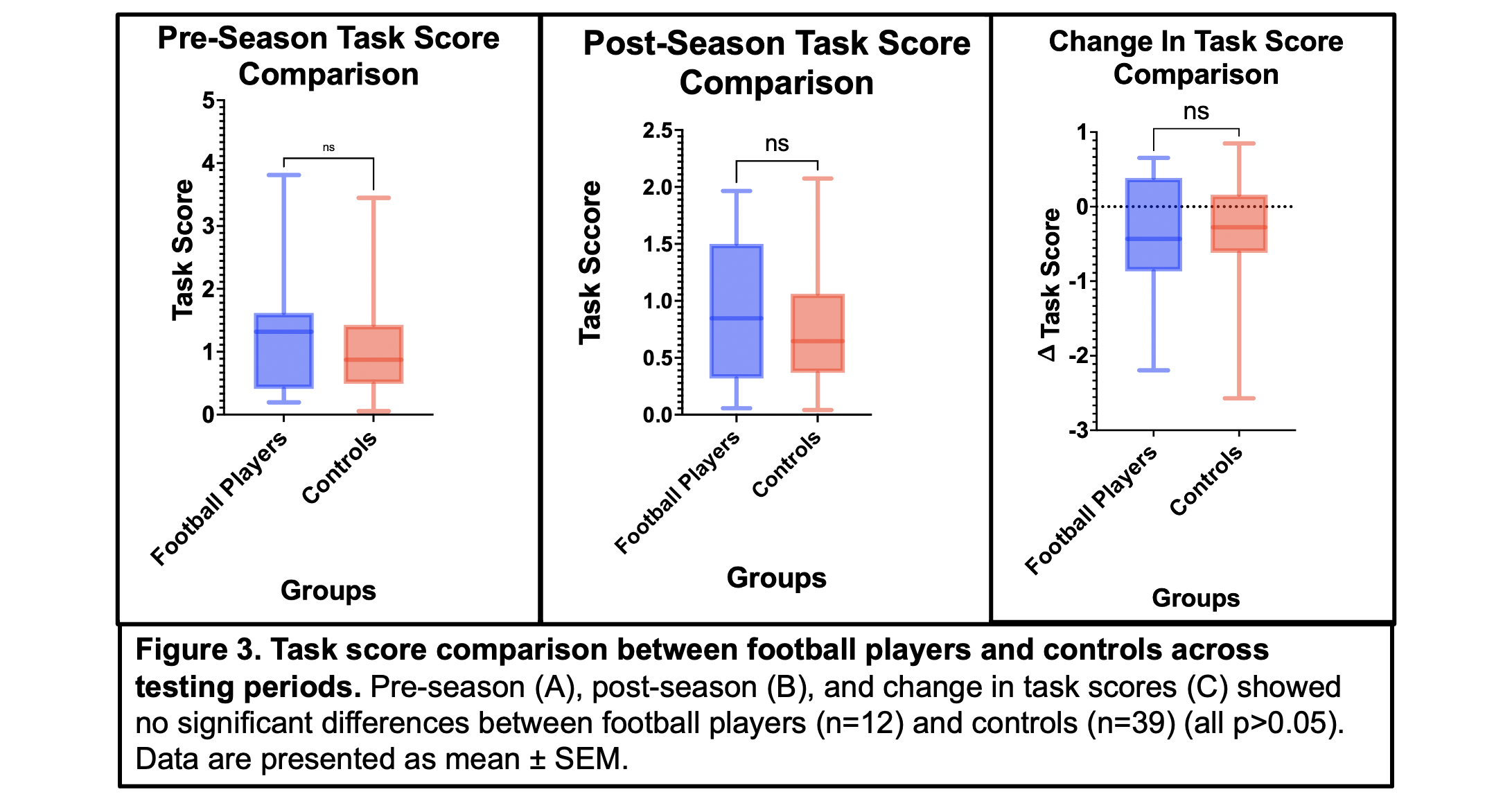
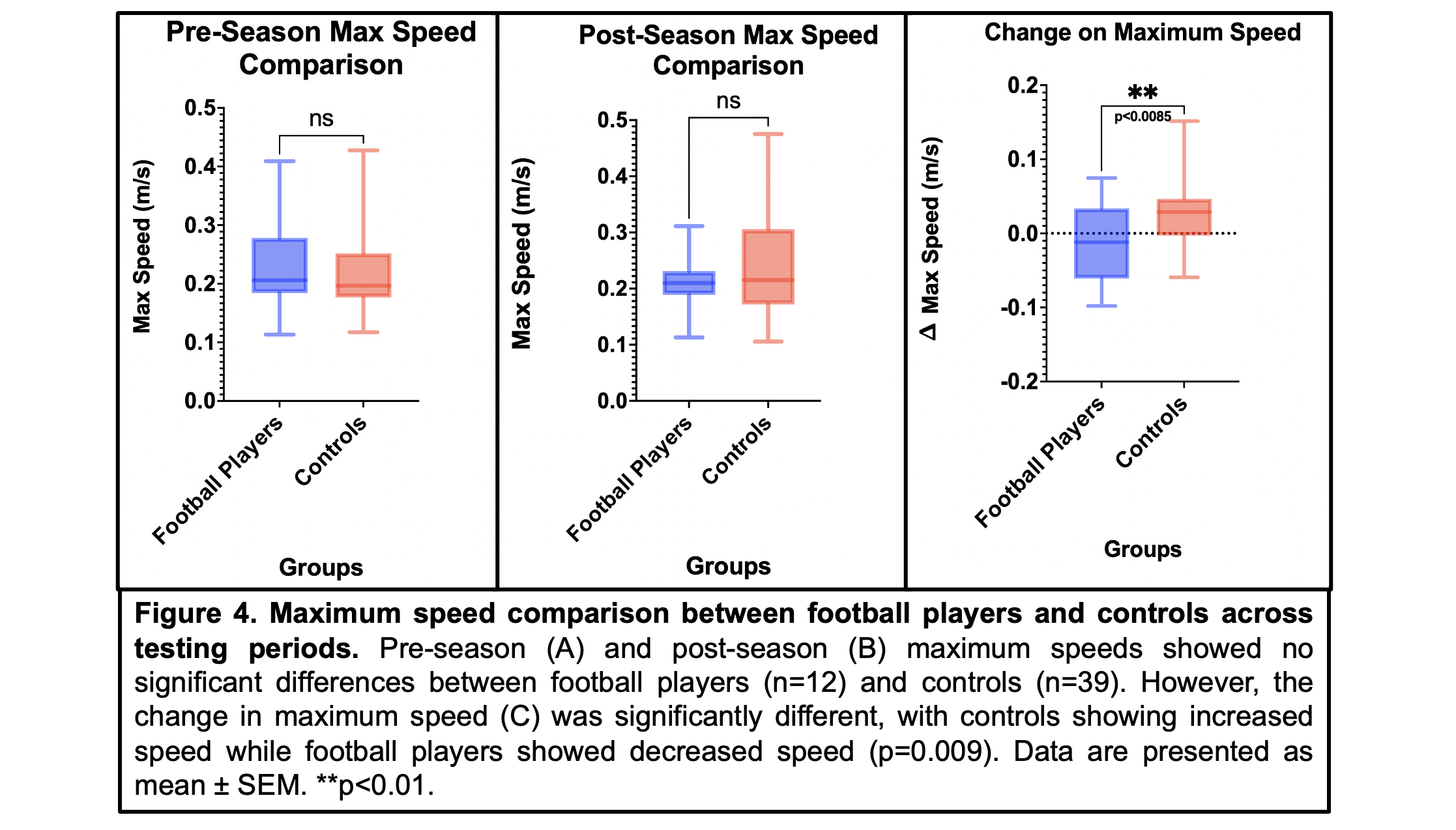
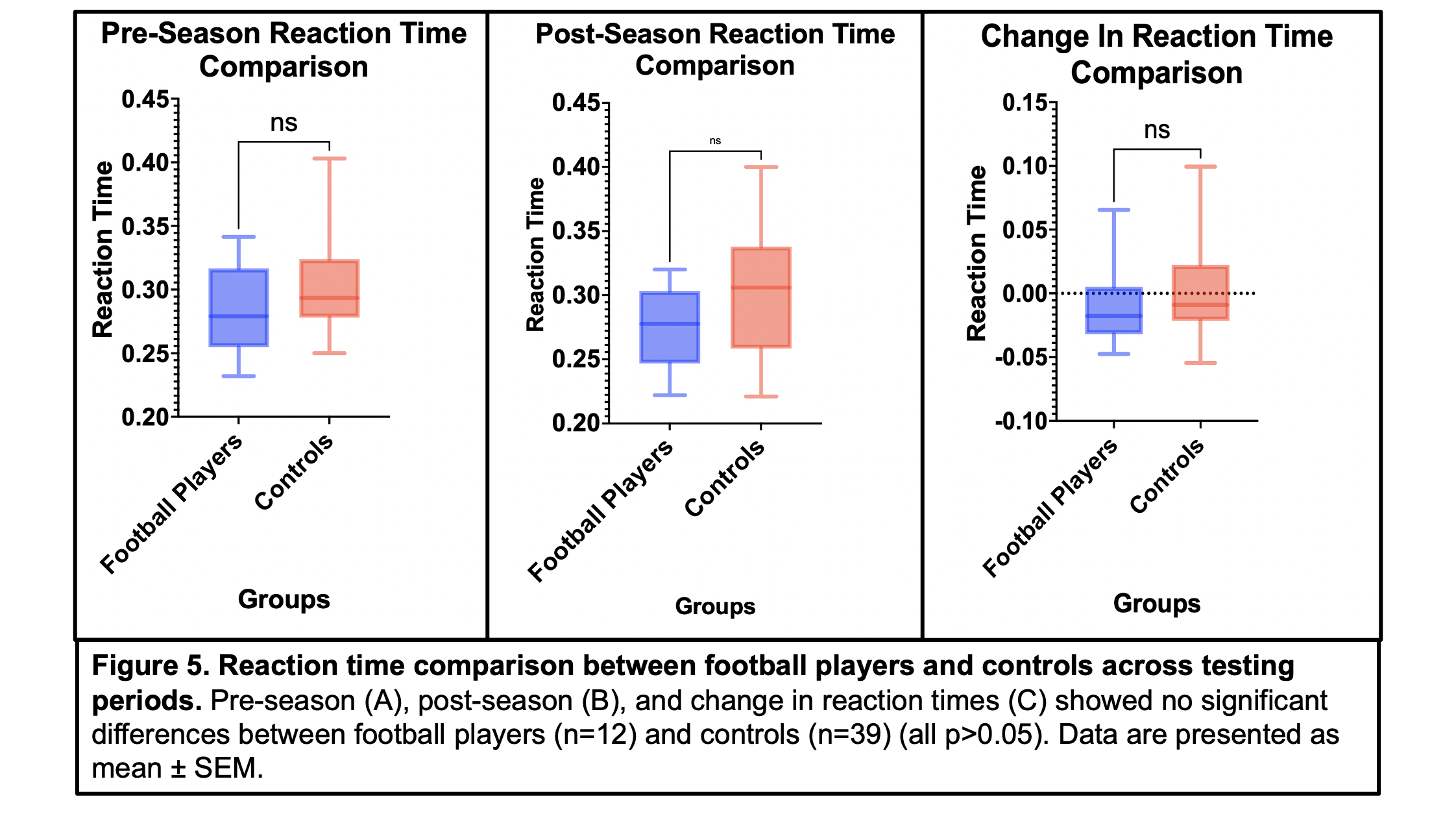
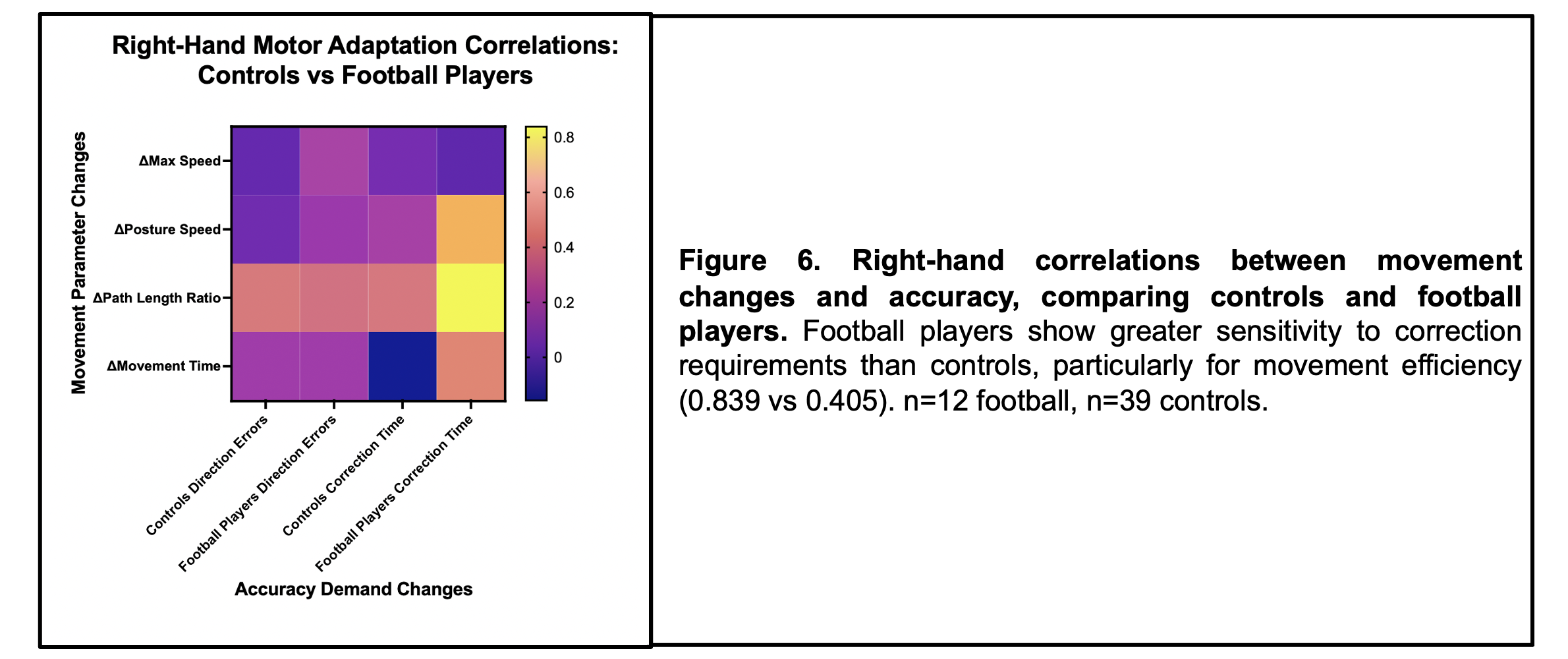

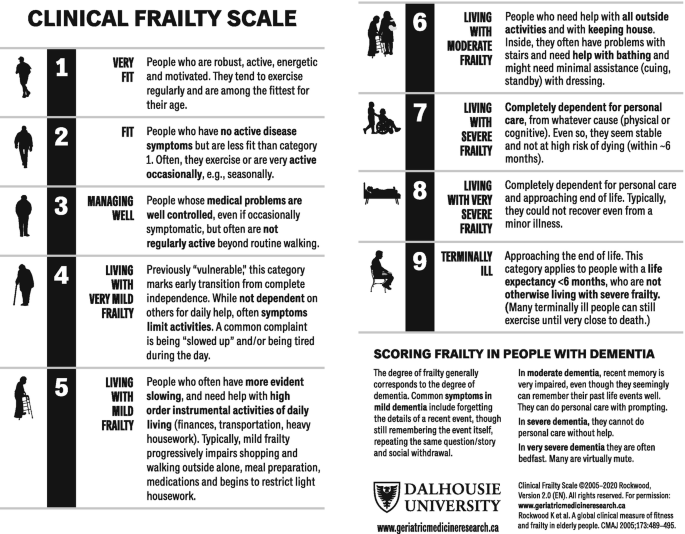
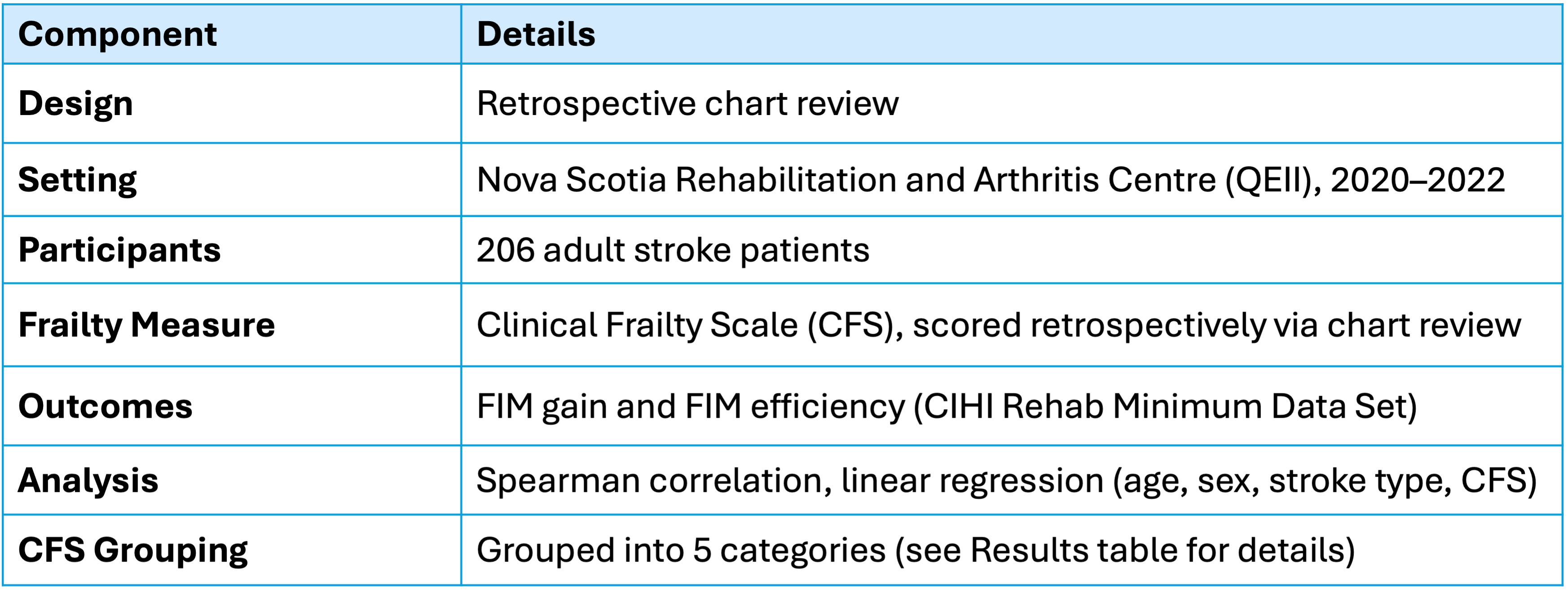
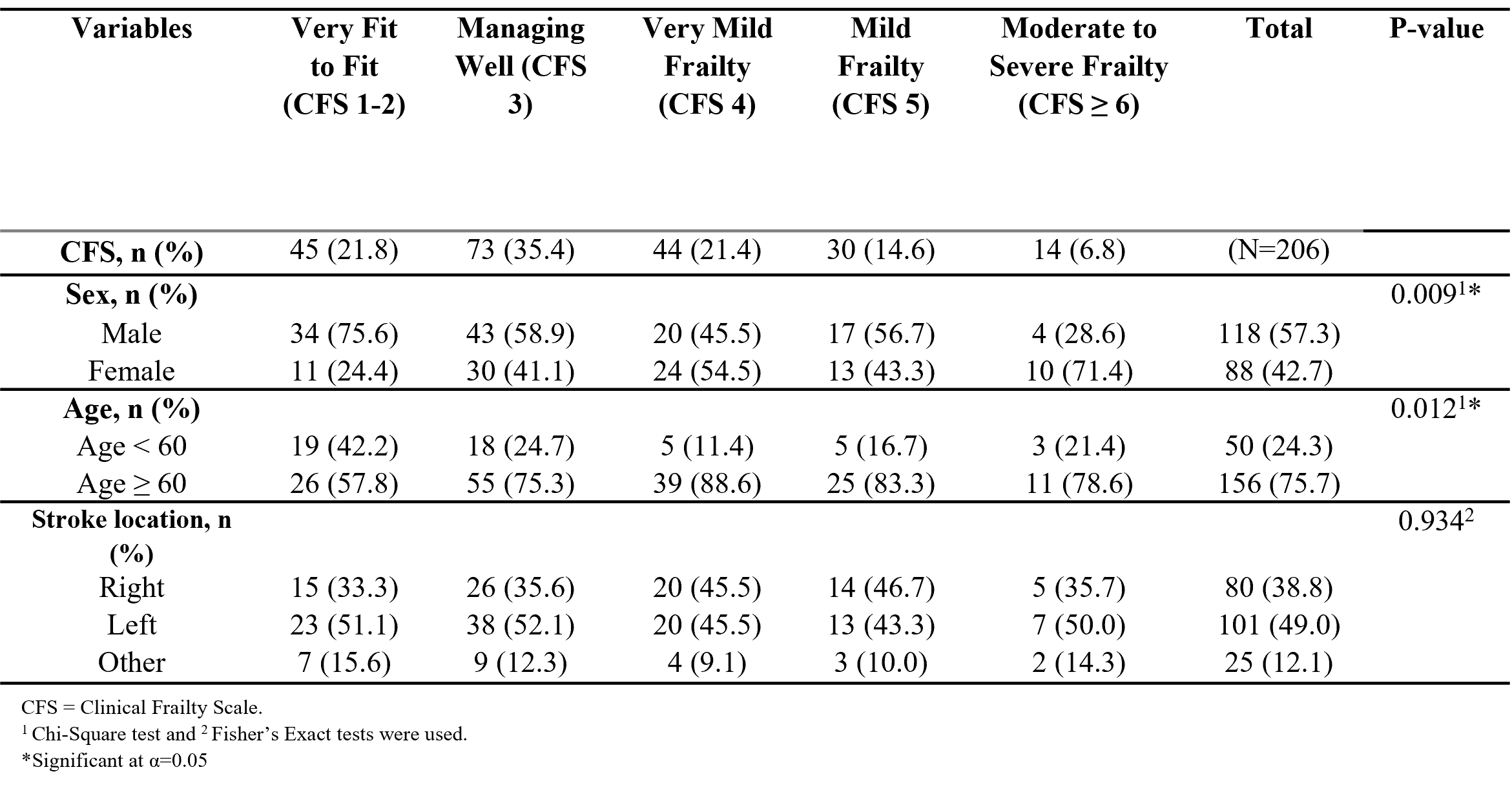
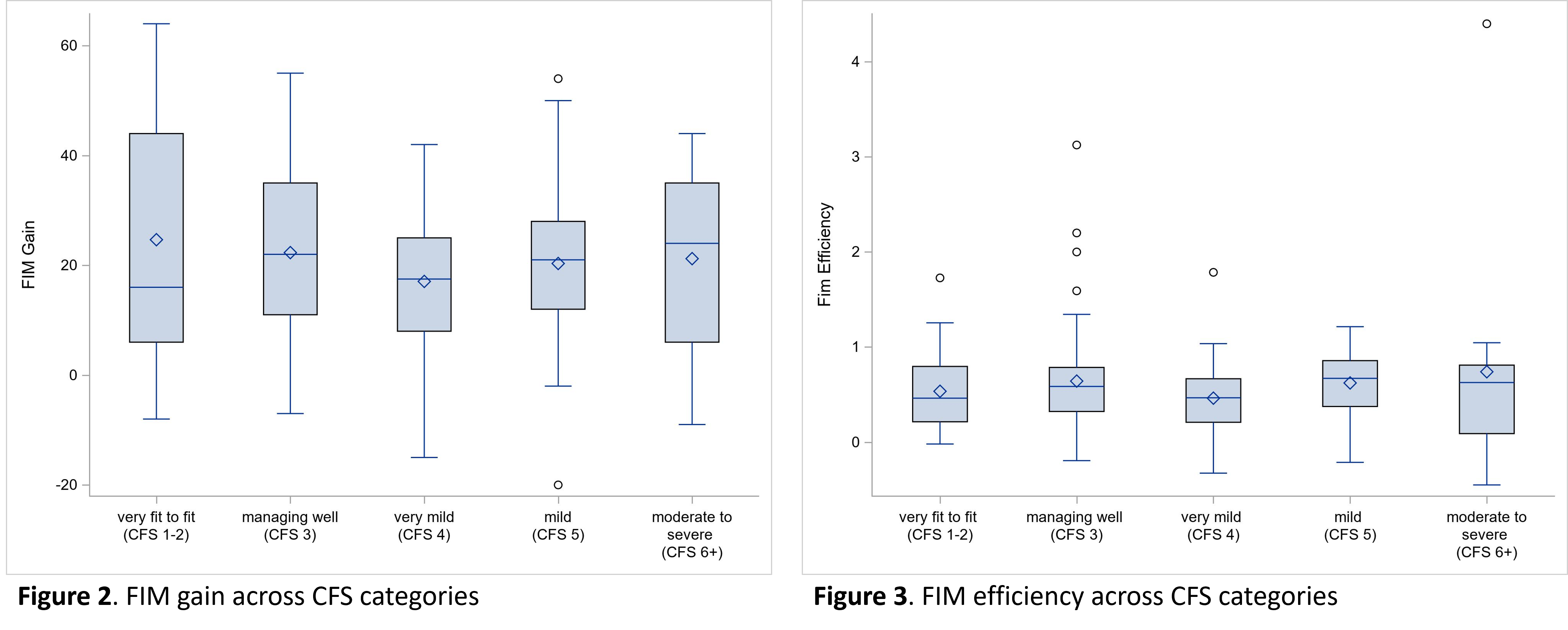
Stroke is the second leading cause of disability worldwide, yet effective therapies remain limited. Currently, alteplase is the only approved treatment for hyperacute ischemic stroke, but its use is constrained by a short therapeutic window, prompting ongoing efforts to develop safer and more effective options. Gene therapy offers a novel approach for repairing tissue damage—particularly NeuroD1-mediated astrocyte-to-neuron conversion, which regenerates functional neurons after ischemic injury. In this study, we administrated NeuroD1 therapy in a non-human primate (NHP) stroke model to evaluate its effects on corticospinal tract (CST) recovery and motor performance.
Eight non-human primates (NHPs) underwent middle cerebral artery occlusion (MCAO). Fourteen days post-MCAO, six animals received intracranial NeuroD1 treatment (n = 3 high dose; n = 3 low dose), while two animals received a control solution. Neurological and functional performance were assessed daily using the Non-Human Primate Stroke Scale (NHPSS) and the primate Rankin Scale (pRS), respectively.
MRI scans—including DTI, FLAIR, T1-weighted (T1w), and T2-weighted (T2w) sequences—were acquired at baseline and at 7, 30, 90, 120, and 240 days post-MCAO. Stroke lesions were manually segmented using T1w, FLAIR, and T2w images. Bilateral corticospinal tracts (CST) were reconstructed at each time point. Group comparisons of behavioral performance and fractional anisotropy (FA) along each CST were conducted to evaluate motor recovery and white matter integrity, respectively.
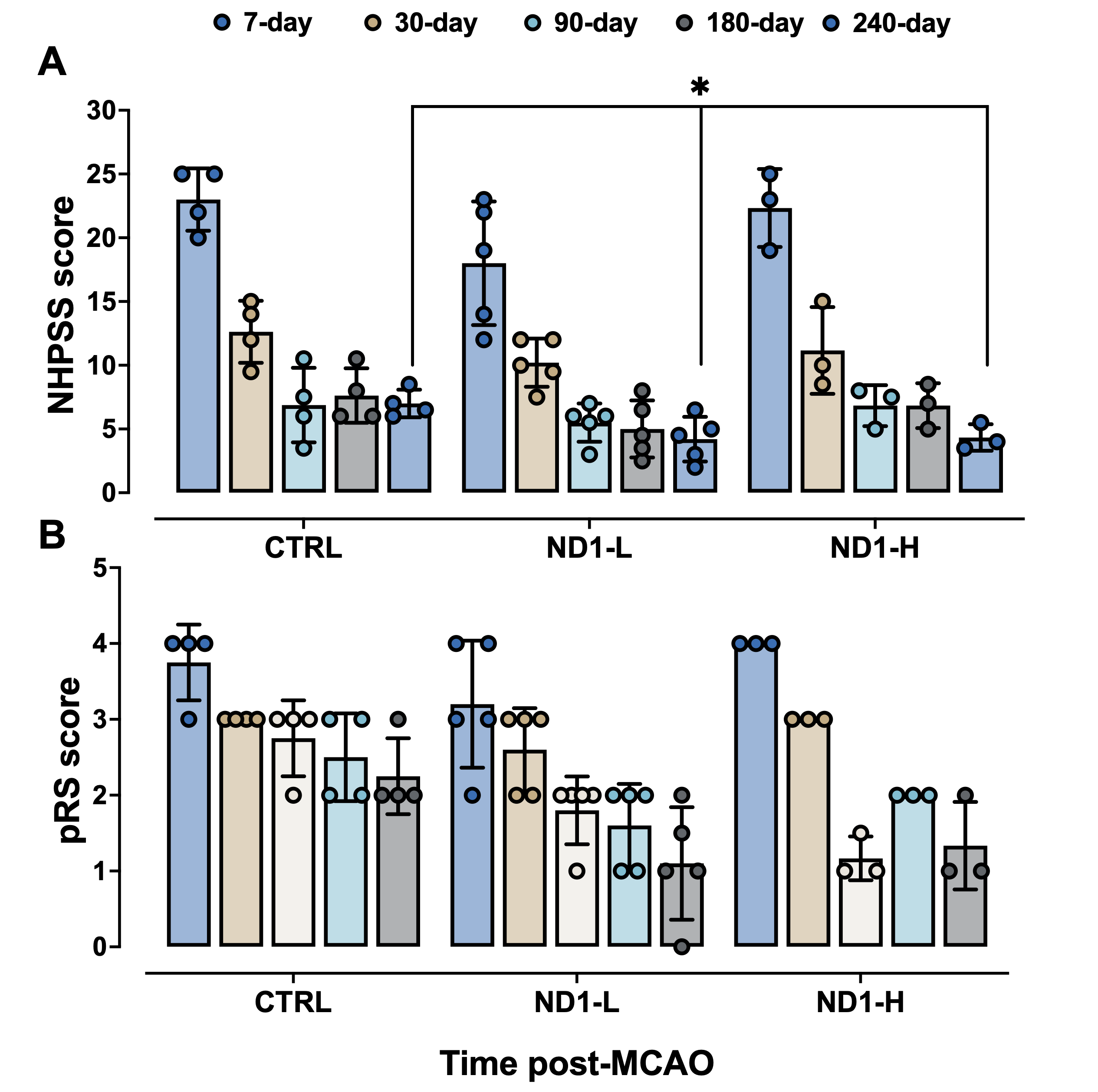
Neurological performance improvements were most evident on the NHPSS scale. NHPs receiving the control solution exhibited poor motor recovery and minimal or no CST reconstruction. In contrast, animals treated with a low dose of NeuroD1 showed both motor and functional recovery, accompanied by evidence of CST reconstruction. Notably, the group receiving the high dose of NeuroD1 demonstrated the most substantial behavioral improvements, along with greater CST integrity. Importantly, no significant differences in lesion size were observed between the control group and either of the NeuroD1-treated groups.
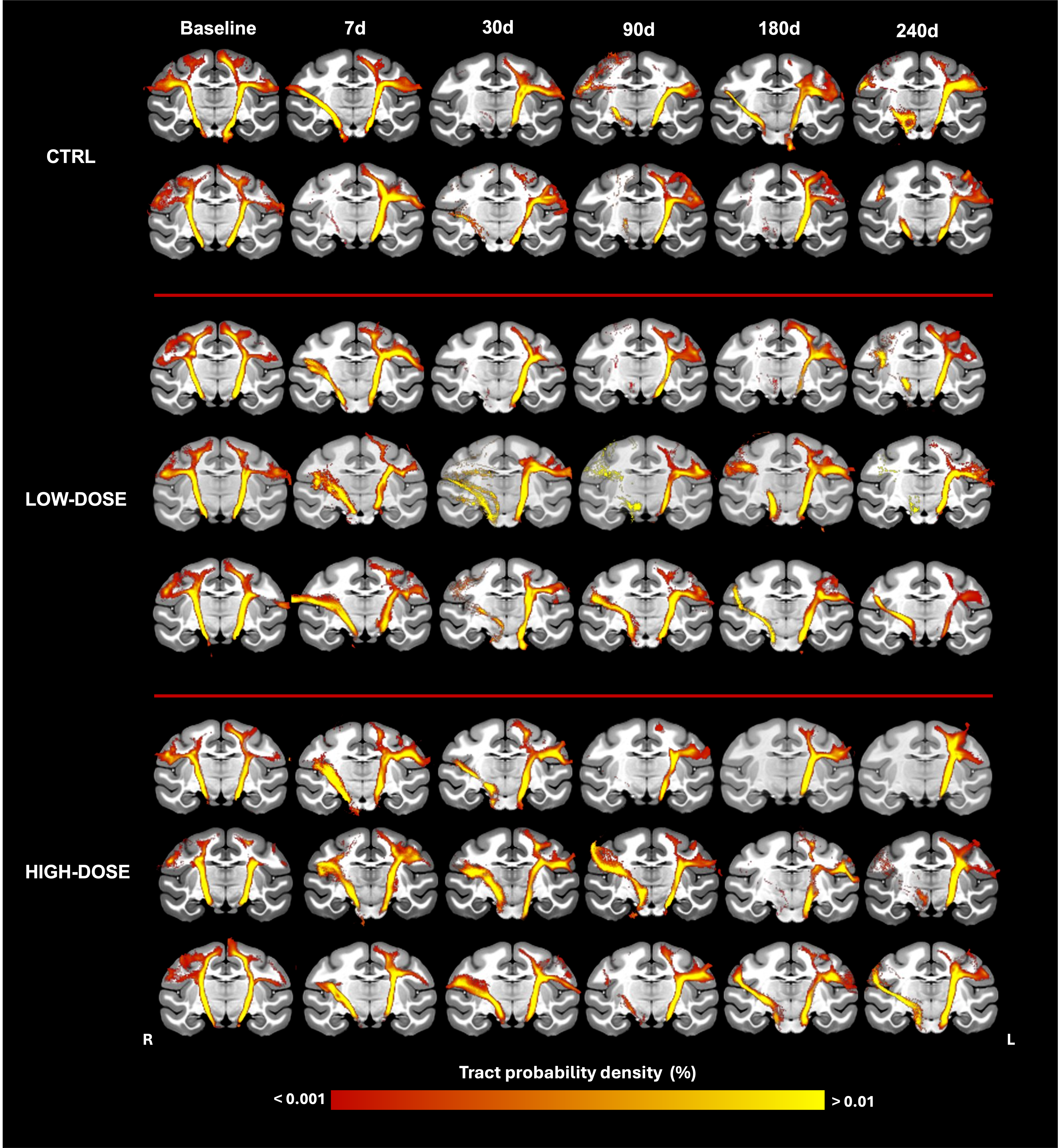
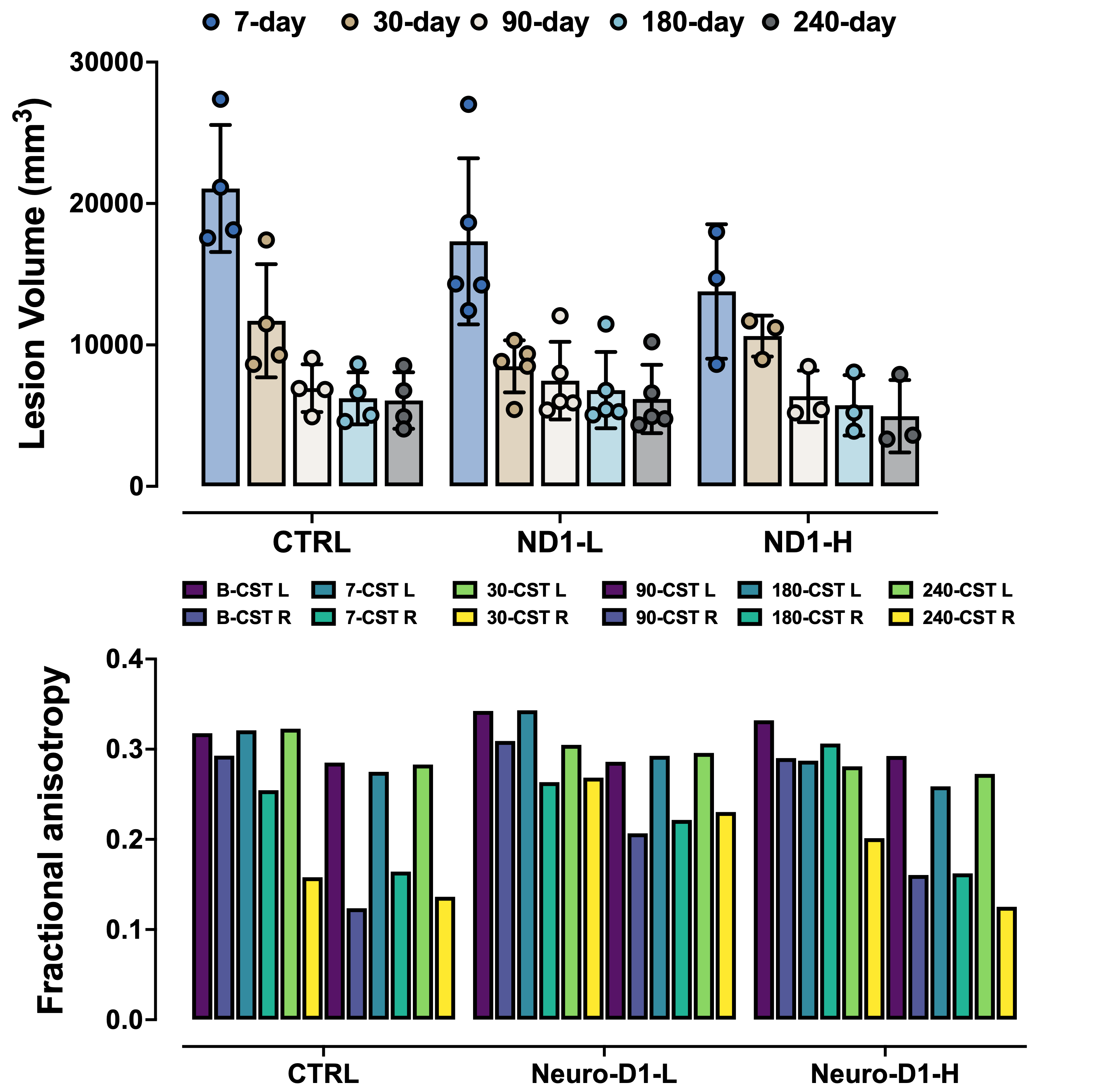
NeuroD1 treatment promotes white matter tract restoration and facilitates motor recovery following stroke.

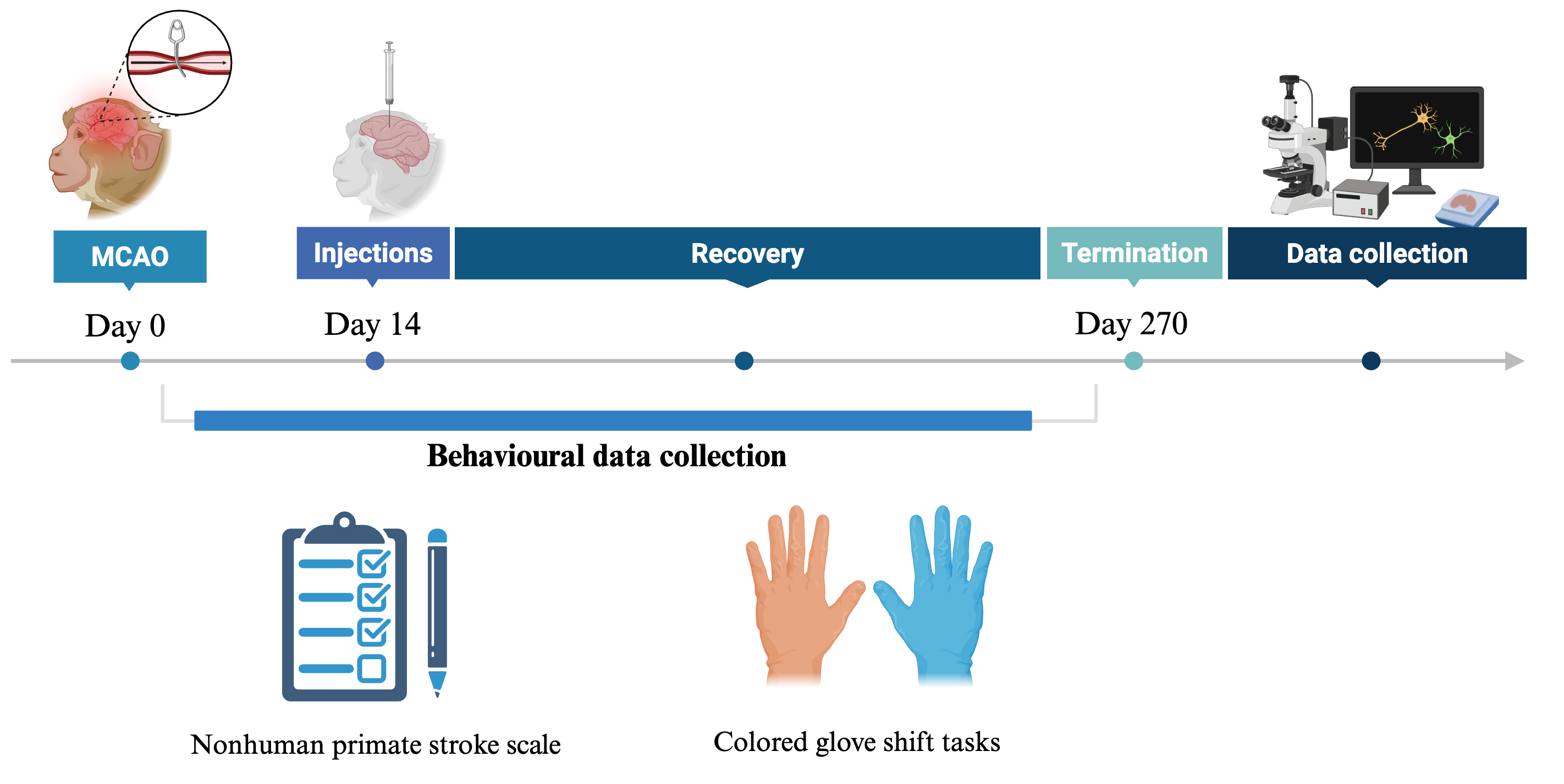
Method
In this study, twelve NHPs at 14 days post middle cerebral artery occlusion surgery received NeuroD1-AVV intracerebrally. NHP stroke scale (NHPSS) and colored glove shift tasks were performed during the recovery period of nine months. Tissues were harvested and stained for neuronal (NEUN and MAP2) and astrocyte (GFAP) markers. Dendritic complexity was evaluated using Neurolucida 360, and cell counts were performed with FIJI. All statistical analyses were conducted using Prism 9 software.
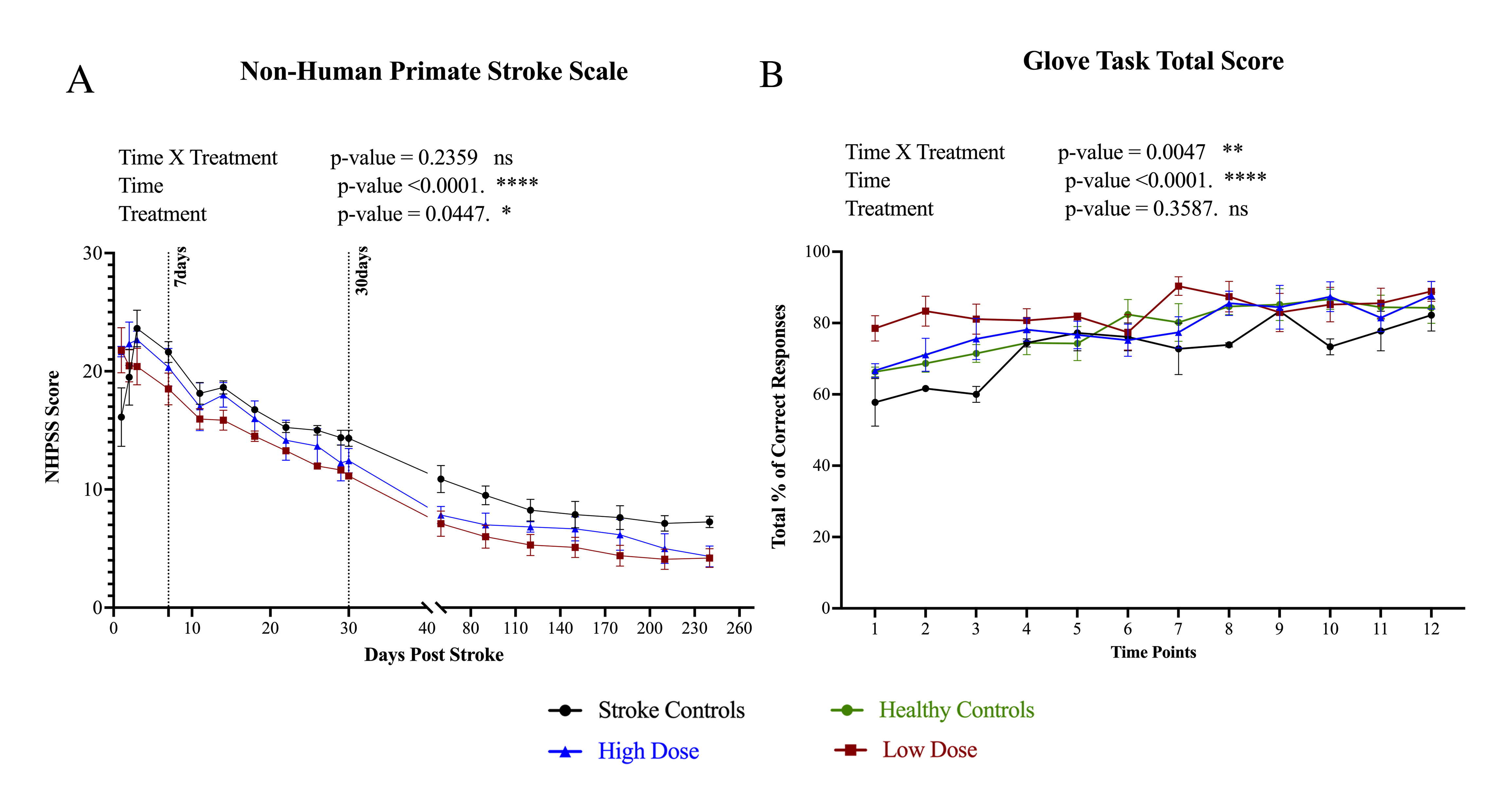
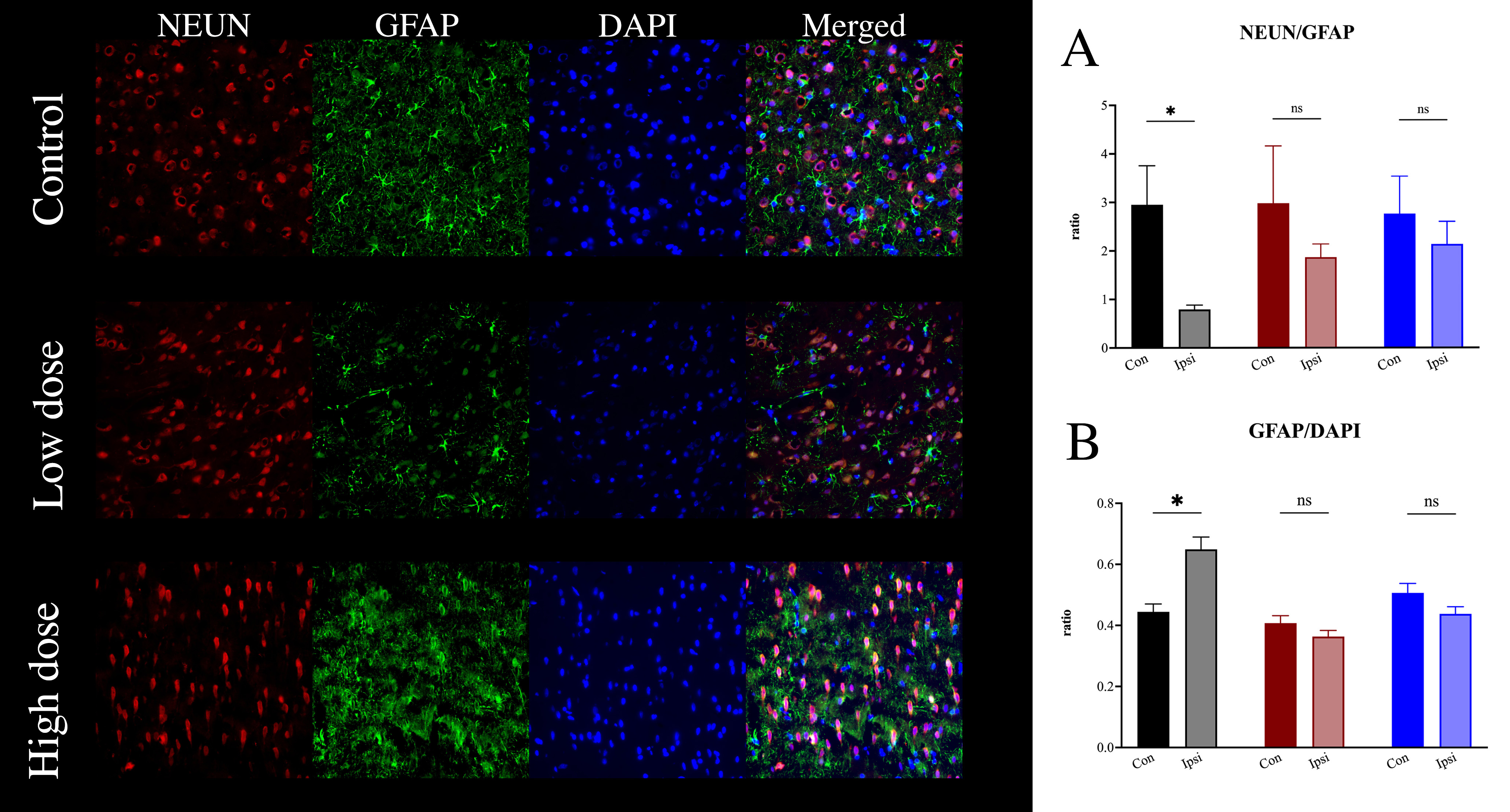
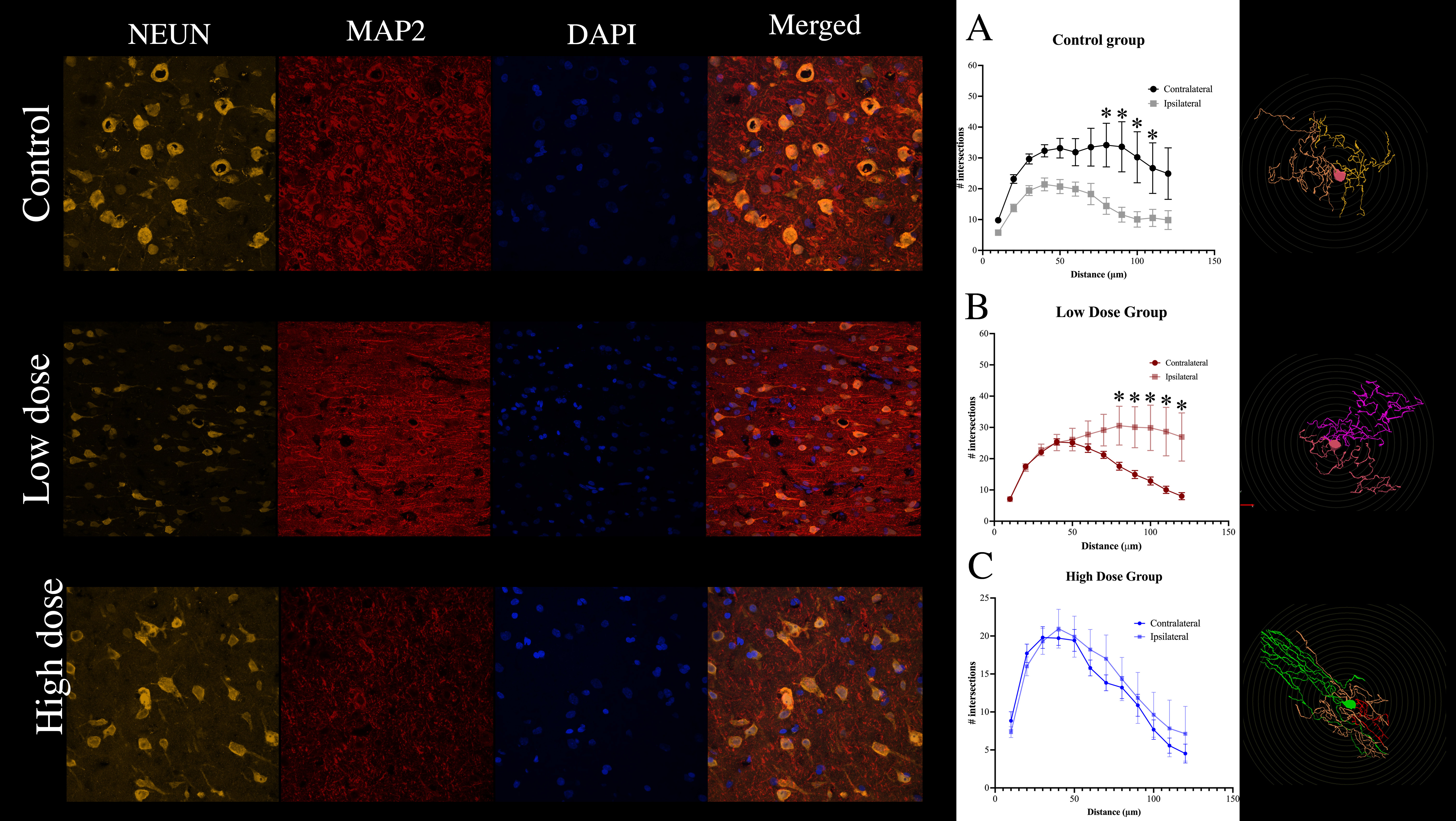
Although all groups are shown to improve in behavioural assessments through the recovery process, treatment groups exert a notable effect. Analysis reveals that both treatment dosages are successfully restoring neuronal and glial cell ratios; the impact on cellular morphology and dendritic complexity varies with dosage. Further investigations are needed to confirm the overall morphological and connective properties of transdifferentiated neurons.
Acknowledgment
We would like to sincerely thank Dr. Andrew Winterborn, Dr. Alana Backx, Dana Mika, ACS techs and staff for their immense contributions to animal health and welfare. Additionally, we acknowledge Neleah Lavoie for her outstanding work in the lab. Your dedication and efforts are greatly appreciated.
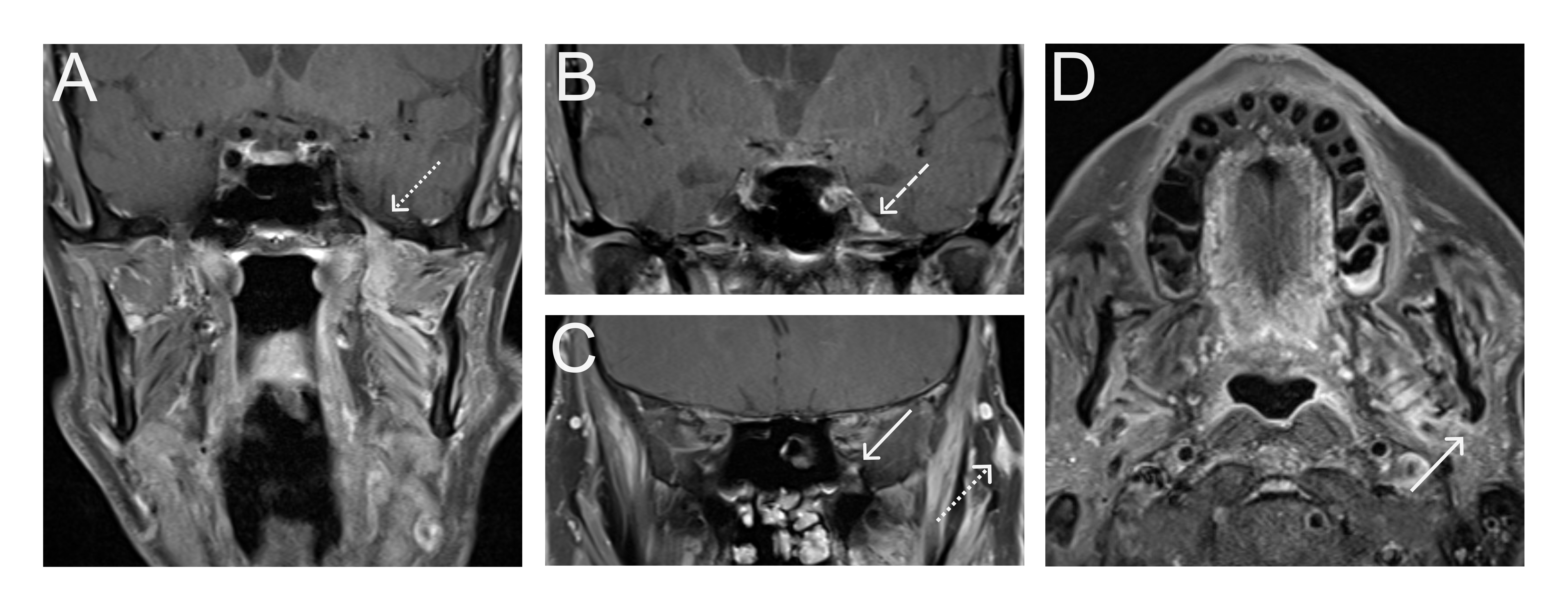
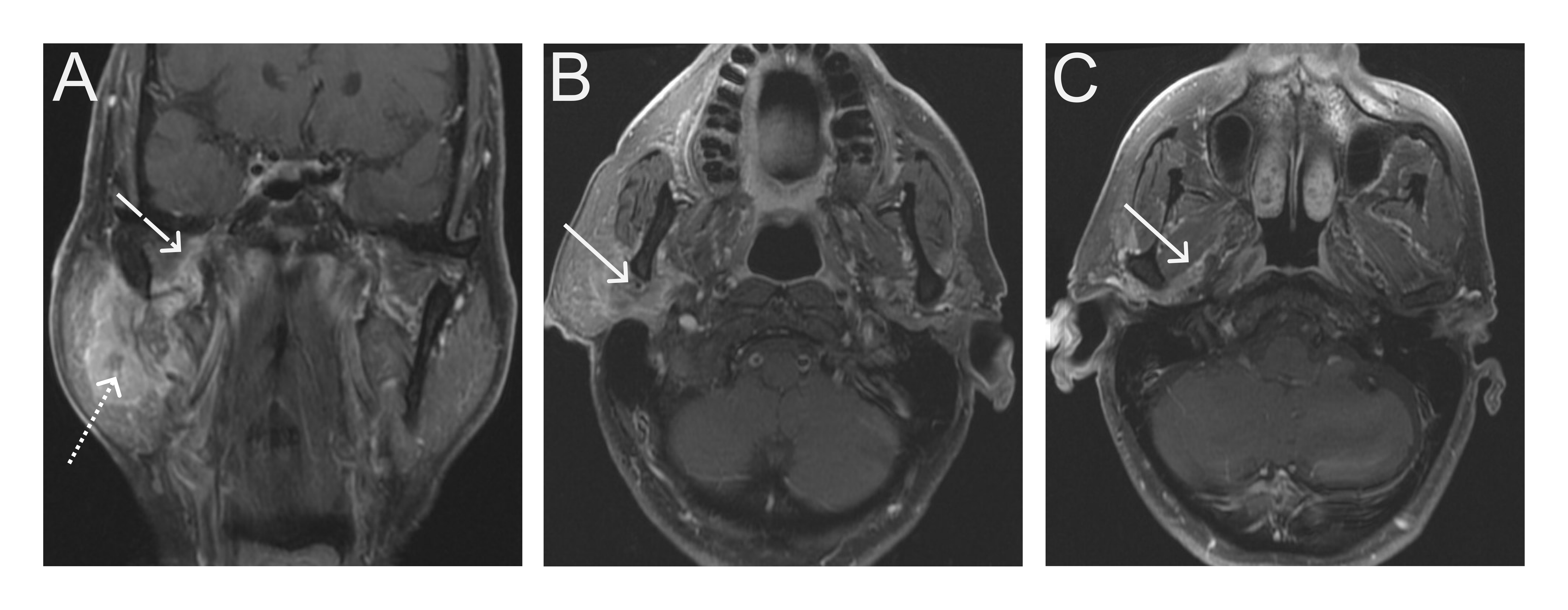
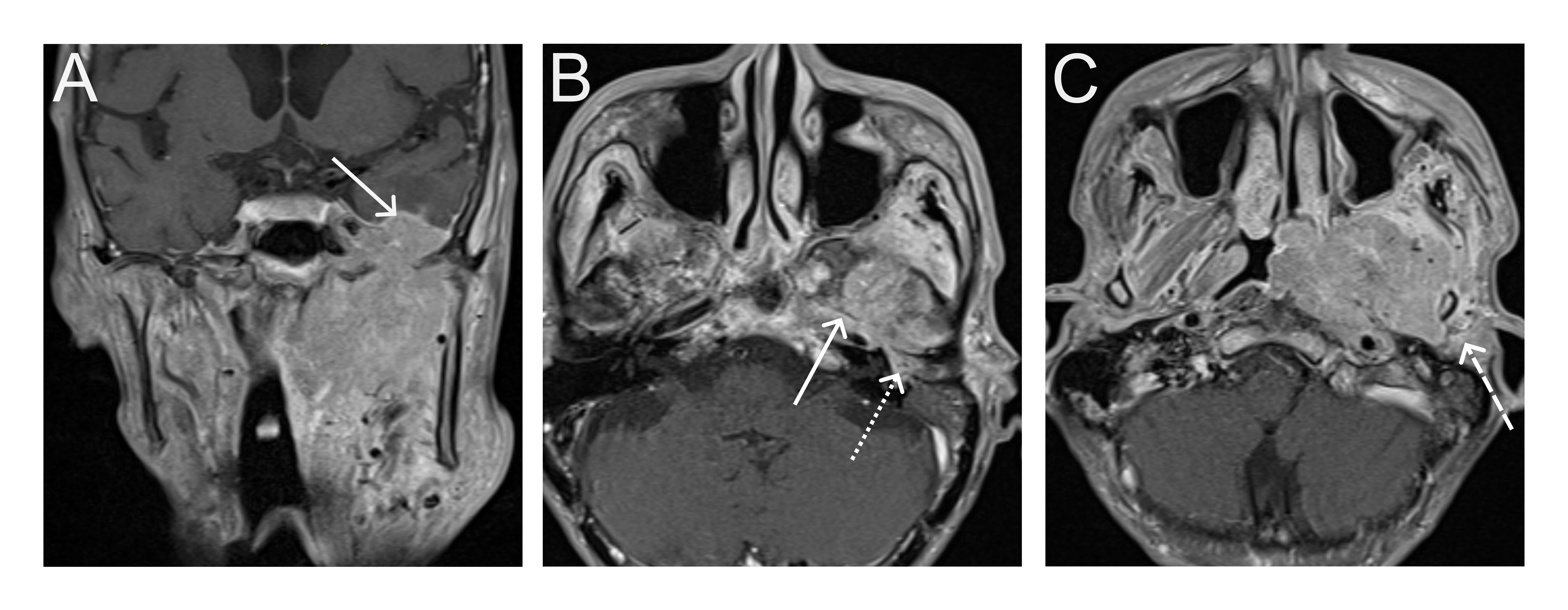
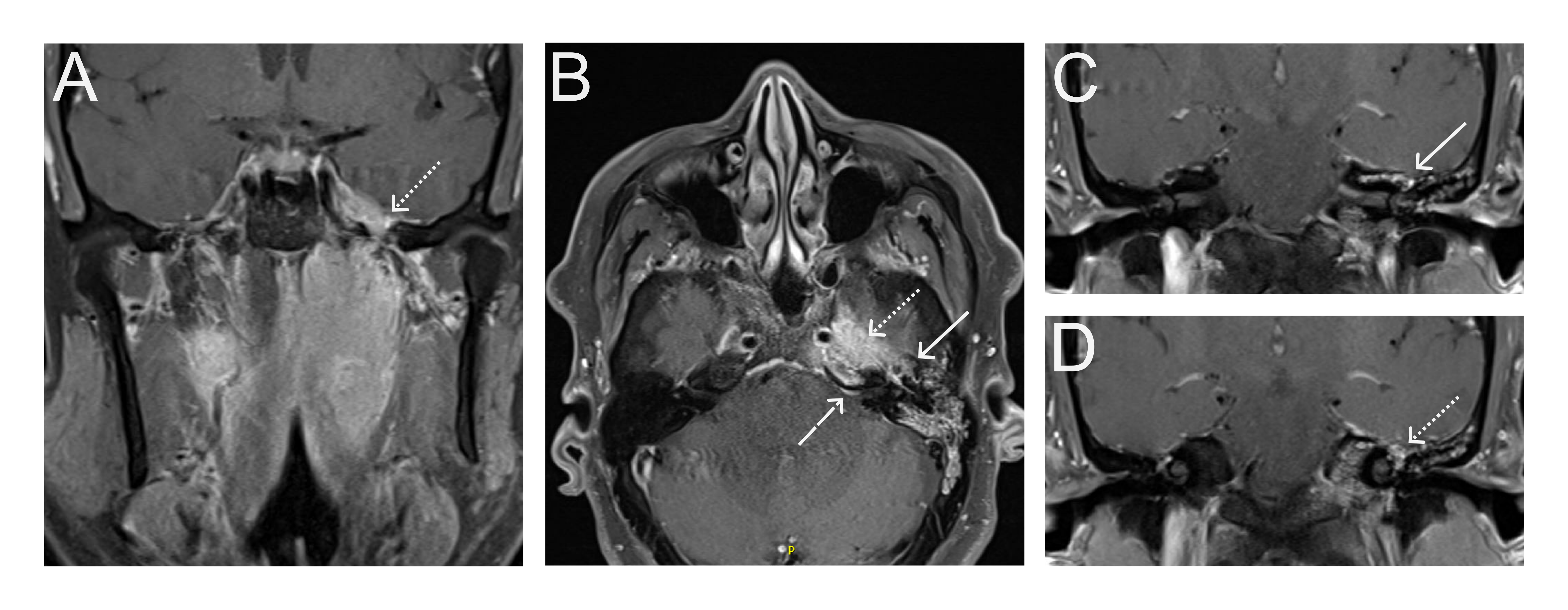
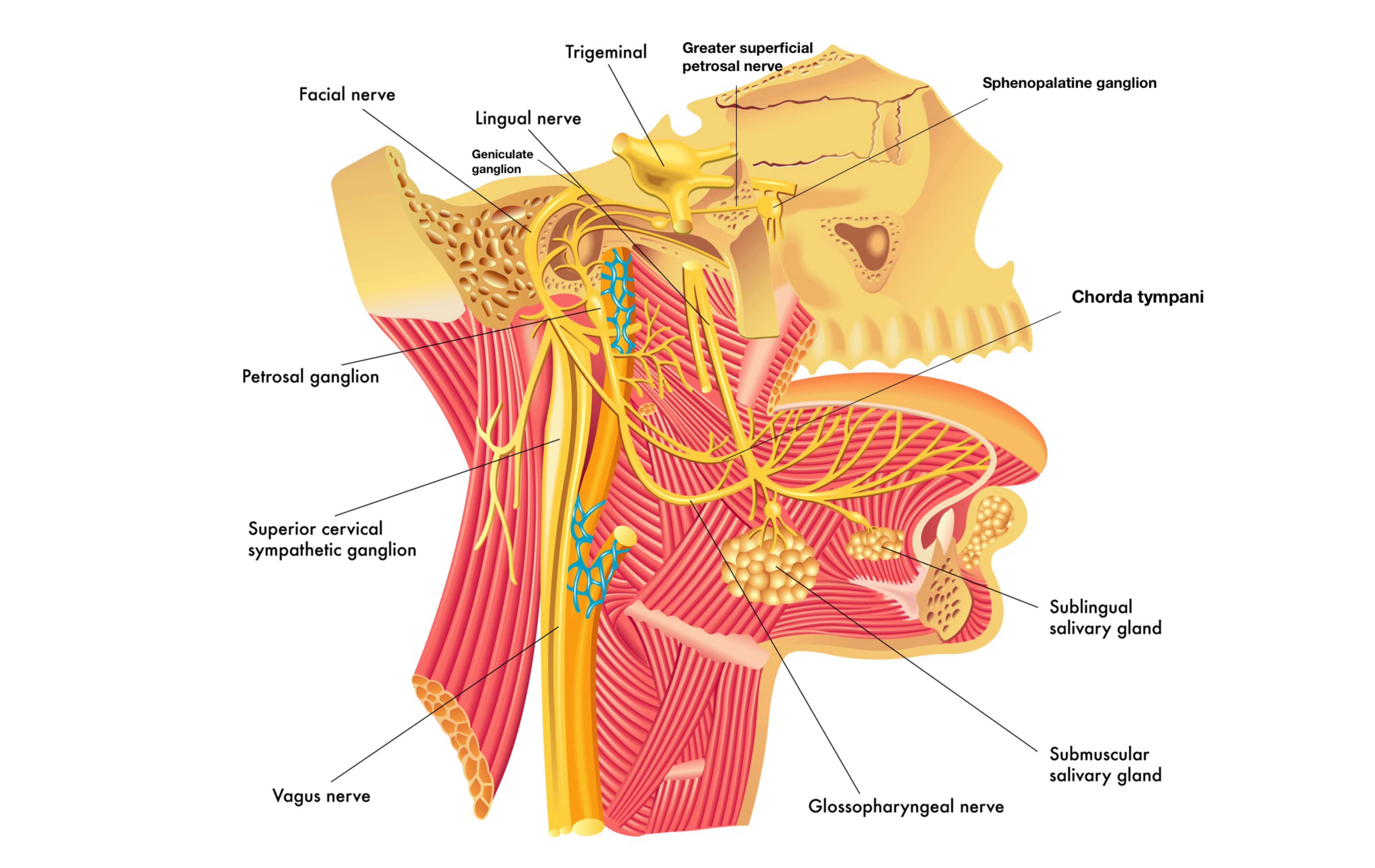
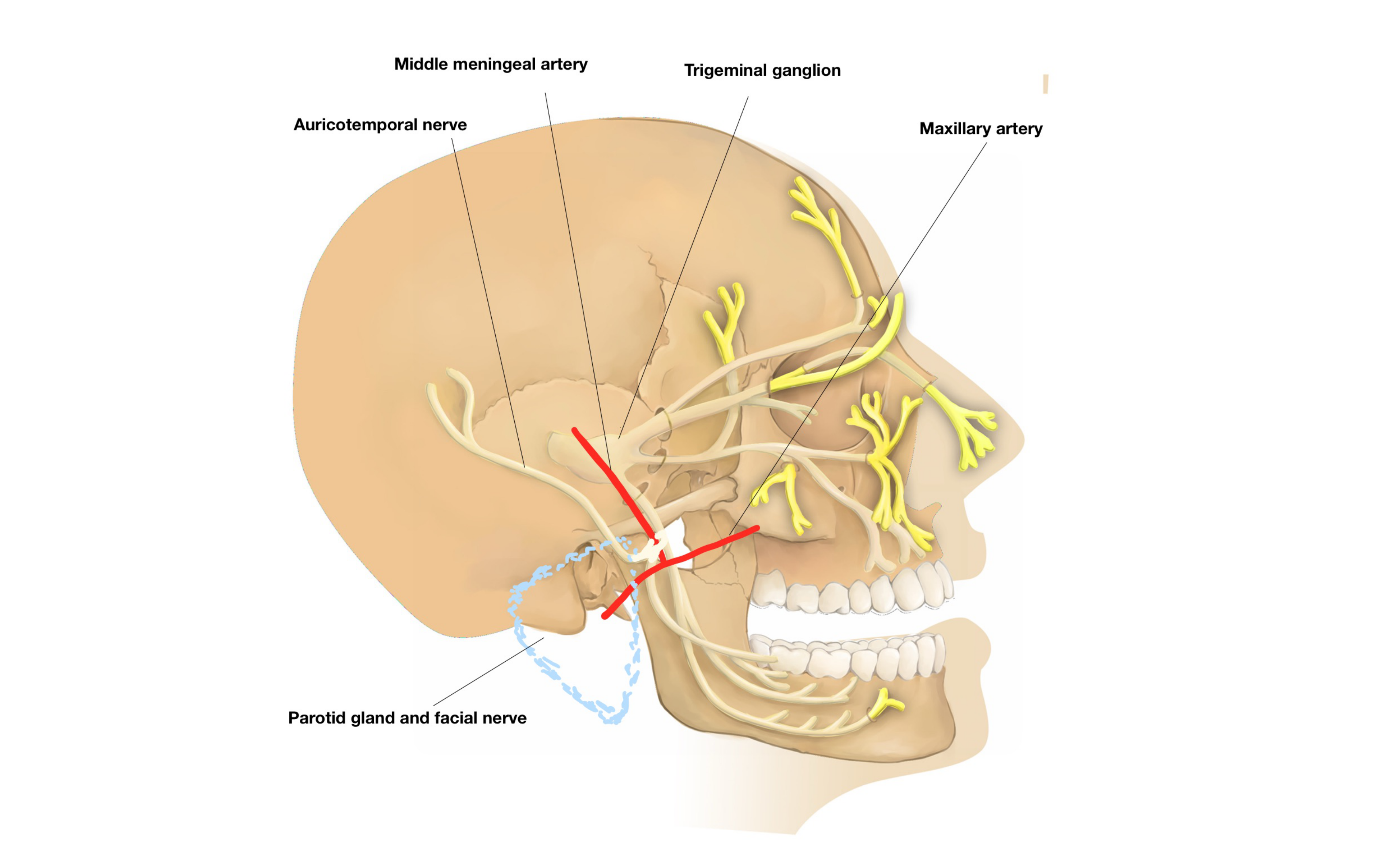

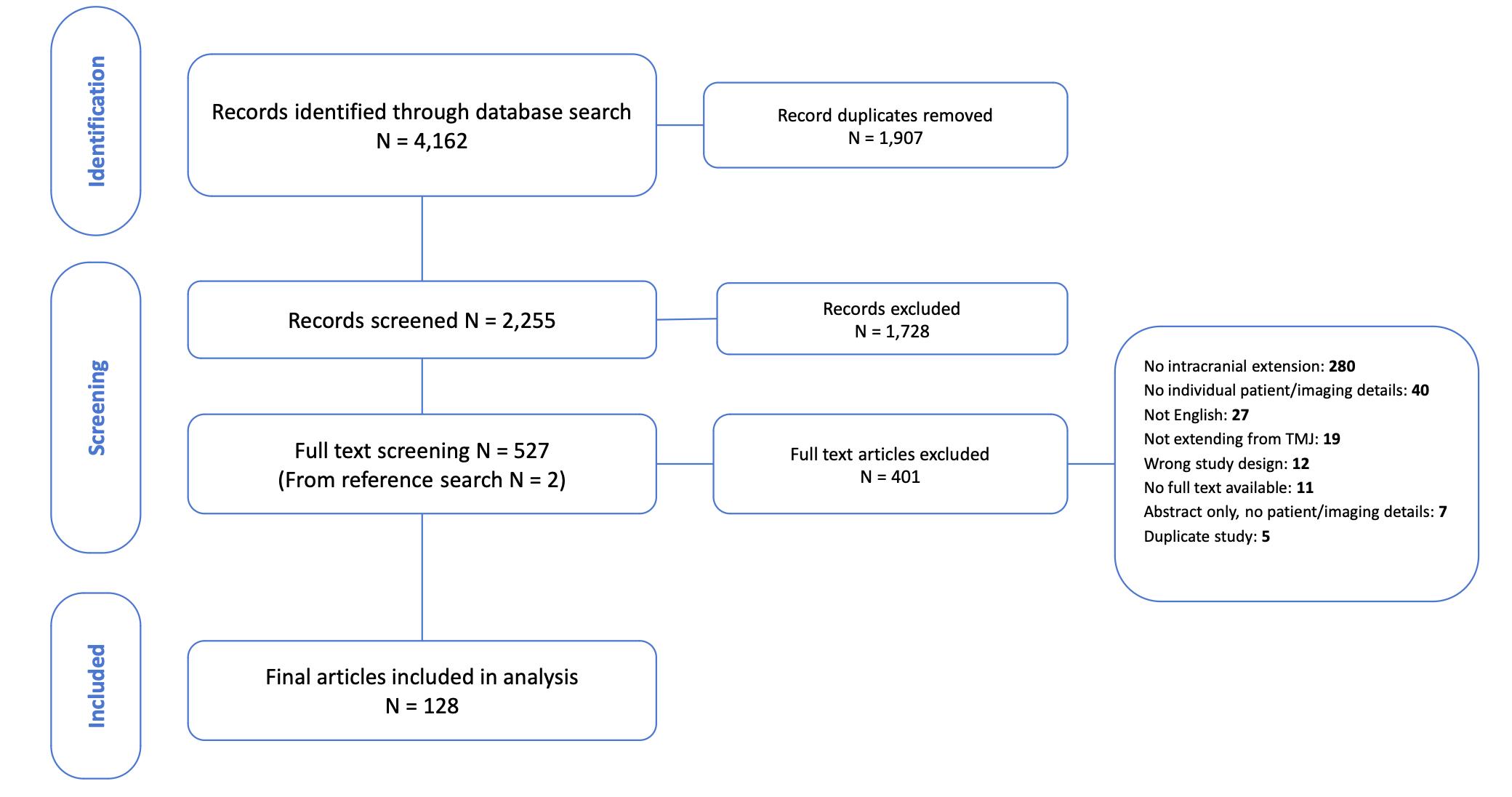
|
Variable |
N=152 (%), Mean (± SD), range |
|
Sex: Female vs Male |
72 (47%) vs 80 (53%) |
|
Laterality: Right vs Left |
73 (48%) vs 78 (51%) |
|
Age |
50 (± 16), 15-90 |
|
Duration of symptoms (months to presentation) |
34 (± 47), 3 days to 21 years |
|
Patient-reported neurological symptoms |
73 (48%) |
|
Hearing loss/Tinnitus |
51 (70%) |
|
Headache |
20 (27%) |
|
Facial numbness/paralysis |
12 (16%) |
|
Histological Diagnosis |
|
|
PVNS / Tenosynovial GCT |
66 (43%) |
|
Synovial chondromatosis (SC) |
36 (24%) |
|
Tophaceous pseudogout |
24 (16%) |
|
Both CT and MRI used in diagnostic workup |
108 (71%) |
|
Studies after 2015 (N=64) |
49 (77%) |
|
Size of lesion (cm, on imaging) |
4.4 (± 1.5) |
|
Diagnosis |
Shape |
CT Enahncing |
MR Enhacing |
Edema |
Key features |
|
PVNS / T-GCT |
Soft-tissue or cystic-solid lesion |
19 (29%) |
21 (32%) |
3 (5%) |
Low signal on MRI - due to hemosiderin (blooming on GRE) |
|
SC |
Lobulated mass, calcified bodies |
0 (%) |
2 (6%) |
0 (0%) |
Multiple calcified loose bodies on CT, small hypo-intense areas on MRI |
|
Tophaceous pseudogout |
Irregular, calcified mass |
0 (%) |
10 (42%) |
1 (4%) |
Inhomogeneous enhancement of lesion on MRI; calcified mass on CT |
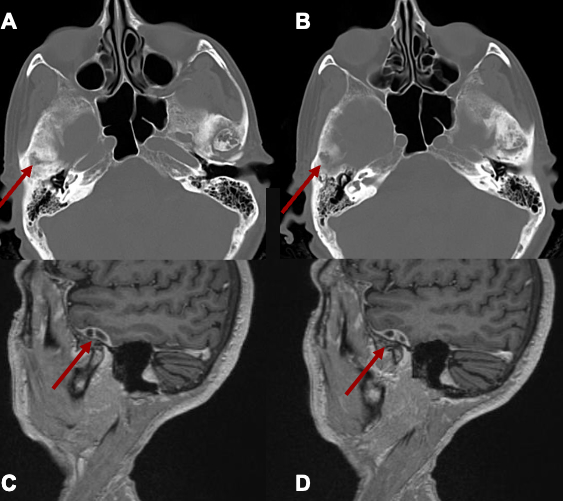
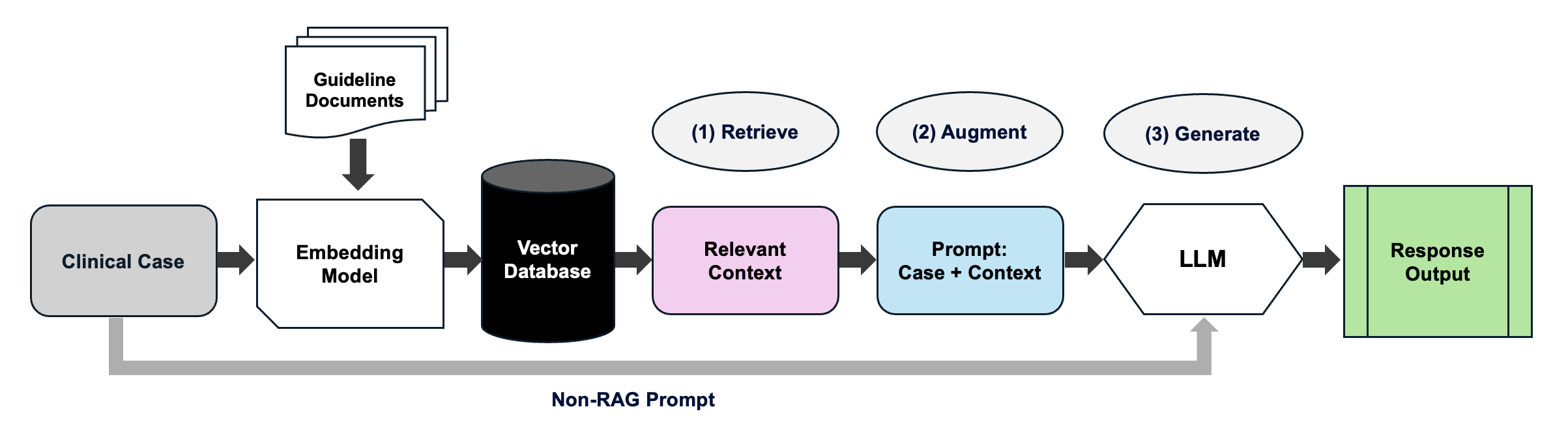
| Model | Full Adherence | Partial Adherence | Non-Adherence | Adherence Rate |
| GPT-4o | 217 | 69 | 14 | 83.8% |
| GPT-4o+RAG | 267 | 30 | 3 | 94.0% |
| o1 | 223 | 67 | 10 | 85.5% |
| o1+RAG | 262 | 35 | 3 | 93.2% |
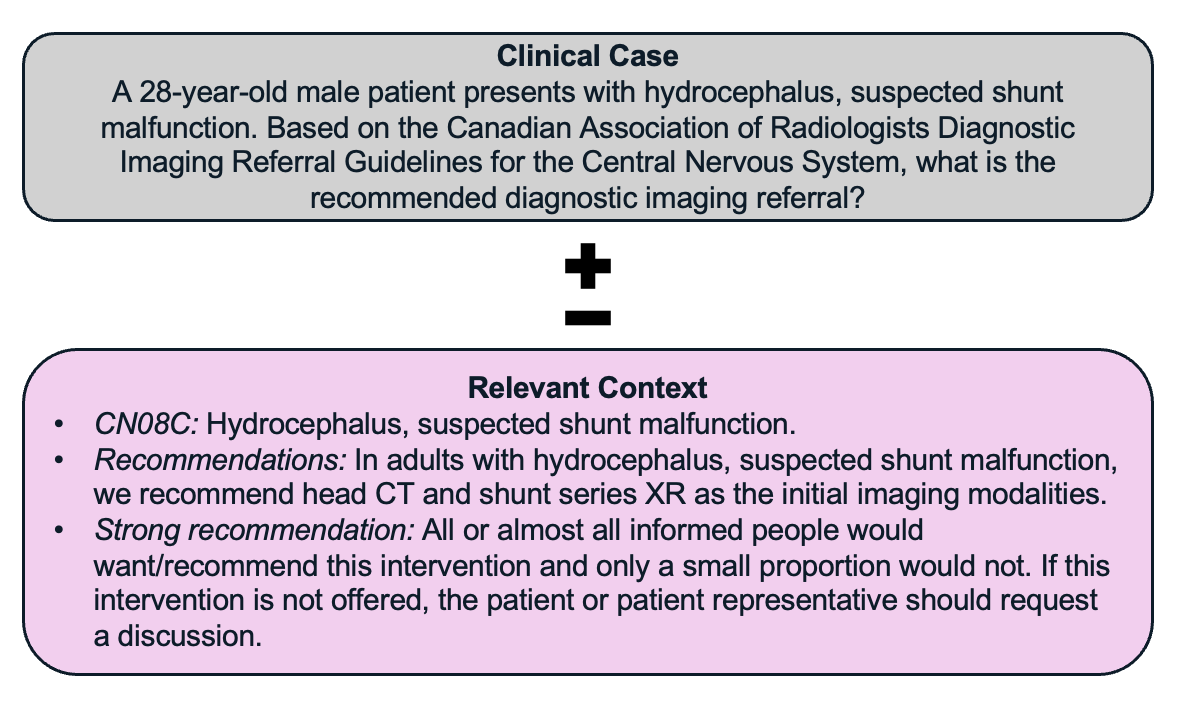
| Guideline Deviation Category | GPT-4o | GPT-4o+RAG | o1 | o1+RAG |
| Incorrect modality selection | 11 | 2 | 9 | 3 |
| Missing modality or guideline component | 1 | 0 | 2 | 0 |
| Vague or non-specific recommendation | 37 | 24 | 33 | 12 |
| Insufficient justification or clinical rationale | 34 | 7 | 33 | 23 |
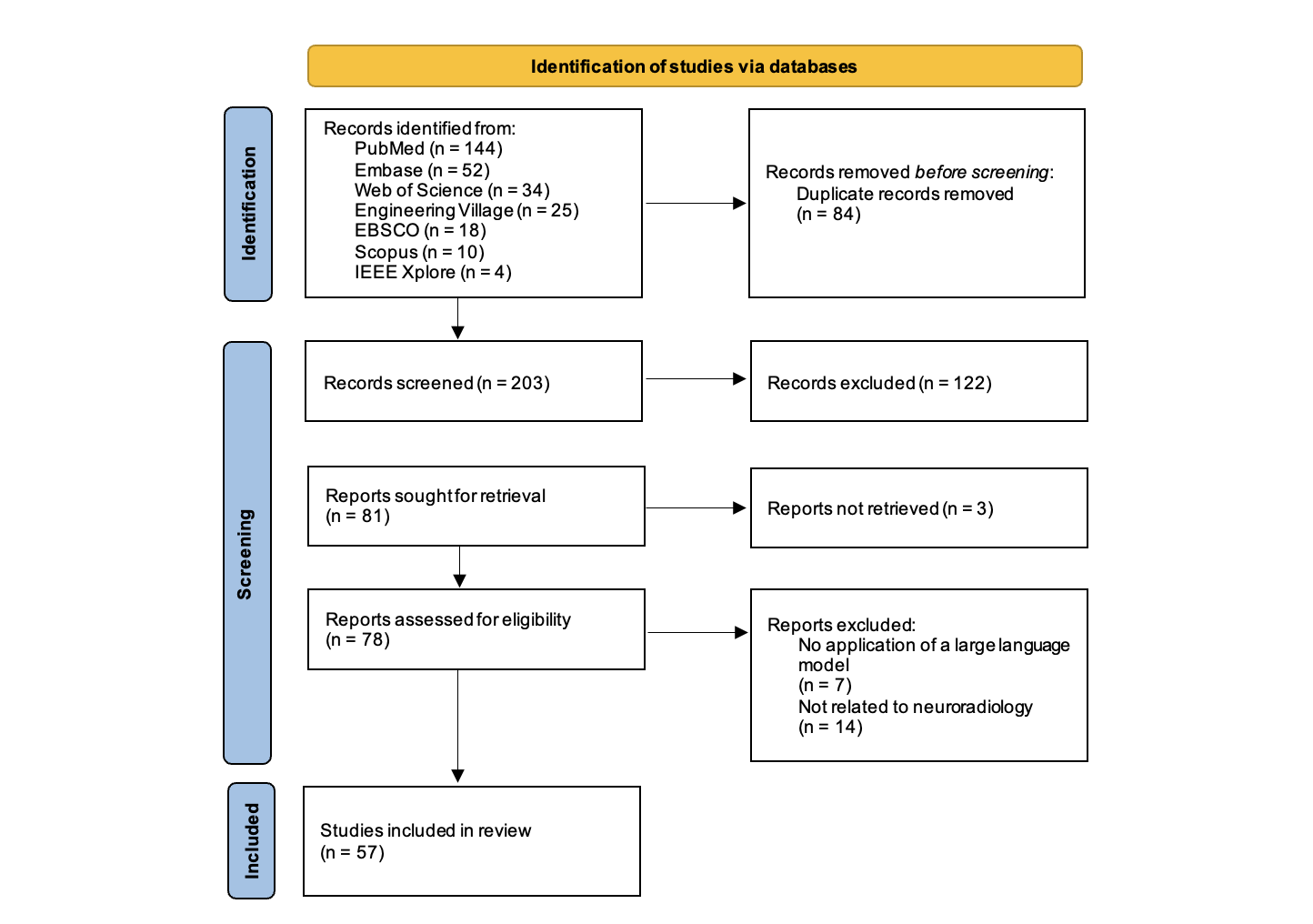
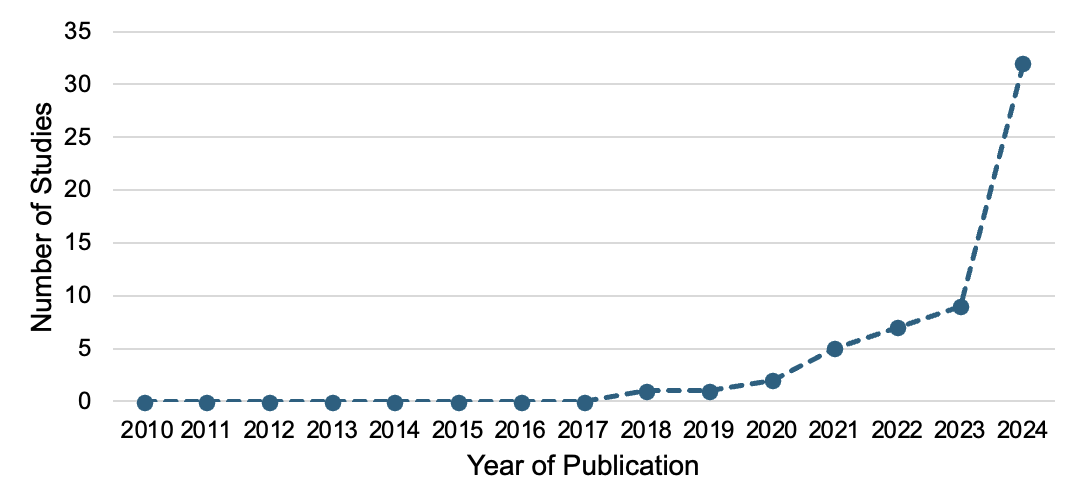
| Theme | Explanation | Example Use Case | N (%) |
| Operational Workflow Optimization | Use of LLMs to streamline radiology operations, scheduling, and reporting | Automated report generation, triage assistance | 26 (45.6%) |
| Diagnostic Decision Support | Integration of LLMs to assist in clinical interpretation, reasoning, and differential diagnosis | Generating differential lists, recommending follow-up imaging | 20 (35.1%) |
| Education and Training | Use of LLMs for radiology teaching, clinical knowledge reinforcement, and patient education | Interactive quizzes, explanation of findings to patients | 11 (19.3%) |

Study aim and objectives
- To compare and determine the similarities and differences between PBAs and monomicrobial brain abscess (MBAs).
Methodology
- Design: Single center, retrospective study design.
- Participants: 31 patients who had brain tissue-confirmed BAs with multiple pathogens and had brain imaging from 2010 to May 2024).
- Intervention: Brain imaging and histopathology evaluation.
- Comparison:Radiological features of monomicrobial brain abscess.
- Methodology: Clinical, radiological and histopathological variables.
- Radiology variables :unifocality vs multifocality, presence of lobulation and presence of heterogeneity and complexity based on 3 things ( difference on capsule thickness, difference in degree of diffusivity and marked variable MRI signal) and radiological stage (Early (I or II, without capsulation) or Late (III or IV, with capsulation).
- Ethics approval: obtained from the Hamilton Integrated Research Ethics Board.
- Statistical analysis:
-31 PBAs versus a large group of 113 MBAs previously studied in our -institution.
- Fisher’s exact and Mann-Whitney U test were used to evaluate the difference in categorical and numerical variables between the two groups respectively.
- A 2-tailed p value of < 0.05 was considered statistically significant.
- 94% of the brain abscess cases were unifocal. p = 0.0412*.
- Lobulation of brain abscess was present in 97% of the cases.
- Half of the PBAs cases (54%) showed heterogeneity and complexity on MRI.
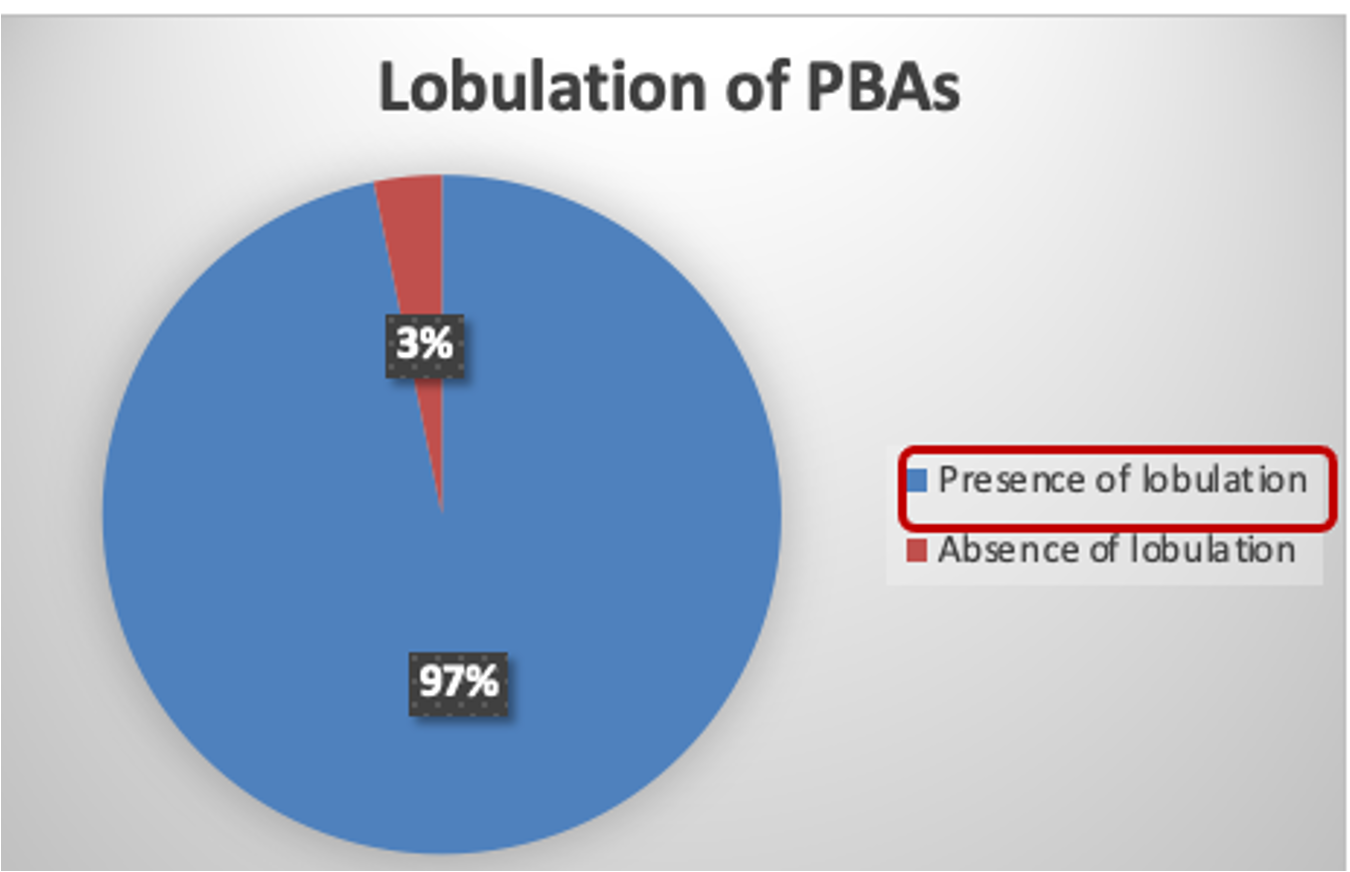
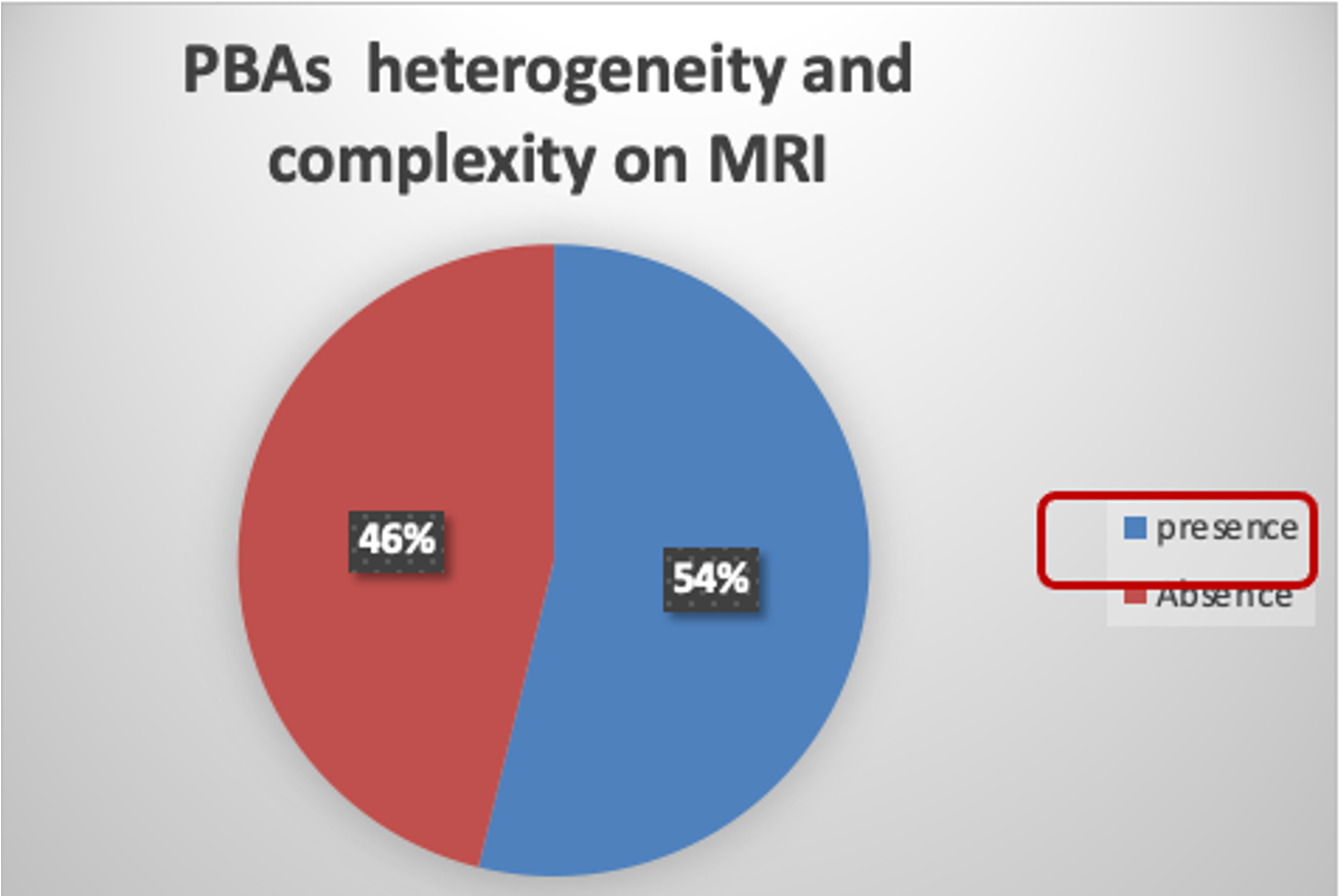
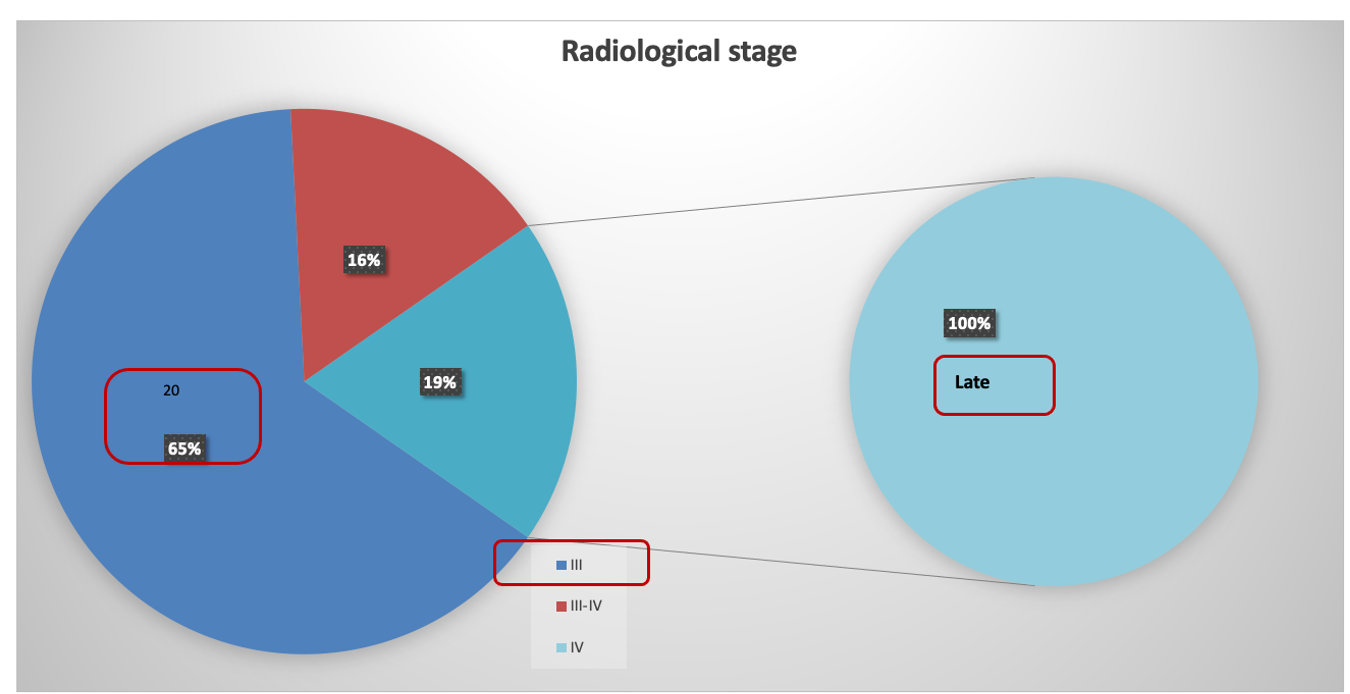
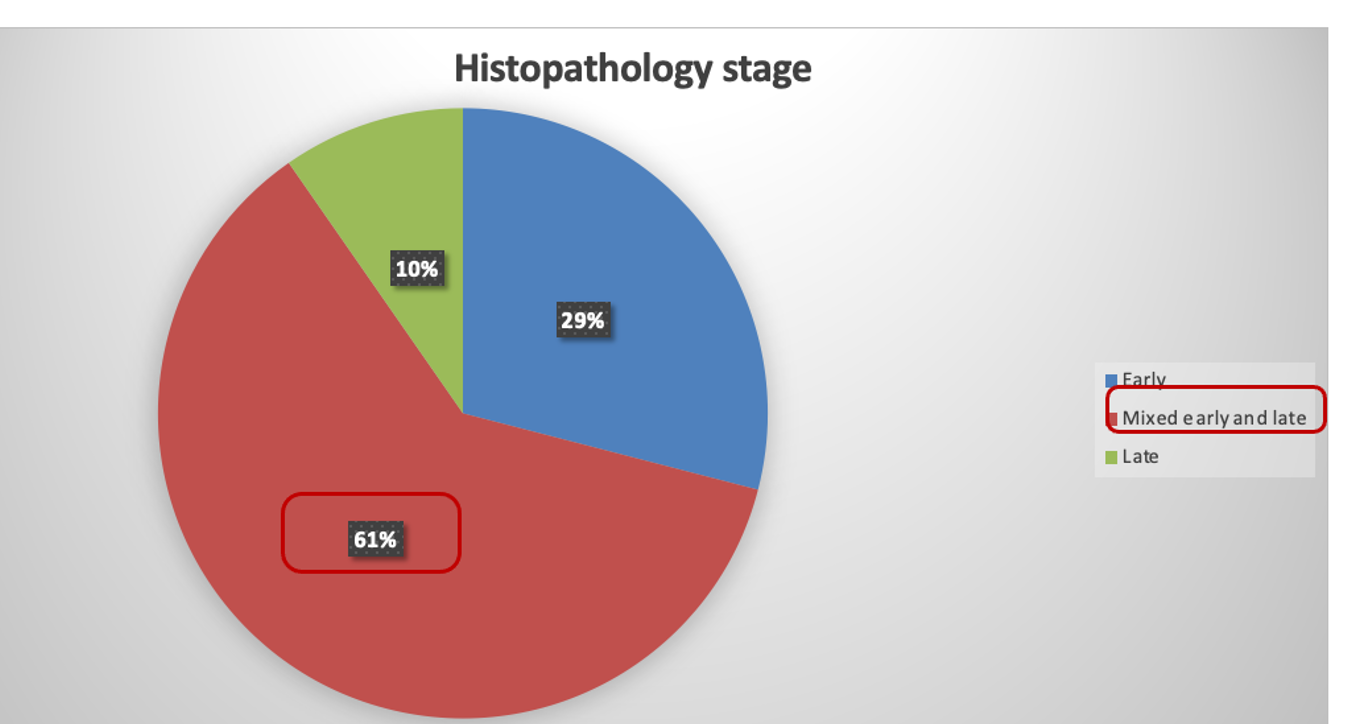
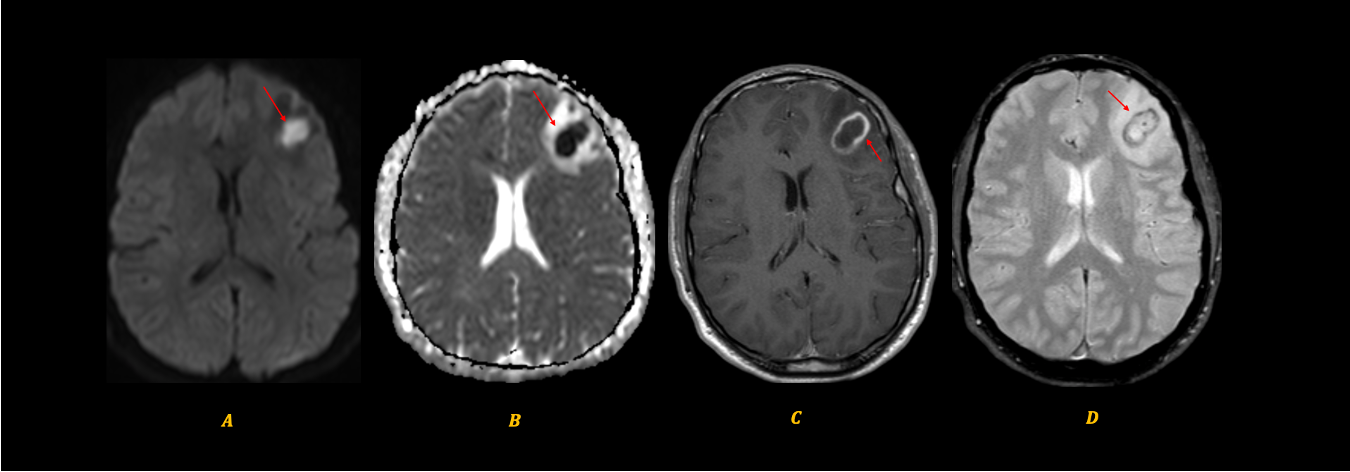
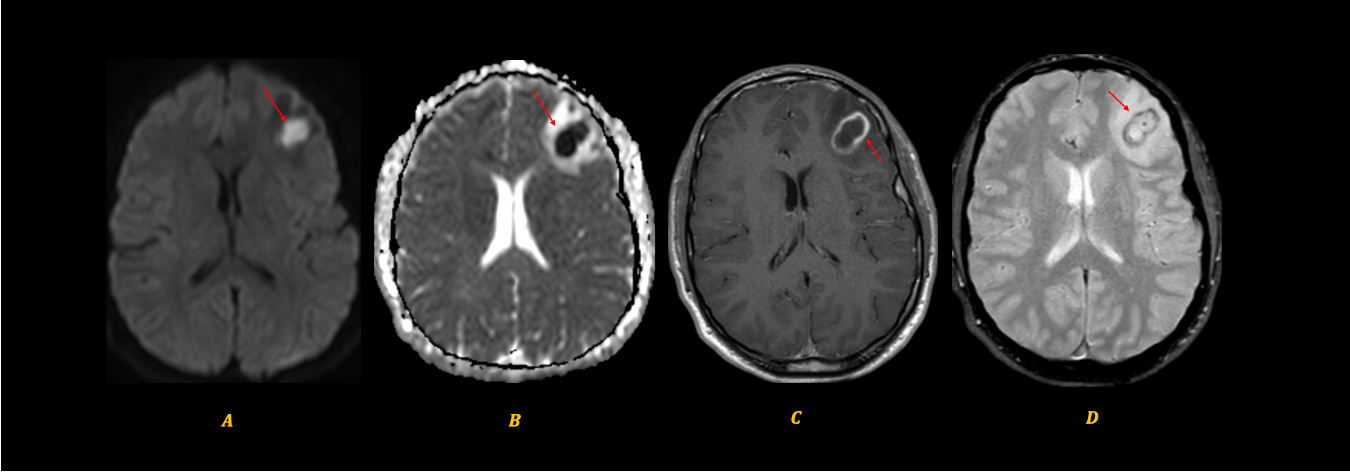
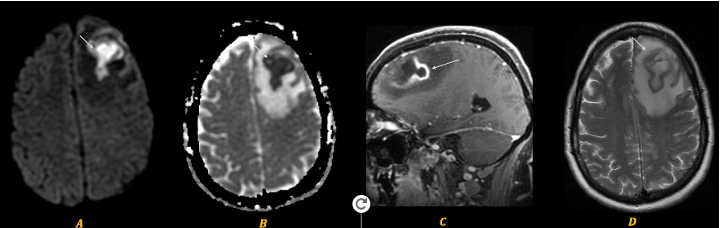
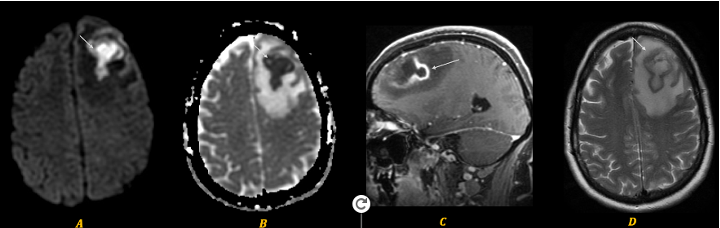
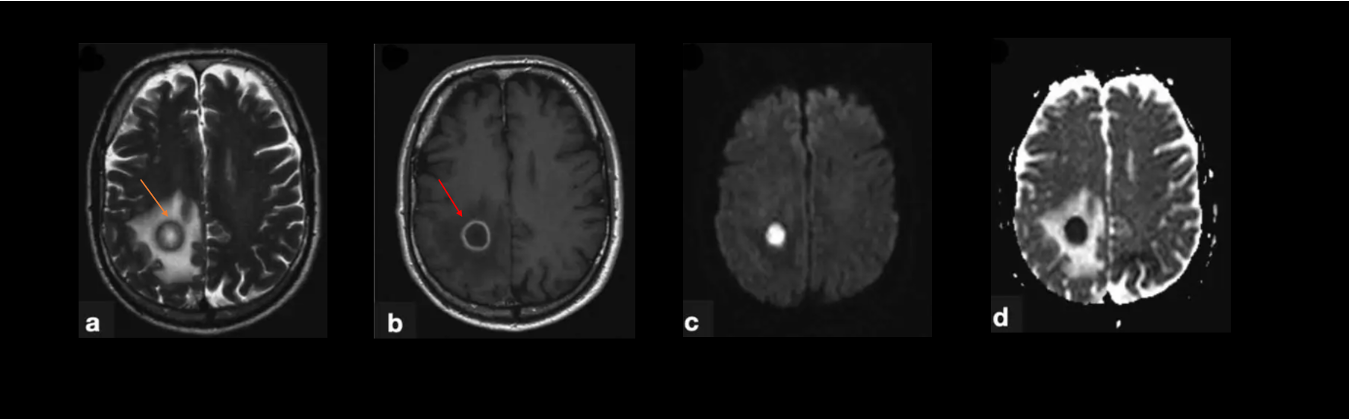
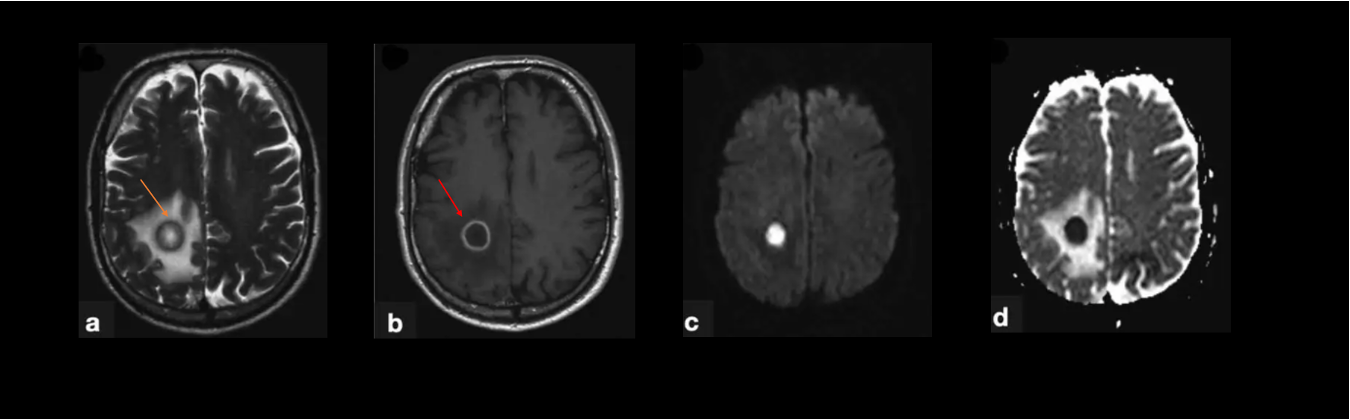
-The present study demonstrates clinical, radiological and pathological characteristics of PBAs, revealing a few novel findings.
- PBAs and MBAs had a few similarities such as nonspecific clinical presentations, a male predilection, and overall similar prognosis following surgical intervention with broad-spectrum antimicrobial therapy.
- Compared to MBAs, PBAs were more likely unifocal (94% of cases) as well as caused by pathogens of otogenic, odontogenic and/or rhinogenic sources(statistically significant).
- PBAs were highly heterogeneous with more complexity on MRI/CT imaging.
- PBAs were typically rim-enhancing lesions at late-stages, (97%) of PBAs showed the lobulation of enhancing rims on MRI and (54%) of cases demonstrated marked difference in the thickness of enhancing rim, marked difference in the degree of DWI signal, and/or marked variation in intra-lesional MRI signal.
- PBA histopathology was characterized mainly by alternating early-stage and late-stage features with regional differences, variable distribution and combinations of 2-4 pathogens. Streptococcus species are the most commonly associated with intracranial abscesses and found in most PBAs in this series.
- PBA pathological stages were somewhat non-corresponding to radiological stages , due to a few reasons including undersampling of the lesion for histopathological examination, and/or disease progression during the interval between preoperative MRI/CT and operation.
- As such, PBAs/BAs should be staged by a clinico-radiologico-pathological approach.

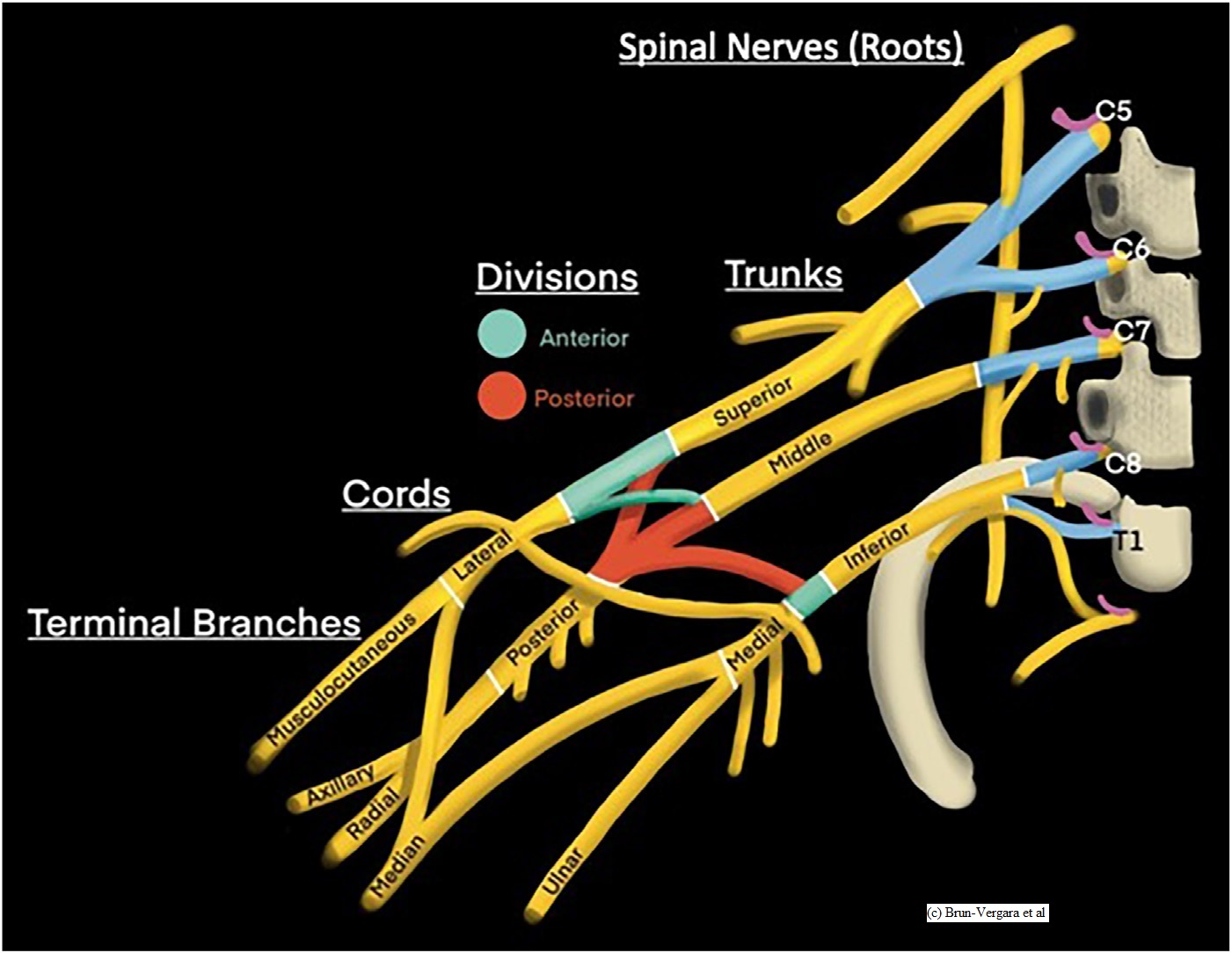
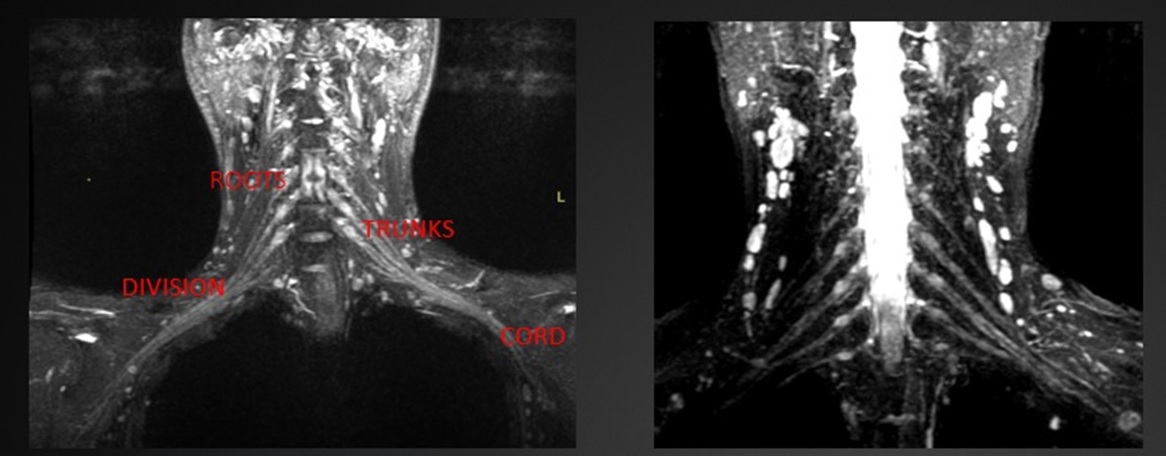
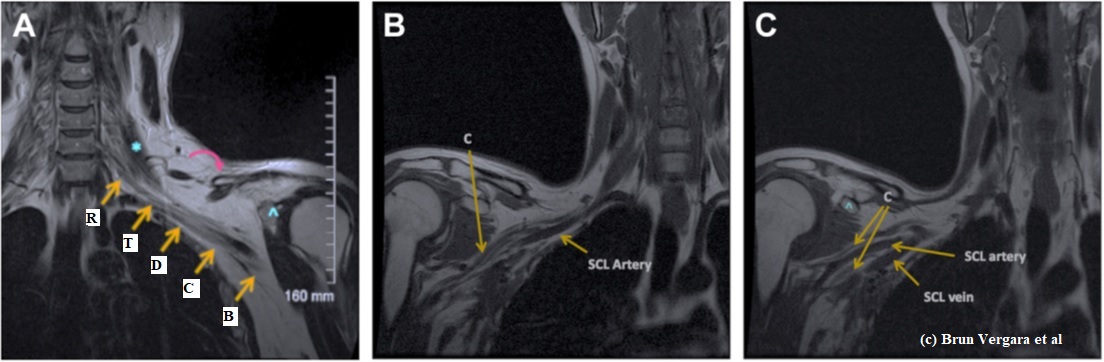
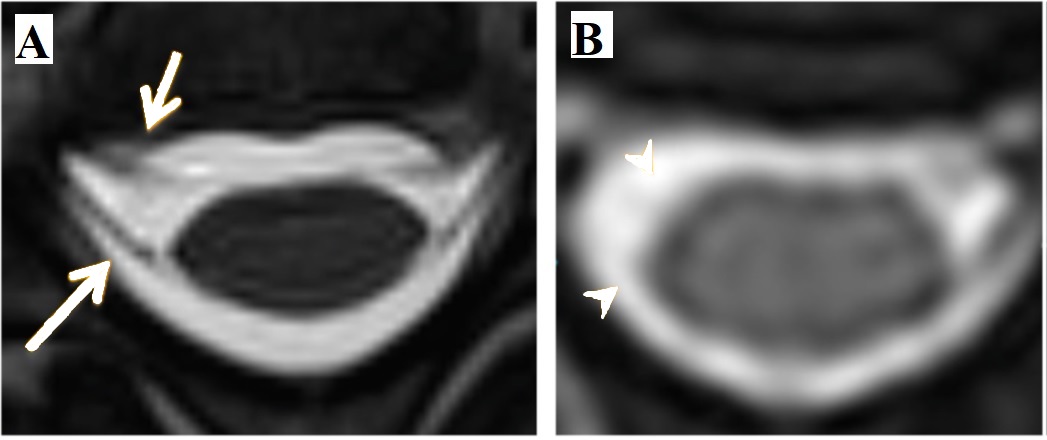
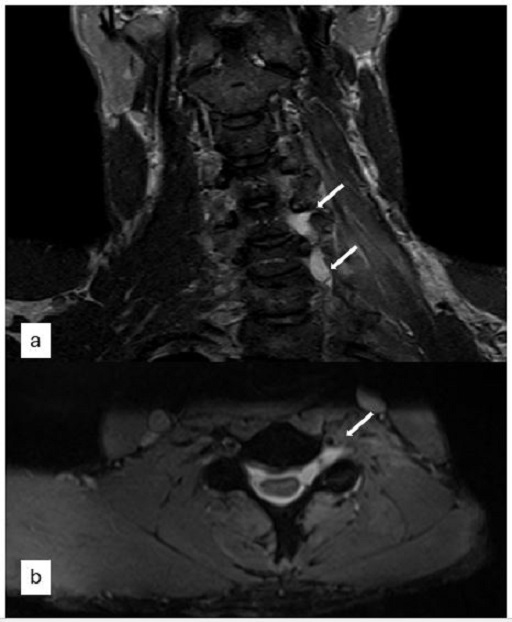
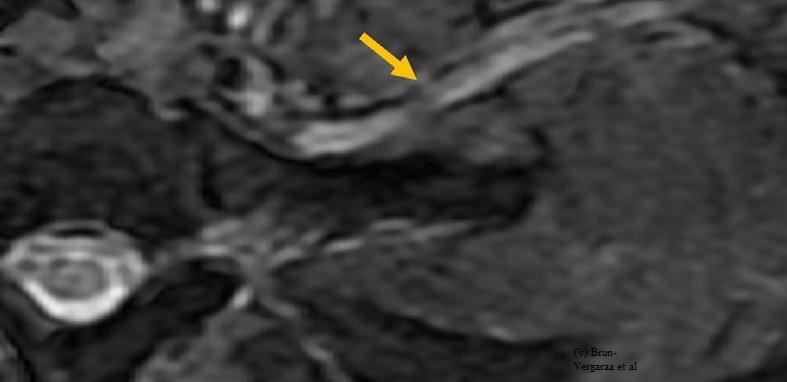

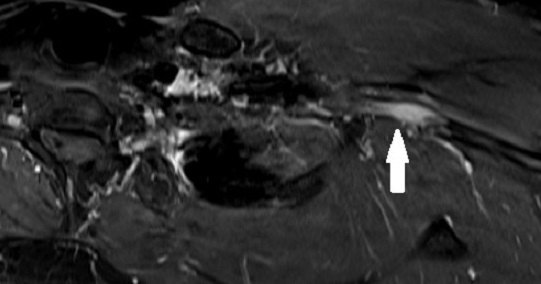
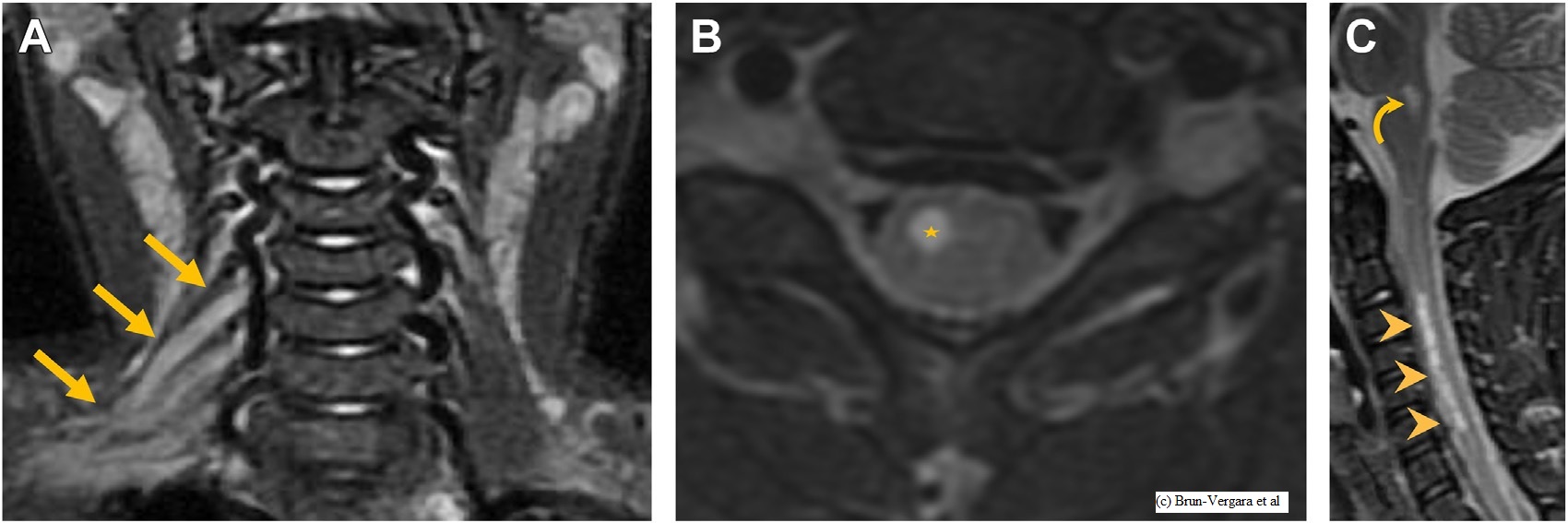

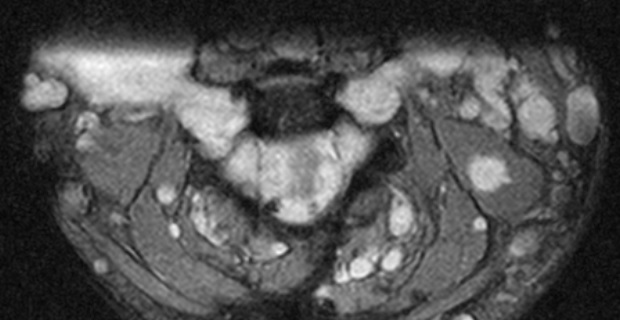
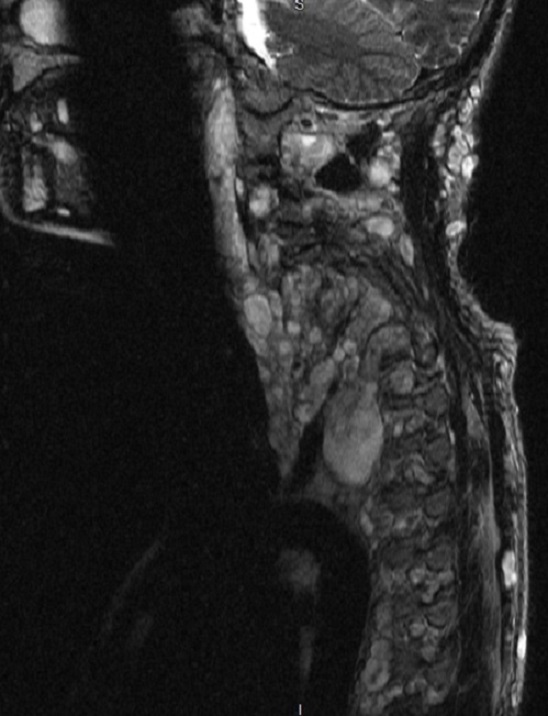
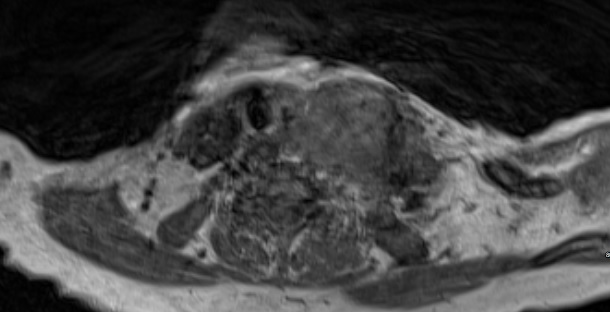
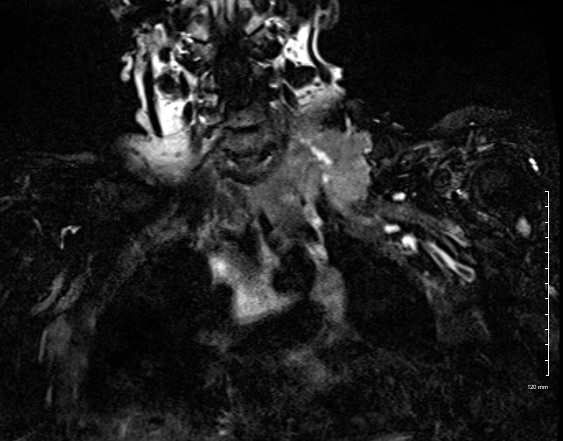
Blunt cervical trauma, especially from assaults and strangulation, can cause Blunt Cerebrovascualr Injury (BCVI) , a rare but potentially fatal condition. Diagnosis is challenging due to non-specific symptoms with an incidence of 0.5% to 2%, higher in assault and strangulation cases. CTA is the most commonly used imaging modality for BCVI, but guidelines on when and how to use it remain unclear. The Biffl Classification is a grading scheme used to describe the spectrum of BCVI seen on angiography.
Primary Objective: To evaluate the utility of neck CTA in detecting BCVI from blunt cervical trauma, including assaults and strangulation.
Secondary Objectives
Exclusion Criteria: Penetrating injuries, Pre-existing cerebrovascular disease, No CTA performed, Incomplete records
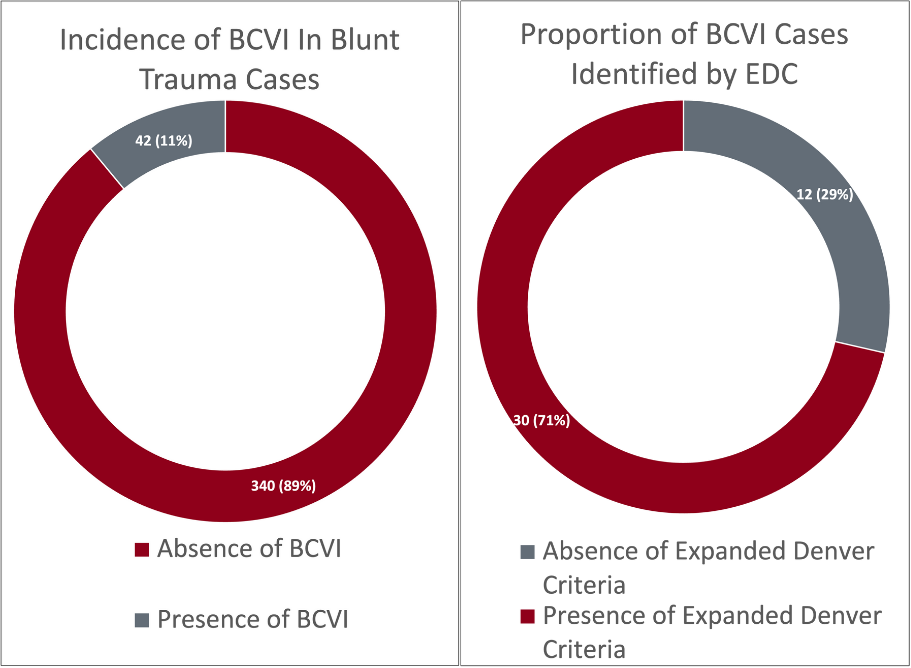
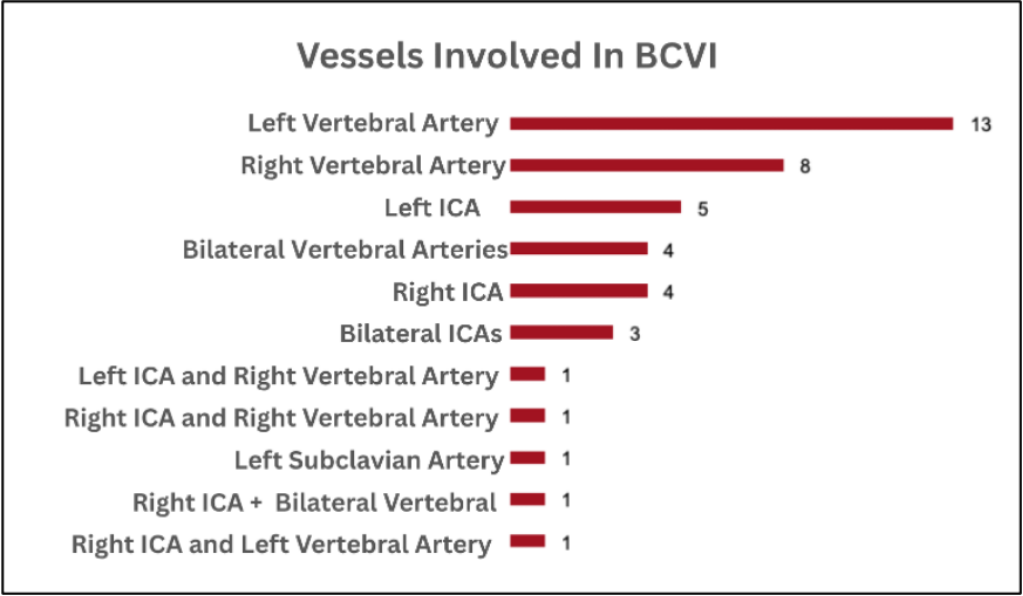
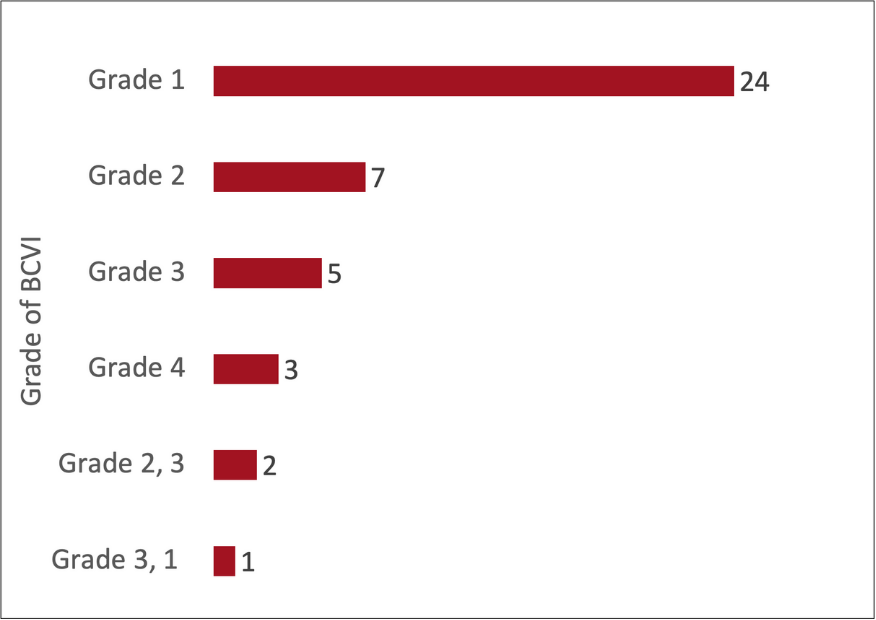
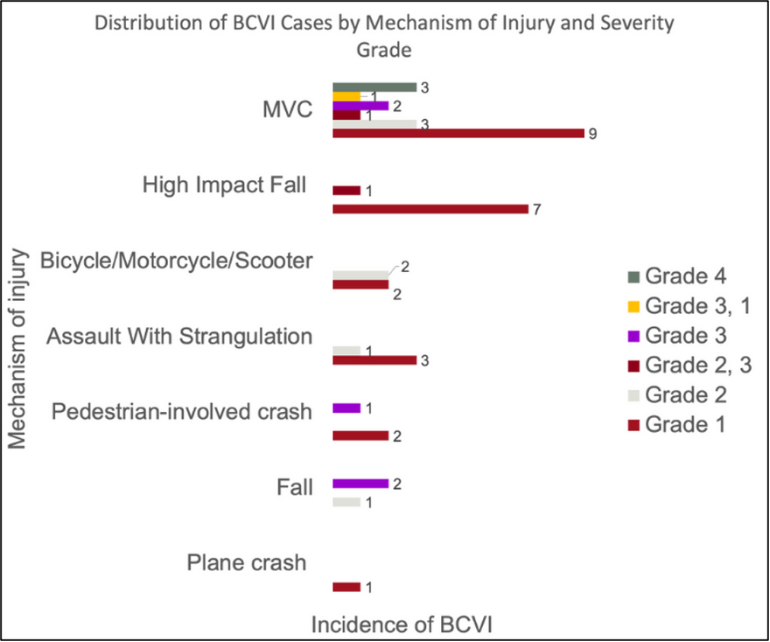
Case report:
A 36-year-old patient sought medical attention due to acute onset of severe headache graded 10/10 in intensity with radiation to neck, photophobia, nausea, and multiple episodes of emesis. Neurological exam was only relevant for confusion without any focal deficits. His past medical history relevant for untreated anxiety and depression as well as active smoking of 10-cigarrets per day.
Computed tomography (CT) angiogram (CTA)/ CT head showed large intraventricular hemorrhage (IVH) in right lateral ventricle with hydrocephalus without any vascular abnormalitiesy. An external ventricular drain. He underwent a magnetic resonance (MR)/MR angiogram (MRA) of his head on day 3 of his admission showing a normal brain parenchyma and absence of any features to suggest an underlying vascular abnormality. He was started on nimodipine 60 mg every 4 hours. Throughout his admission, his headache persisted with bouts of intense thunderclap-headaches and confusion.
On day 15 of his admission, he underwent diagnostic cerebral angiography showing segmental vessel caliber narrowing involving bilateral internal carotids, basilar artery, anterior cerebral, middle cerebral and posterior cerebral arteries bilaterally. On day 17, he developed acute onset of global aphasia, right hemibody weakness and homonymous hemianopia. His National Institutes of Health Stroke Scale (NIHSS) at the time of assessment was 8. A head CTA showed severe diffuse intracranial stenosis involving the circle-of-Willis bilaterally. He was taken to the angiography suite for chemical spasmolysis with verapamil. Following infusion of 15 mg verapamil within both internal carotid arteries and left vertebral artery, there was significant interval improvement in multifocal stenoses. Radiographic improvement was also associated with complete resolution of his symptoms. He was ultimately discharged home 28 days after his admission with complete resolution of his symptoms. His 3-month follow up diagnostic cerebral angiogram showed normal intracranial vasculature.
Discussion and Conclusion:
Reversible cerebral vasoconstriction syndrome (RCVS) is defined clinically by recurrent thunderclap headaches associated sometimes with seizures and focal neurological deficits, and radiologically with intermittent spasms in cerebral arteries that would resolve in 3 months’ time. It can present with multiple bleeding patterns, mostly cortical subarachnoid and intracerebral hemorrhage (ICH). Overall, isolated intraventricular hemorrhage is a rare cause of ICH, constituting only 3.1% of all hemorrhagic stokes. There are 4 reported cases of RCVS presenting with IVH associated with ICH/stroke (Table 1). This case highlights rarity of presentation of RCVS and a further signifies the utility of response to intra-arterial spasmolytics as adjunct in the diagnosis of difficult cases of RCVS. Further retrospective and prospective data are needed.
Refrences: [1] Kaufmann J, Buecke P, Meinel T, Beyeler M, Scutelnic A, Kaesmacher J, Mujanović A, Dobrocky T, Arsany H, Peters N, Z'Graggen W, Jung S, Seiffge D. Frequency of ischaemic stroke and intracranial haemorrhage in patients with reversible cerebral vasoconstriction syndrome (RCVS) and posterior reversible encephalopathy syndrome (PRES) - A systematic review. Eur J Neurol. 2024 May;31(5):e16246. doi: 10.1111/ene.16246. Epub 2024 Mar 12. PMID: 38470001; PMCID: PMC11235994. [2] Dakay K, McTaggart RA, Jayaraman MV, Yaghi S, Wendell LC. Reversible cerebral vasoconstriction syndrome presenting as an isolated primary intraventricular hemorrhage. Chin Neurosurg J. 2018 Jun 4;4:11. doi: 10.1186/s41016-018-0118-7. PMID: 32922872; PMCID: PMC7398312. [3]Wilson D, Marshall CR, Solbach T, Watkins L, Werring DJ. Intraventricular hemorrhage in reversible cerebral vasoconstriction syndrome. J Neurol. 2014 Nov;261(11):2221-4. doi: 10.1007/s00415-014-7499-0. Epub 2014 Sep 21. PMID: 25240397; PMCID: PMC4221649. [4]Fujita S, Hayashi M, Sato S, Hiramoto Y, Nakayama H, Ito K, Saito N, Iwabuchi S. A case of reversible cerebral vasoconstriction syndrome with intracranial hemorrhage. Brain hemorrhages. 2020 Dec; 1 (4): 192-195. Doi:10.1016/j.hest.2020.10.006 [5]Tark BE, Messe SR, Balucani C, Levine SR. Intracerebral hemorrhage associated with oral phenylephrine use: a case report and review of the literature. J Stroke Cerebrovasc Dis. 2014 Oct;23(9):2296-300. doi: 10.1016/j.jstrokecerebrovasdis.2014.04.018. Epub 2014 Aug 23. PMID: 25156786; PMCID: PMC4180794.
Table 1: Case Series Isolated Intraventricular Hemorrhage Presenting as RCVS
|
Authors |
Patient demographics and symptoms |
Medications |
Workup |
Treatment |
Follow up |
|
Dakay et al |
58-year-old female Worse headache History of chronic migraines, depression, seasonal allergies
|
Serotonergic medications, bupropion, sertraline, decongestants |
Negative toxicology. Catheter cerebral angiography: multifocal areas of irregular narrowing in the distal posterior cerebral artery branches and distal left middle cerebral artery. |
IV nimodipine then oral verapamil, magnesium gluconate |
Resolution of symptoms at 2 months |
|
Wilson et al |
47-year-old male Sudden occipital headache, nausea, vomiting, left facial weakness
|
Regular intranasal oxymetazoline for coral symptoms |
CT head: right posterior cerebral artery infarction and subarachnoid blood in the prepontine cistern and fourth ventricle. Catheter cerebral angiography: focal stenosis of right middle cerebral artery. MRI brain: multiple areas of restricted diffusion right MCA, PCA. |
Nimodipine 60 mg 4 times a day |
Resolution of symptoms 2 days from admission. 3 months: repeat catheter angiogram showed resolution. |
|
Fujita et al |
54-year-old female Known to have migraine presented with headaches and then was discharged (unknown day), re-presented 6 days after initial presentation with consciousness disorder, GCS 15 |
Not reported |
MR brain/ MRA: left–right difference in the vertebral arteries, suggesting dissection of the right vertebral artery. CTA was negative. Day 5 from initial presentation: CT head/CTA right frontal lobe bleed and anterior cerebral artery and peripheral middle cerebral arteries vasospasm. |
Day 7 from initial presentation: peripheral cerebral edema on CT scan, no change neurologically, so craniotomy hematoma removal done then verapamil 120 mg started. |
MRA head: improved vasospasm in 2 weeks, mRS 3 and discharged to rehabilitation center 3 months follow up mRS0. 4 months diagnosed with hydrocephalus and lumboperitoneal shunt inserted. |
|
Tark et al |
59-year-old female Severe headache, right-sided hemiparesis, aphasia, and left gaze deviation
|
Decongestants |
CT head: left hemispheric ICH with intraventricular and subarachnoid extension. CTA and MRA: negative. Catheter cerebral angiography: focal narrowing distal vessels.
|
Brain biopsy at the time of surgical evacuation not diagnostic. |
Discharged 22 days to rehabilitation with bowel and urinary incontinence, ataxia, right sided weakness, and expressive aphasia. 72 days from presentation: symptoms improved and discharged home. |



Carotid blowout syndrome is a life-threatening complication in head and neck cancer patients. Endovascular coiling of the internal carotid artery (ICA) or pseudoaneurysm is a commonly employed salvage treatment to control hemorrhage. Coil extrusion refers to the protrusion or migration of embolization coils out of the vessel or into adjacent structures. This event is exceedingly rare but can occur, particularly in patients with prior radiotherapy to the neck. Radiation-induced soft tissue radionecrosis can lead to chronic wound breakdown, creating fistulous tracts that permit coil exposure. Though rare, coil extrusion carries serious risks, including hemorrhage and infection, warranting high clinical suspicion in post-radiated patients who have undergone carotid occlusion.
We report a case of a 58-year-old man with advanced nasopharyngeal carcinoma (NPC) treated with definitive chemoradiation. One year after treatment, he had left ICA blow out, resulting in massive epistaxis. He was managed via endovascular coil embolization of the left ICA. The patient recovered and remained symptom-free, until six months later, when he presented with foreign body sensation in the back of his nose. Nasal endoscopy revealed extrusion of coil material in the nasopharynx. There were no signs of active epistaxis or neurological deficit, thus conservatively managed. On subsequent follow up, he developed left paraspinal abscess which was treated with antibiotic without removal of the coil.
Figures 1a and 1b: Axial and coronal post-contrast CT images during the presentation of foreign body sensation post coiling demonstrated mild coil extrusion (star) into the nasopharyngeal lumen through the left nasopharyngeal
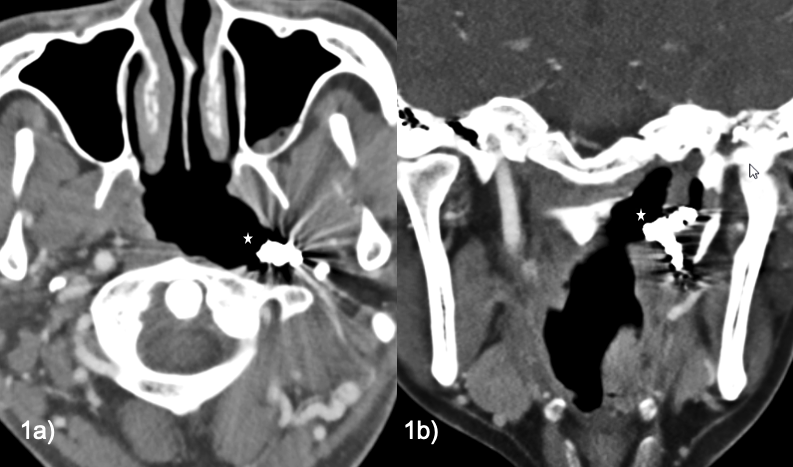
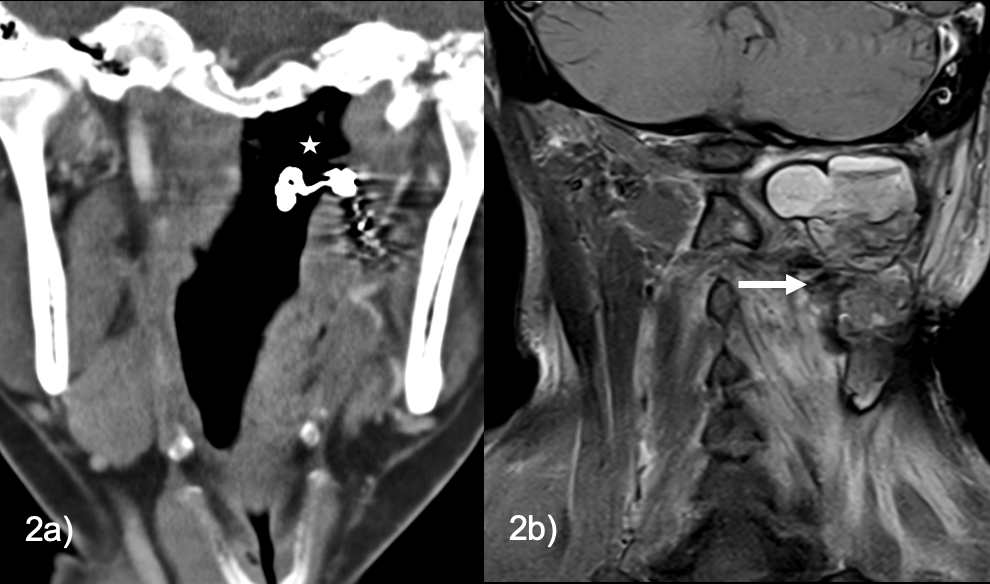
This case illustrates a rare delayed complication of carotid artery coiling in an irradiated neck, likely facilitated by radiation-induced tissue necrosis and vessel wall fragility leading to coil extrusion into the nasopharynx. Coil extrusion carries significant risks of hemorrhage and infection, and in this case, managed conservatively. Singh et al. (2018) described a coil extrusion 18 months after coiling a cavernous internal carotid artery (ICA) pseudoaneurysm, successfully removed endoscopically without complications, whereas Lin et al. (2010) reported a severe extrusion complicated by septicemia requiring debridement and flap reconstruction. A review by Vinciguerra et al. (2024) of ten ICA coil extrusion cases identified radiotherapy as a predisposing factor and recommended prompt angiographic evaluation and surgical intervention to address such complications. Effective management requires urgent angiographic evaluation and careful surgical technique: extruded coil segments should be removed without traction to prevent catastrophic hemorrhage while preserving intravascular portions; flap reconstruction can promote healing and mitigate infection risk in irradiated tissues. Long-term follow-up remains essential to monitor for recurrence or late-onset complications.
Carotid artery coil extrusion, though rare, represents a serious complication post-radiation therapy requiring high clinical suspicion, early recognition, and multidisciplinary management. Gentle surgical removal and reconstruction are central to effective treatment, emphasizing careful long-term surveillance to ensure patient safety.
1. Lin HW et al. Auris Nasus Larynx 2010;37:390–393.
2. Singh A et al. Neurointervention 2018;13:66–69.
3. Vinciguerra A et al. Int Forum Allergy Rhinol 2024;14:1529–1534.

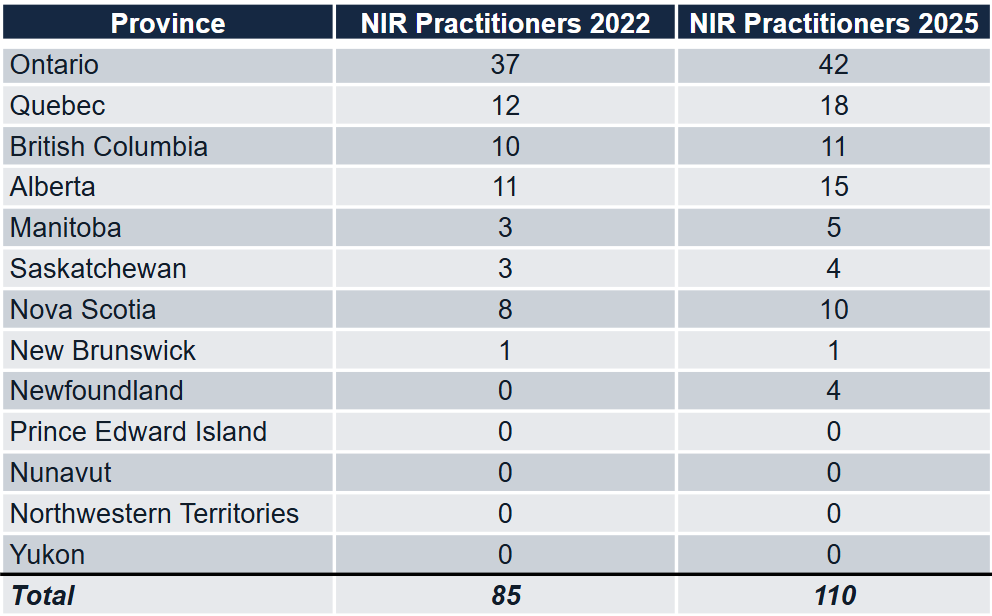
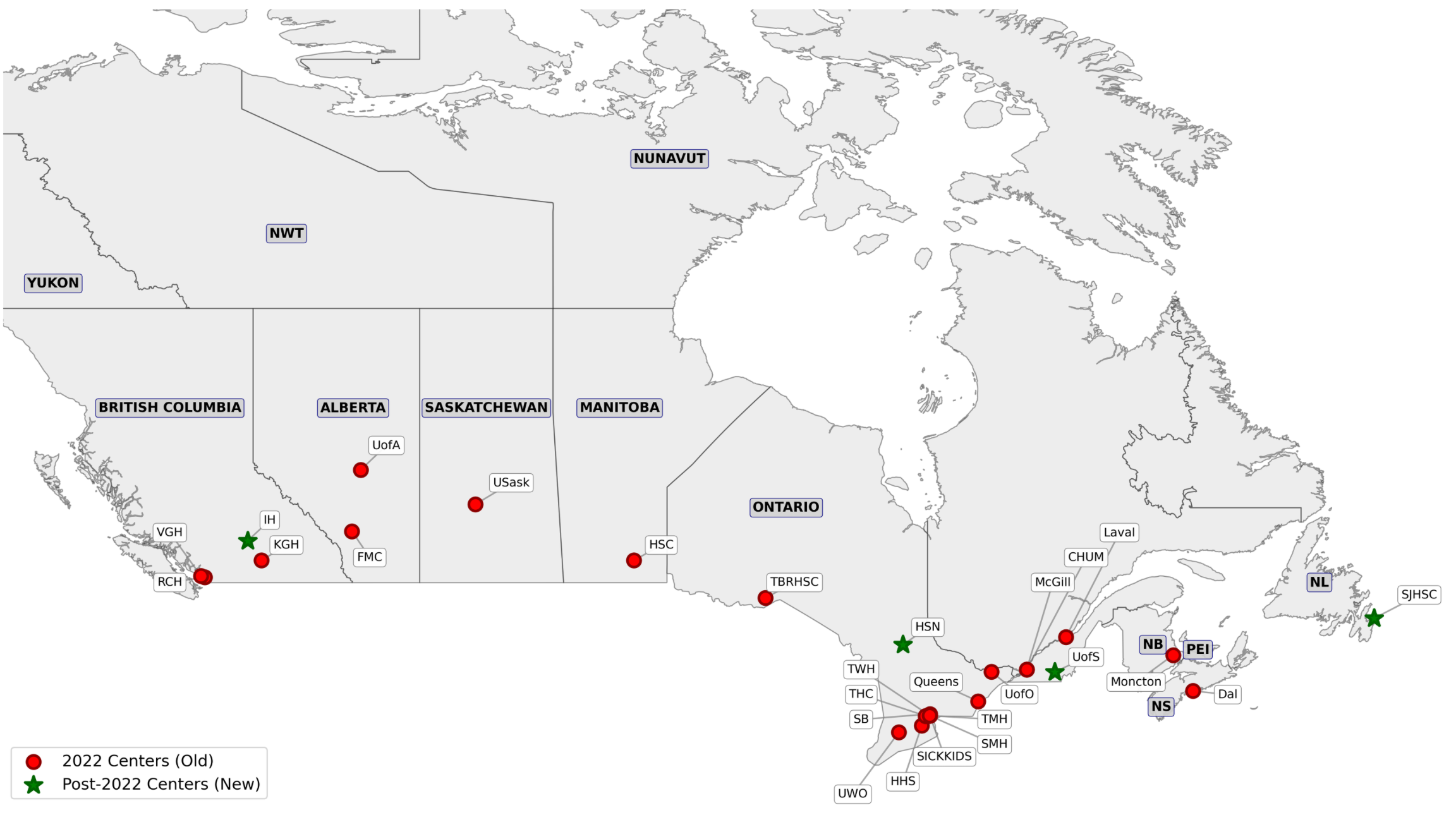
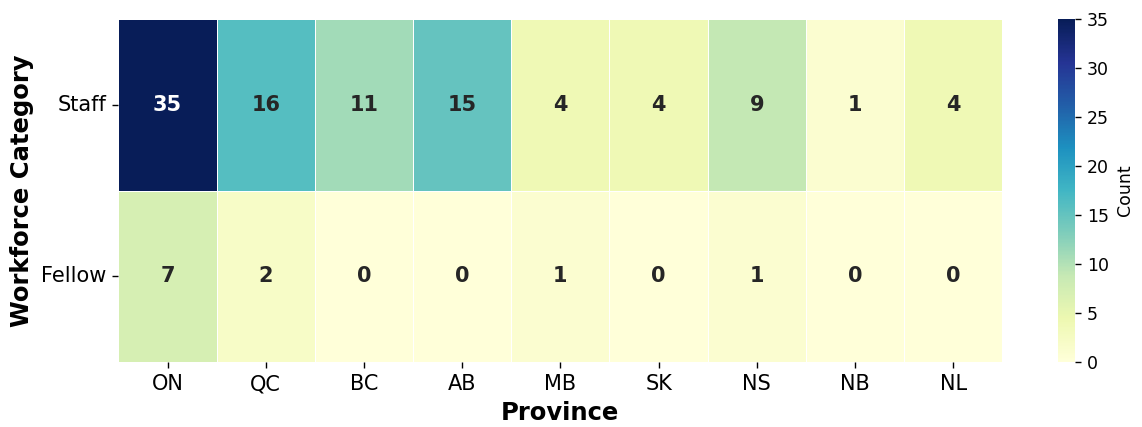
Occipital nerve stimulation (ONS) is a minimally invasive, adjustable, and reversible intervention used for managing refractory craniofacial pain unresponsive to conventional therapies. This study reviews a 15-year experience at Hôpital Enfant-Jésus, CHU de Québec, analyzing the efficacy and factors influencing ONS outcomes across diverse craniofacial pain conditions.

Methods
A retrospective cohort analysis was performed, encompassing patients diagnosed with occipital neuralgia, cluster headaches, neuropathic pain, migraines, and other craniofacial pain syndromes who underwent ONS implantation.
Outcome measures included changes in pain intensity (Numerical Pain Rating Scale, NPRS), quality of life assessments (Brief Pain Inventory, BPI; Short Form Health Survey 36, SF-36), and patient-reported improvements, evaluated at baseline, one year, and at the most recent follow-up. All patients underwent an initial trial stimulation phase to assess responsiveness prior to permanent device implantation.
Surgical Approaches for ONS
Implanting subcutaneously 1 or more electrodes unilaterally or bilaterally medial to lateral in the occipital region to cover the greater, lesser and third occipital nerves. Each implantation follows a trial and permanent phases.
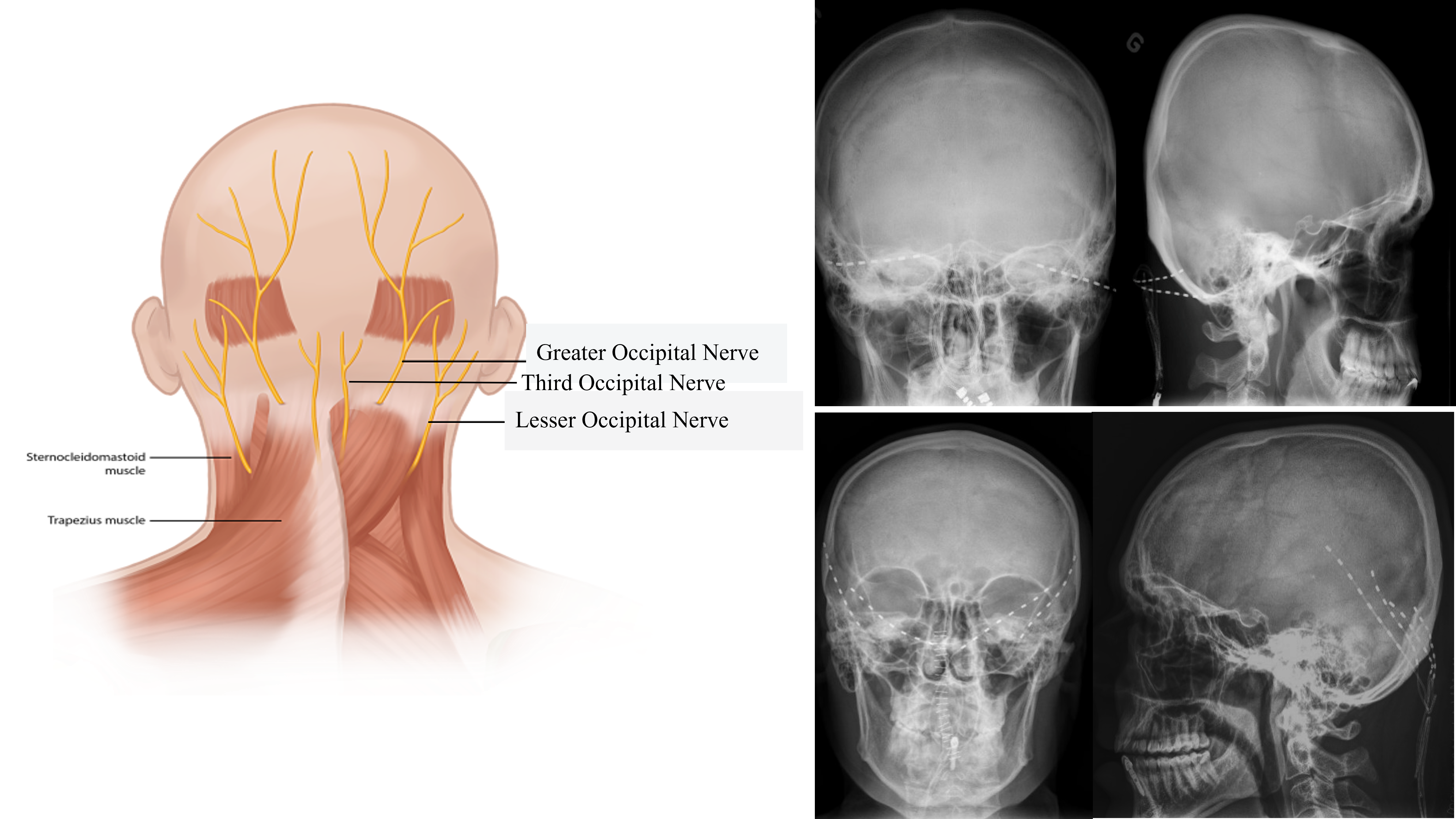
Results
Forty-five patients (mean age: 53.7 years) underwent ONS implantation. Conditions included occipital Arnold’s neuralgia (n=17), migraines (n=11), cluster headaches (n=3), cervicogenic pain (n=5) and neuropathic and mixed craniofacial pain syndromes (n=9). At the last follow-up (mean follow-up time: 4.72 ± 1.02 years), NPRS scores decreased significantly by 3.8 ± 1.7 points, and BPI scores reduced by 45% ± 18. SF-36 measures showed a 20% ± 25 improvement in physical functioning and a 30% ± 22 increase in social functioning. Adverse events occurred in 27% of cases, with lead migration (14%), breakage (8%), and IPG-related issues (6%) being the most common. Surgical re-interventions were required in 14% of patients, predominantly to address hardware-related complications.
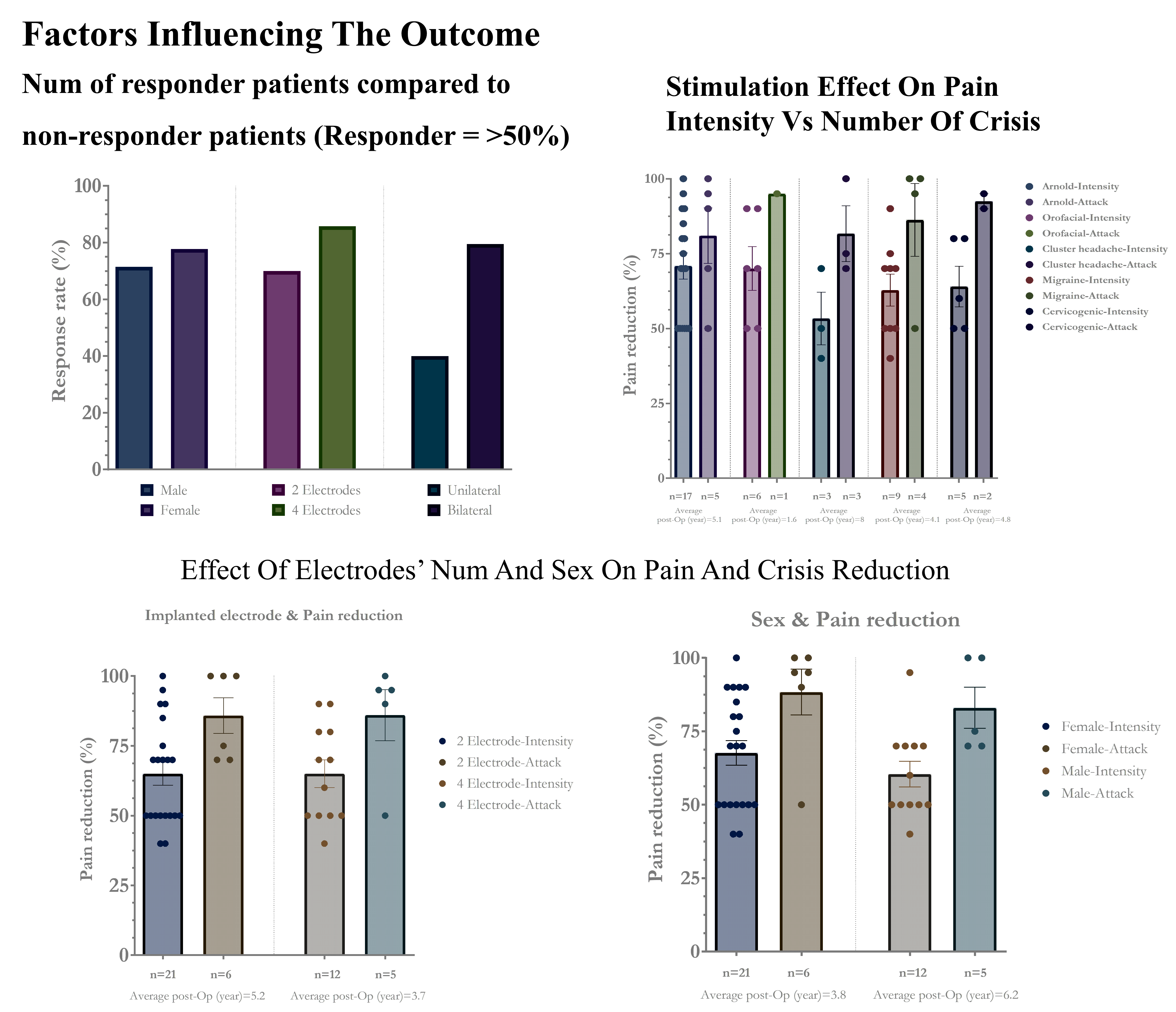
Discussion and conclusion
ONS demonstrated notable efficacy in reducing pain and enhancing quality of life, particularly in patients with occipital Arnold’s neuralgia and cluster headaches. However, the patients with neuropathic component were less responsive for ONS, demonstrating the importance of particularity of its mechanism of pathogenicity. The variability in response among migraine patients highlights the need for personalized approaches. Complications, though frequent, decreased with improved surgical expertise and device refinement. Multidisciplinary preoperative assessment and postoperative adjustments were crucial for optimizing outcomes.
Continued innovation in device technology, patient selection, surgical techniques and programming are essential to maximize therapeutic success while minimizing complications. These findings support the integration of ONS into multimodal pain management strategies for carefully selected patients.
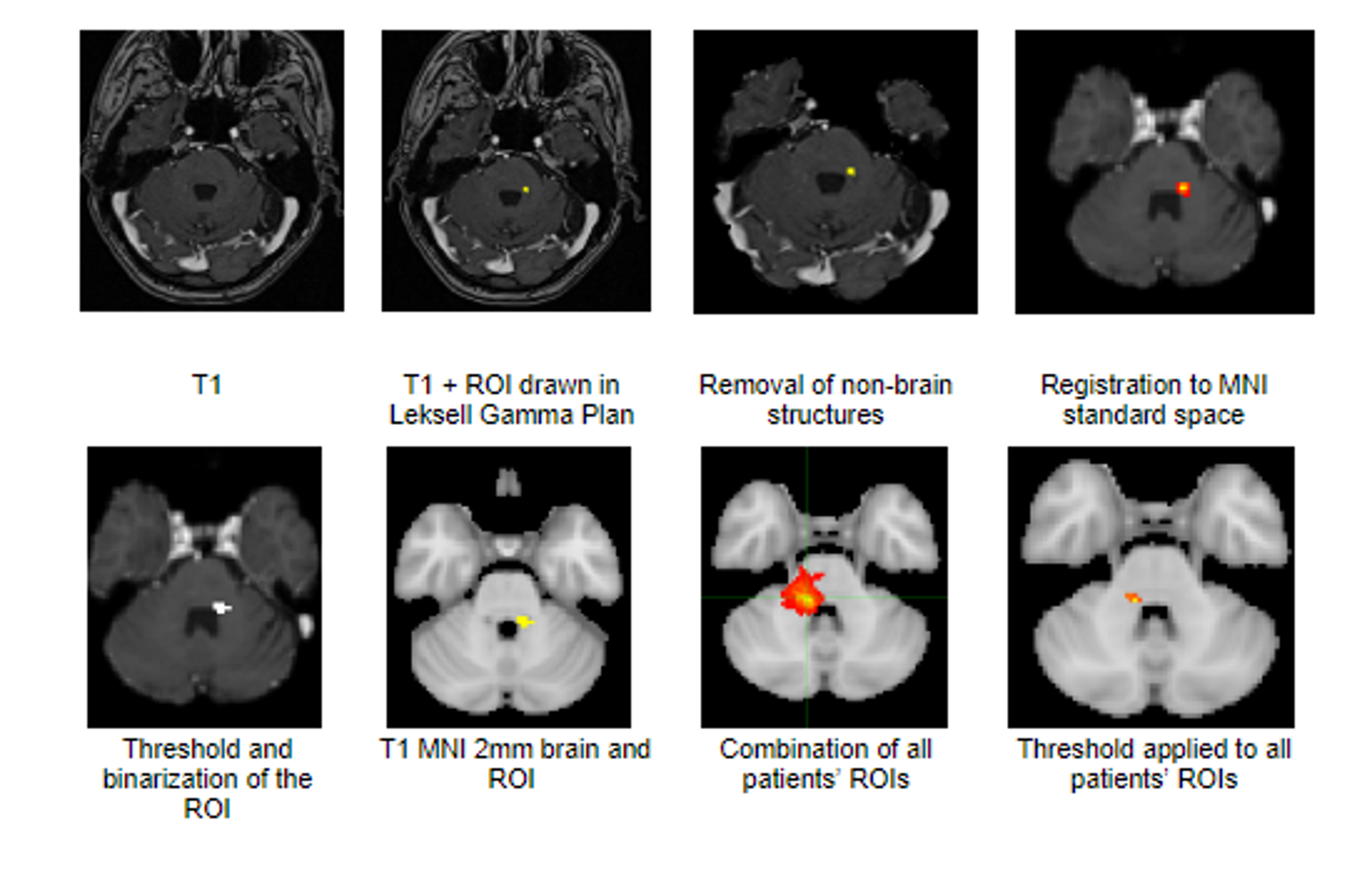
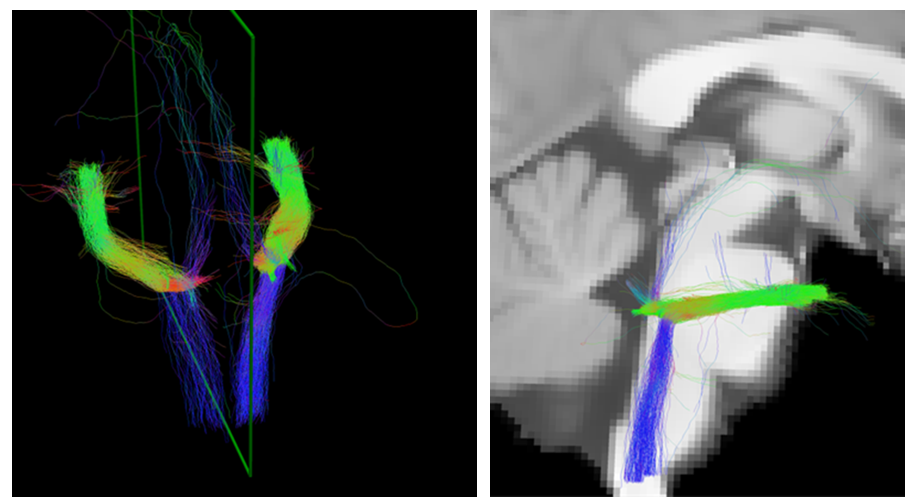
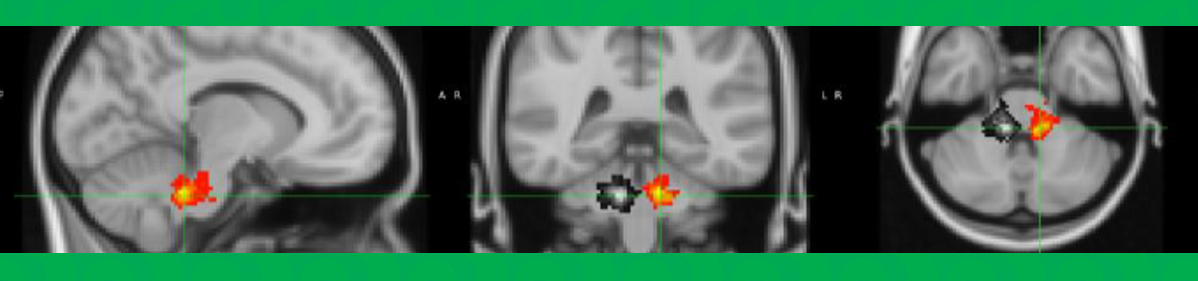
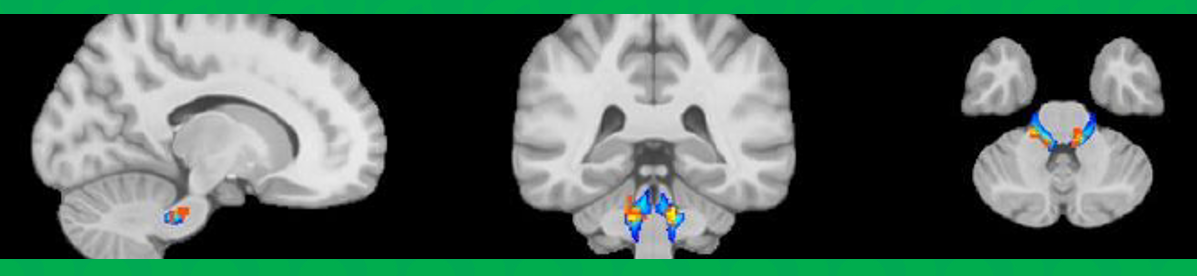
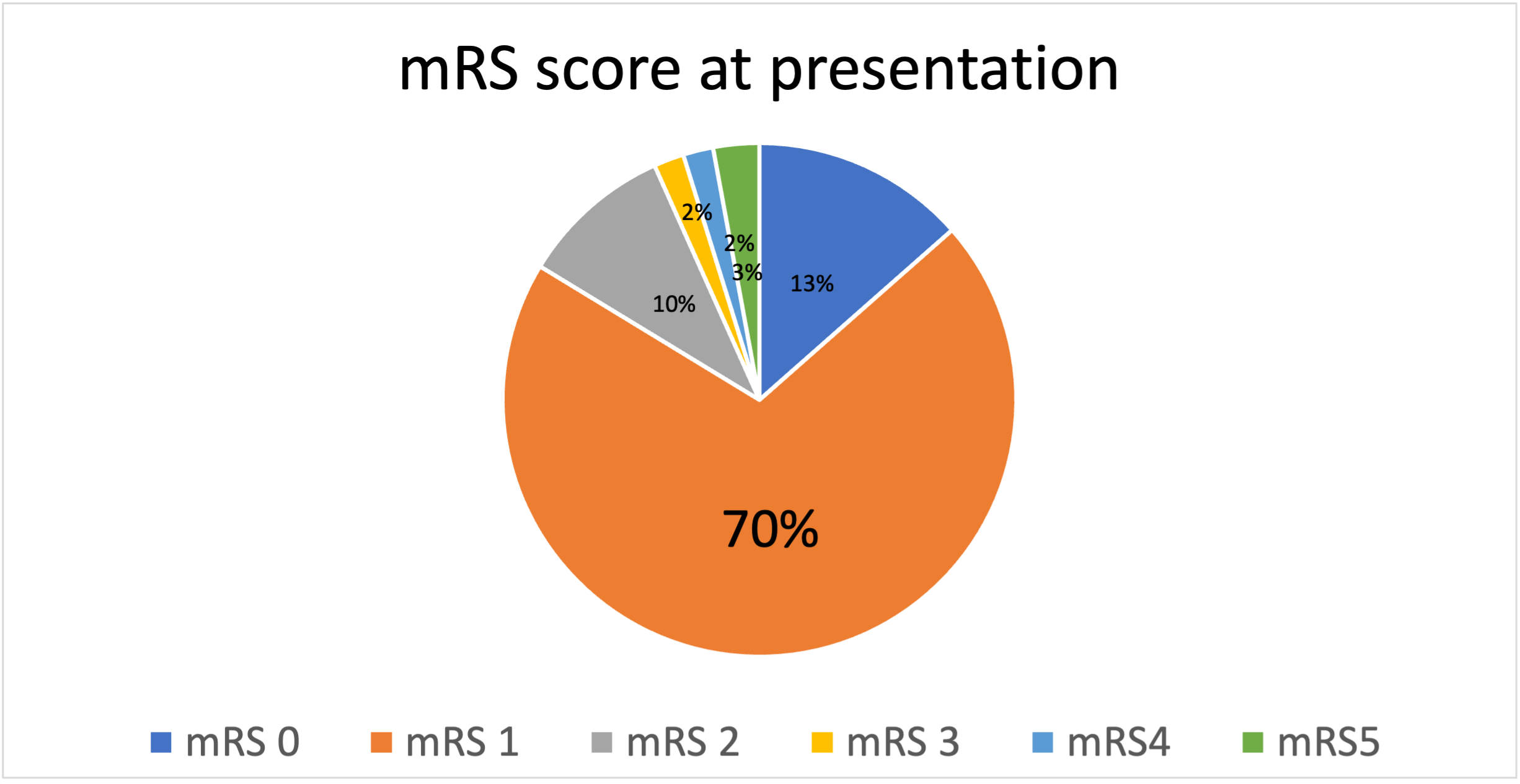
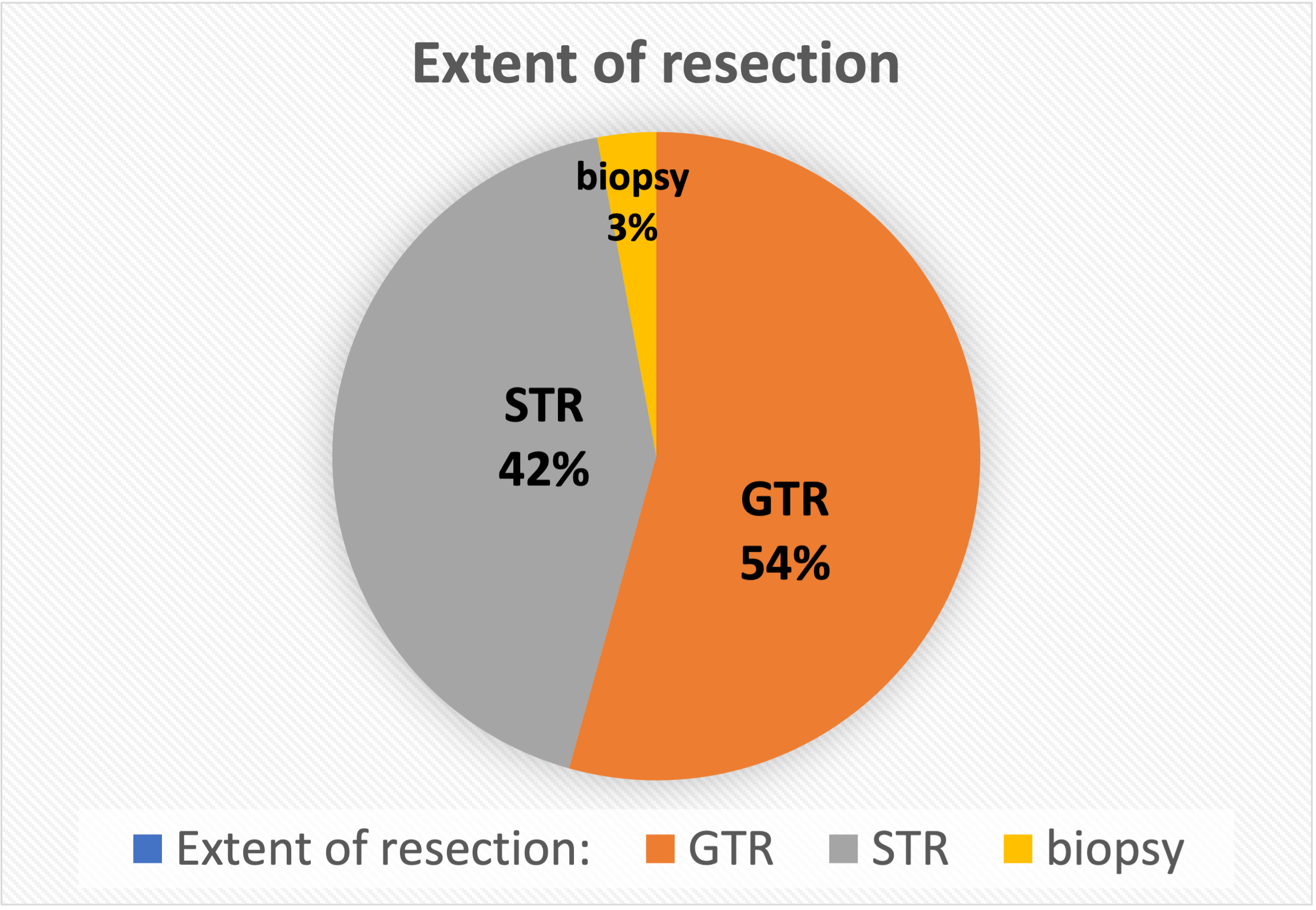
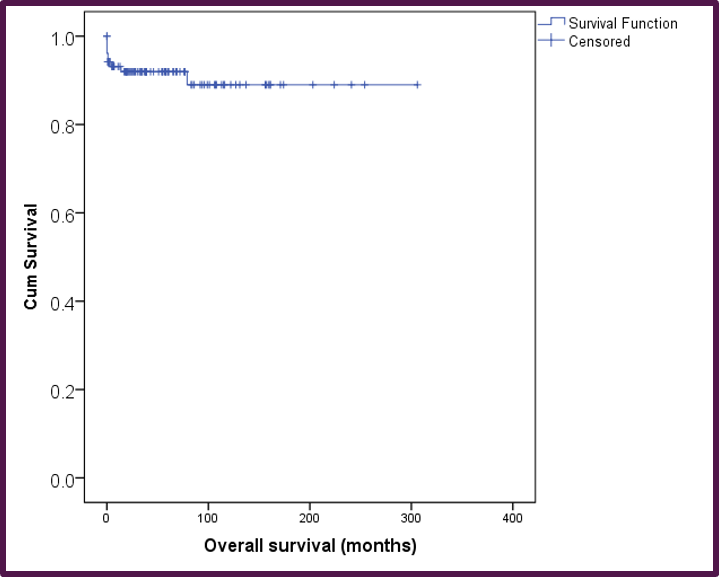
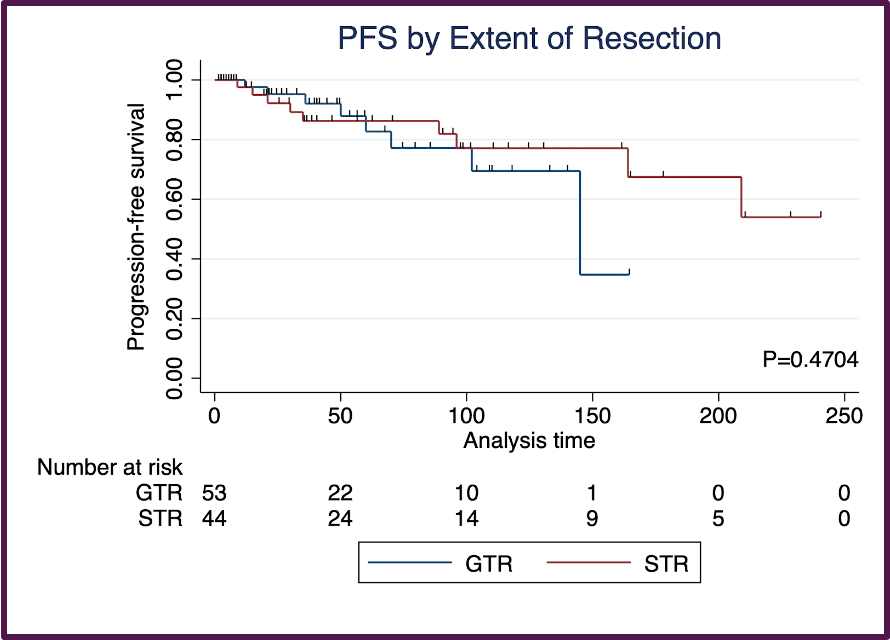
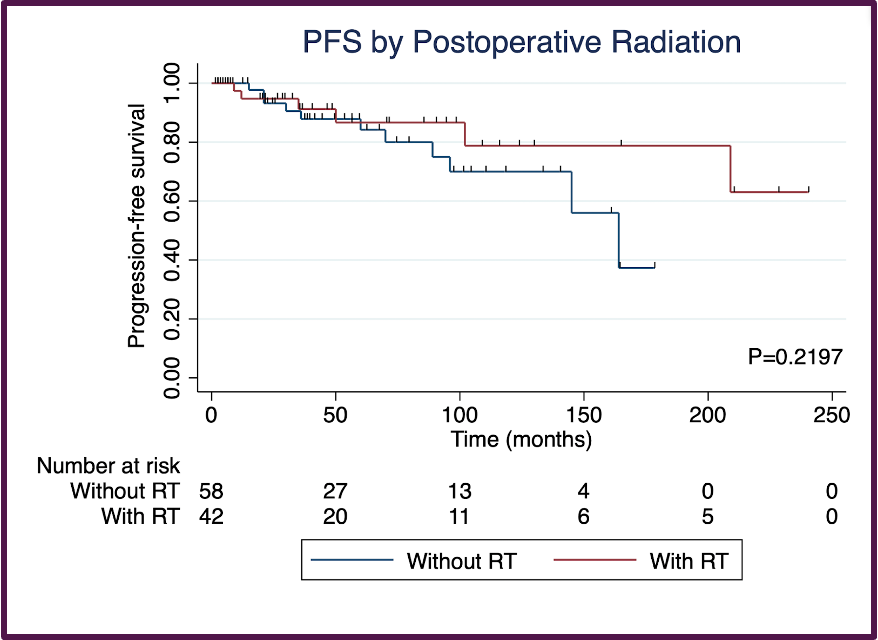
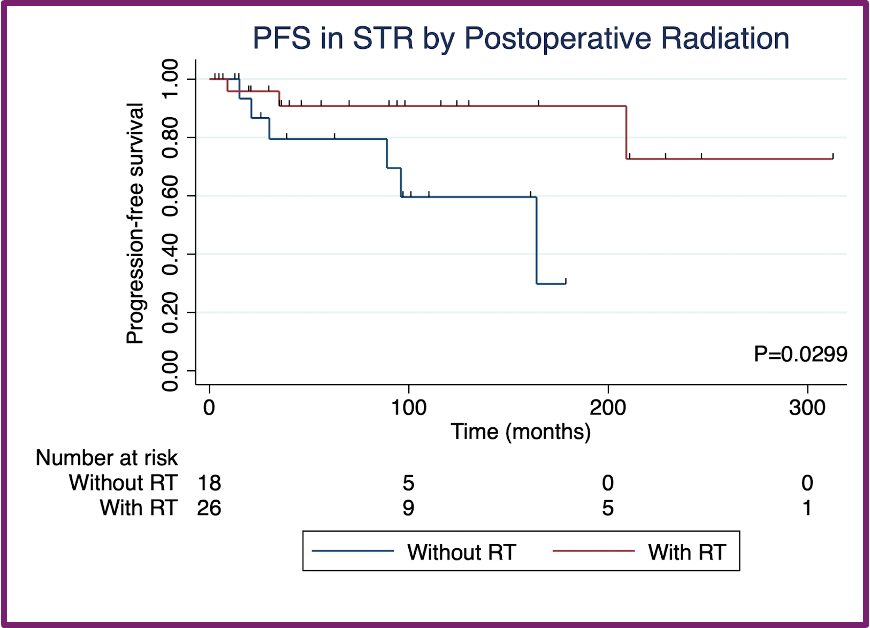
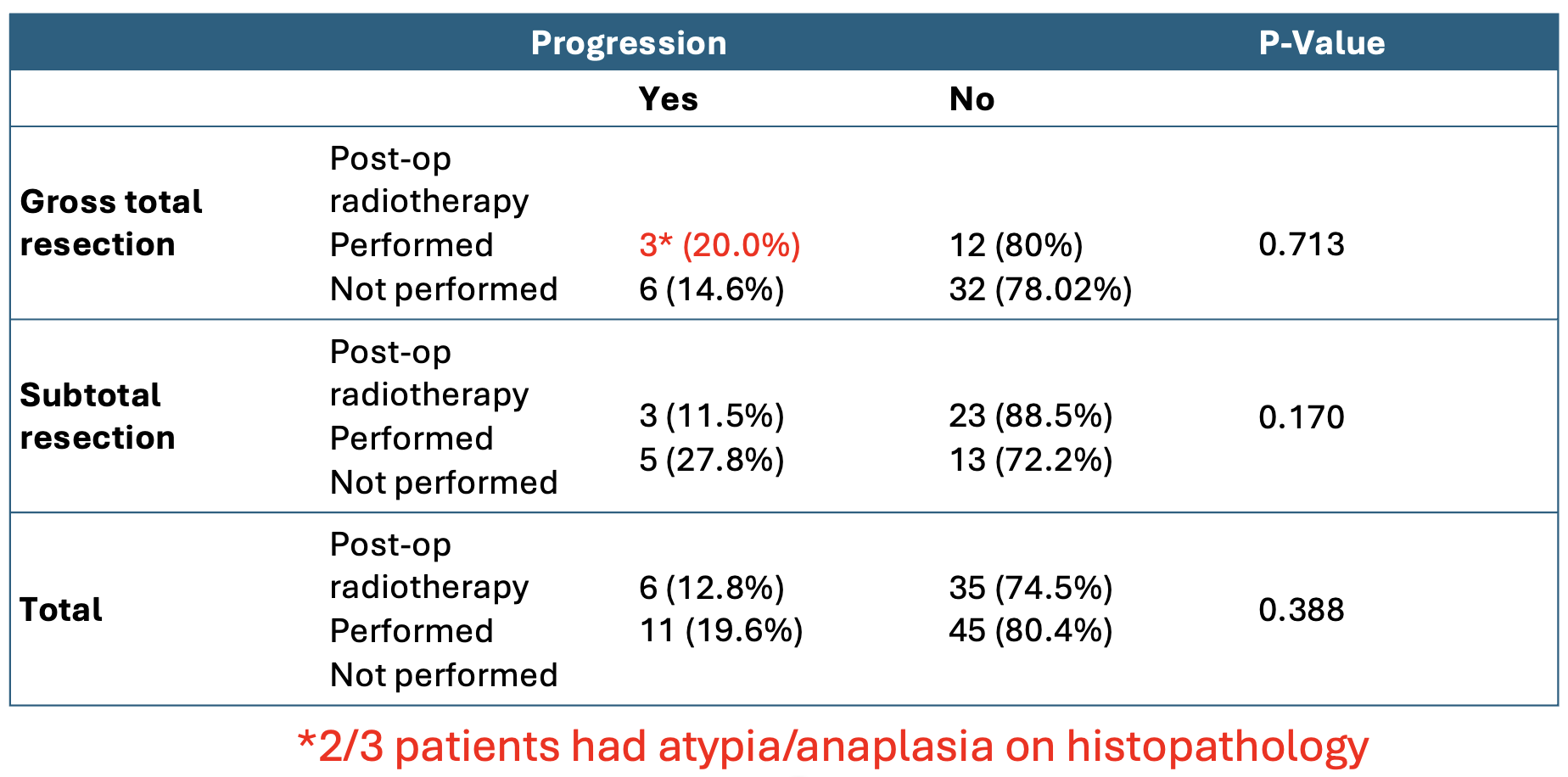
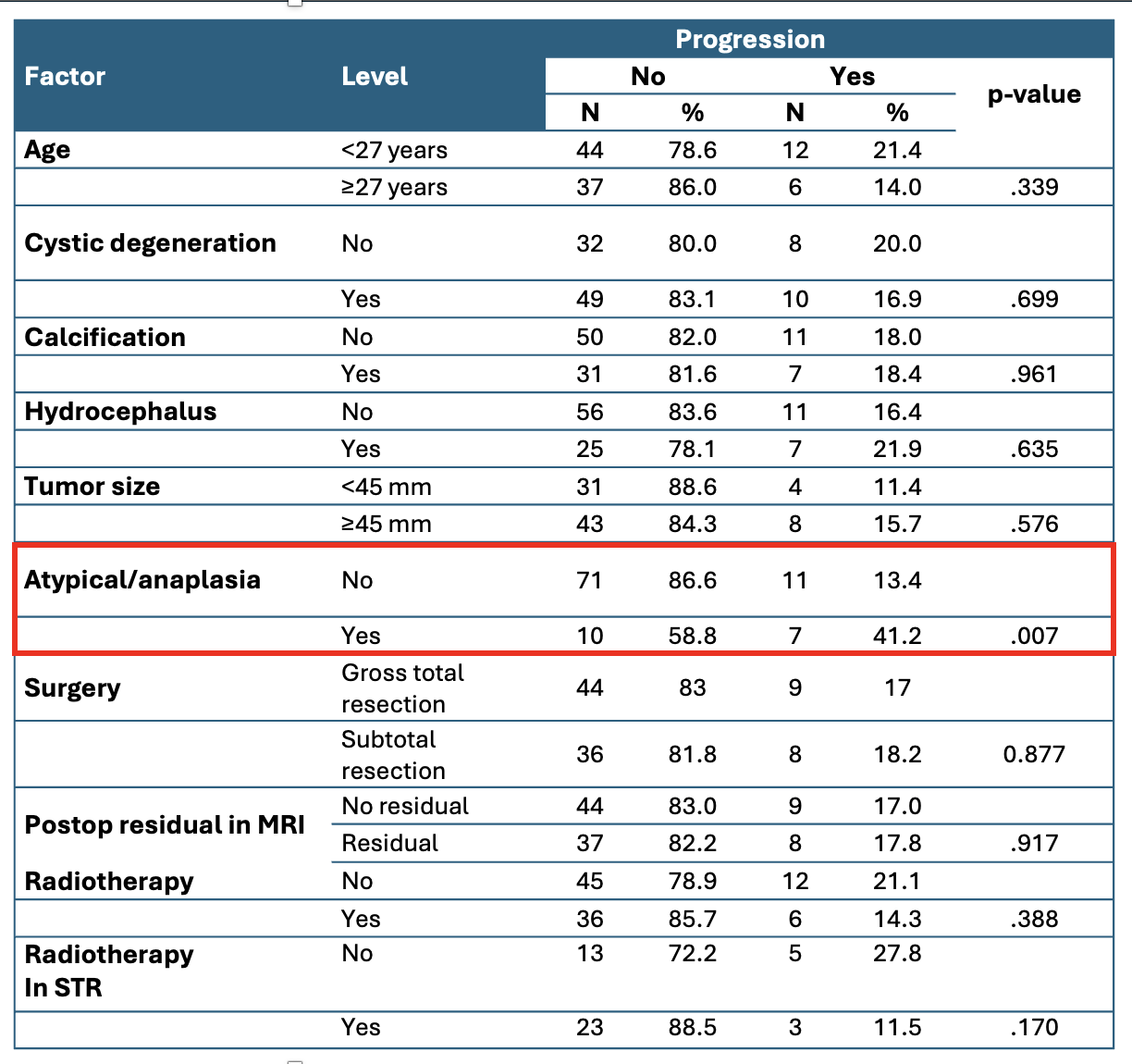
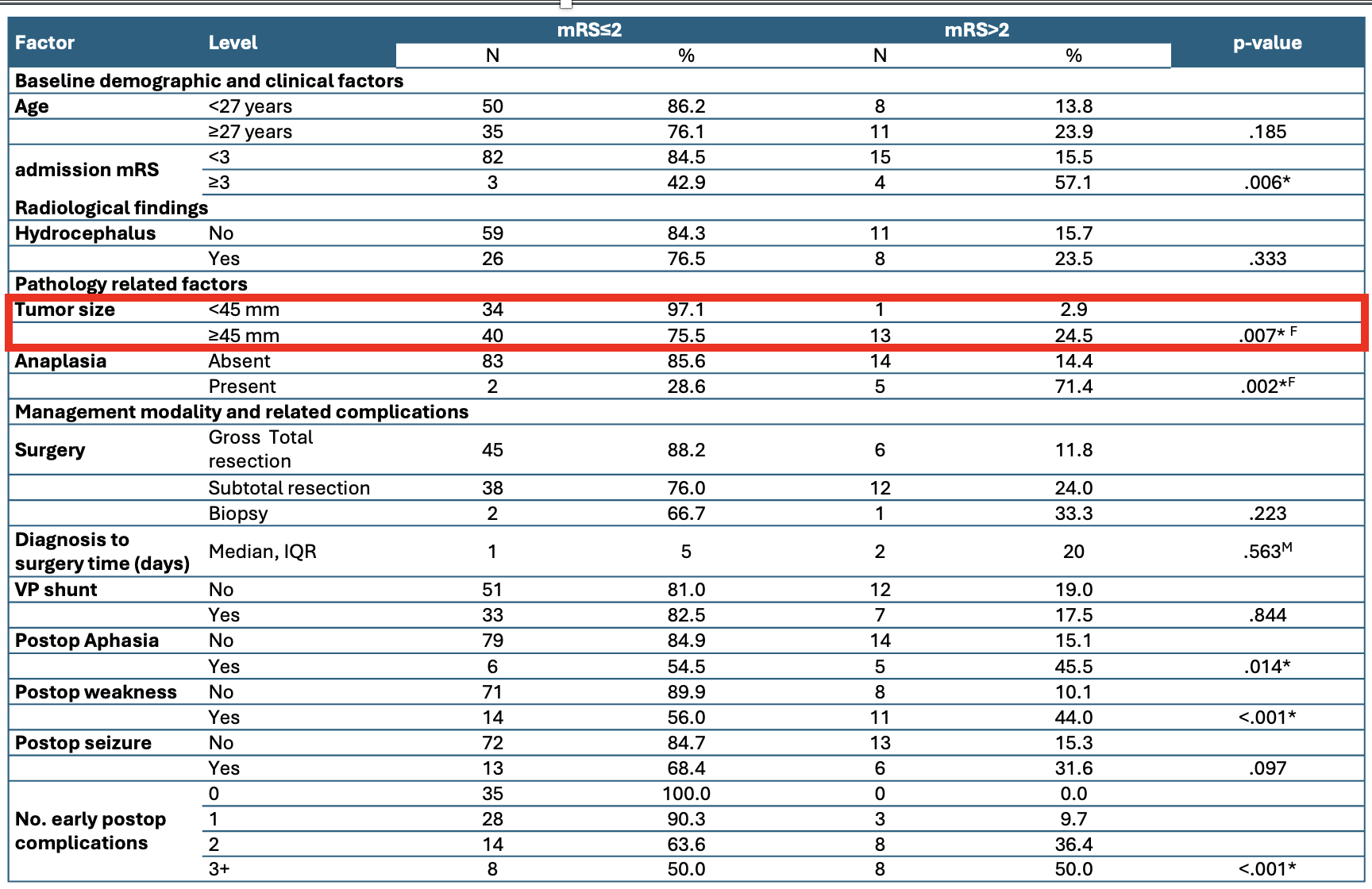

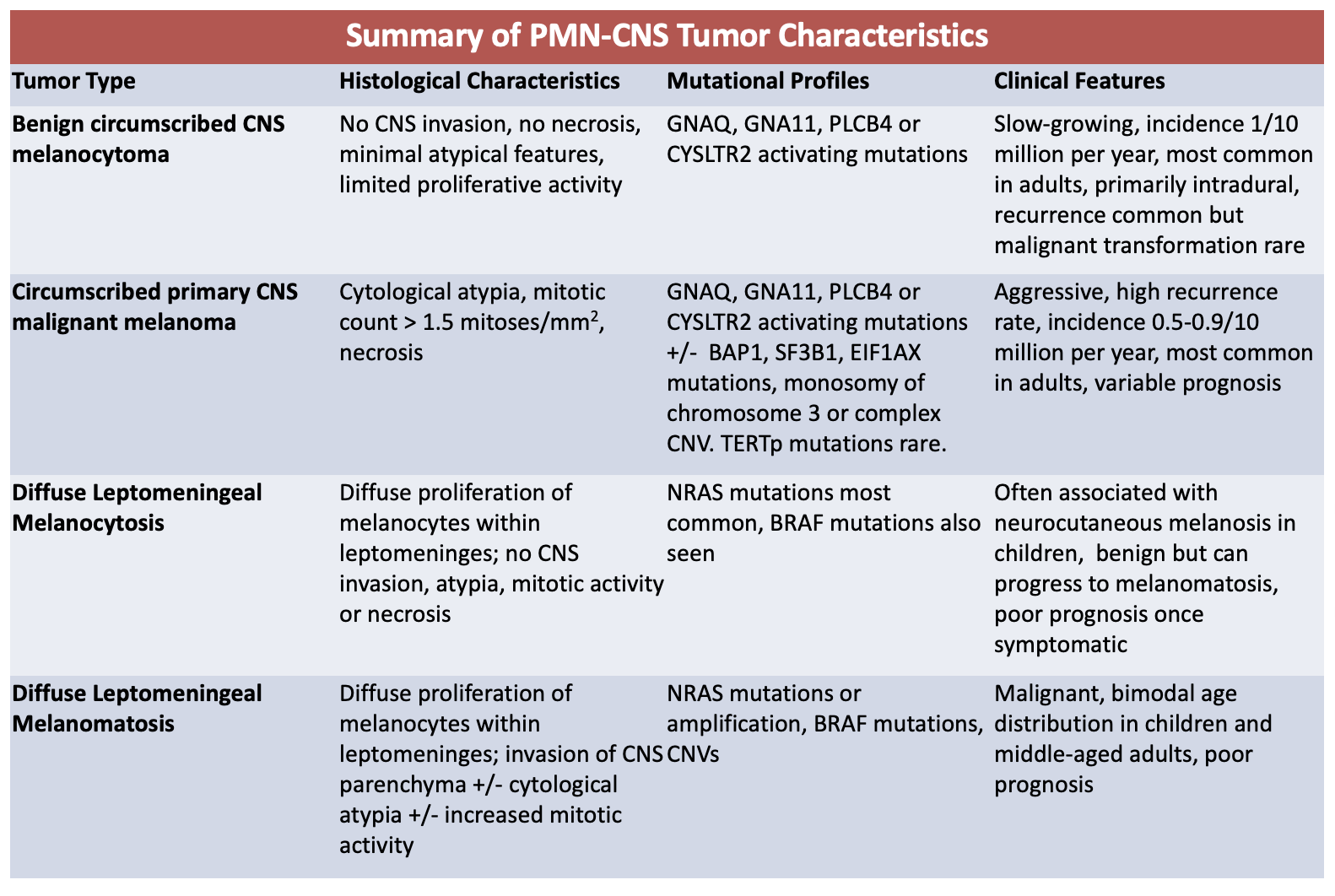
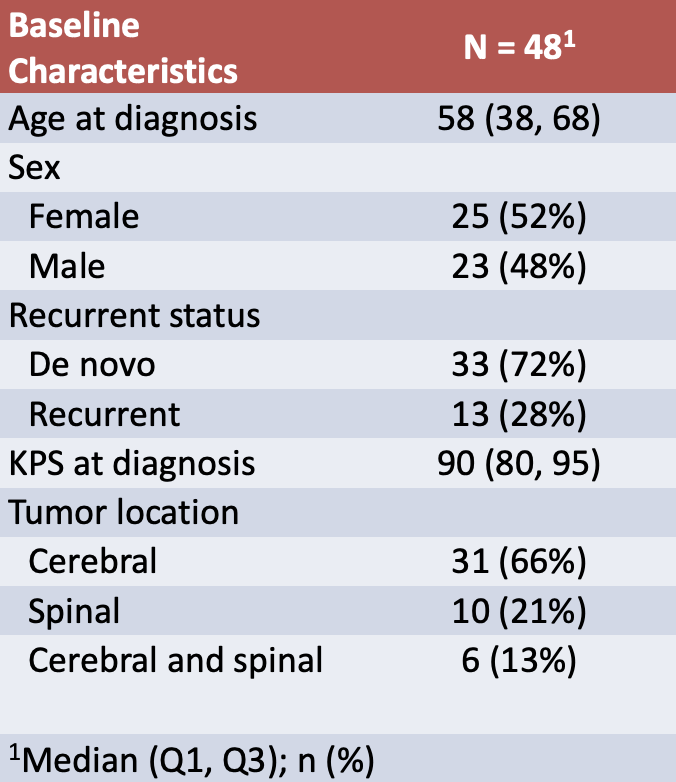
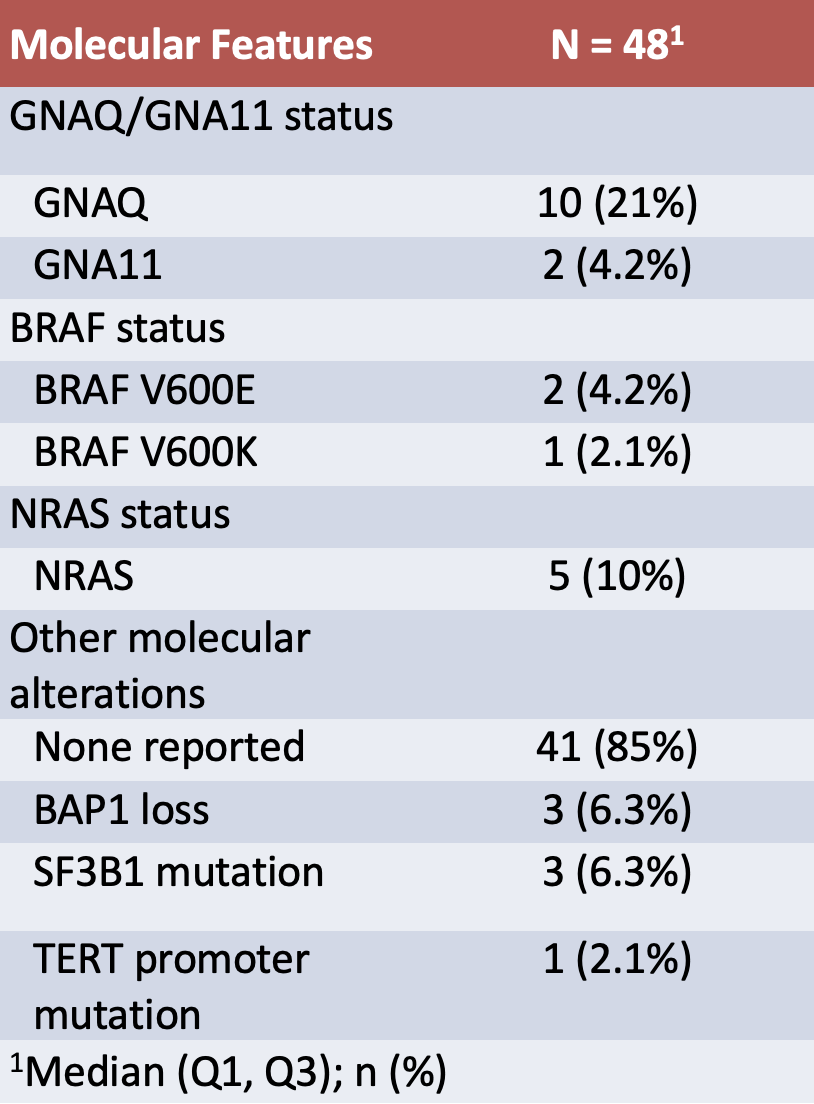
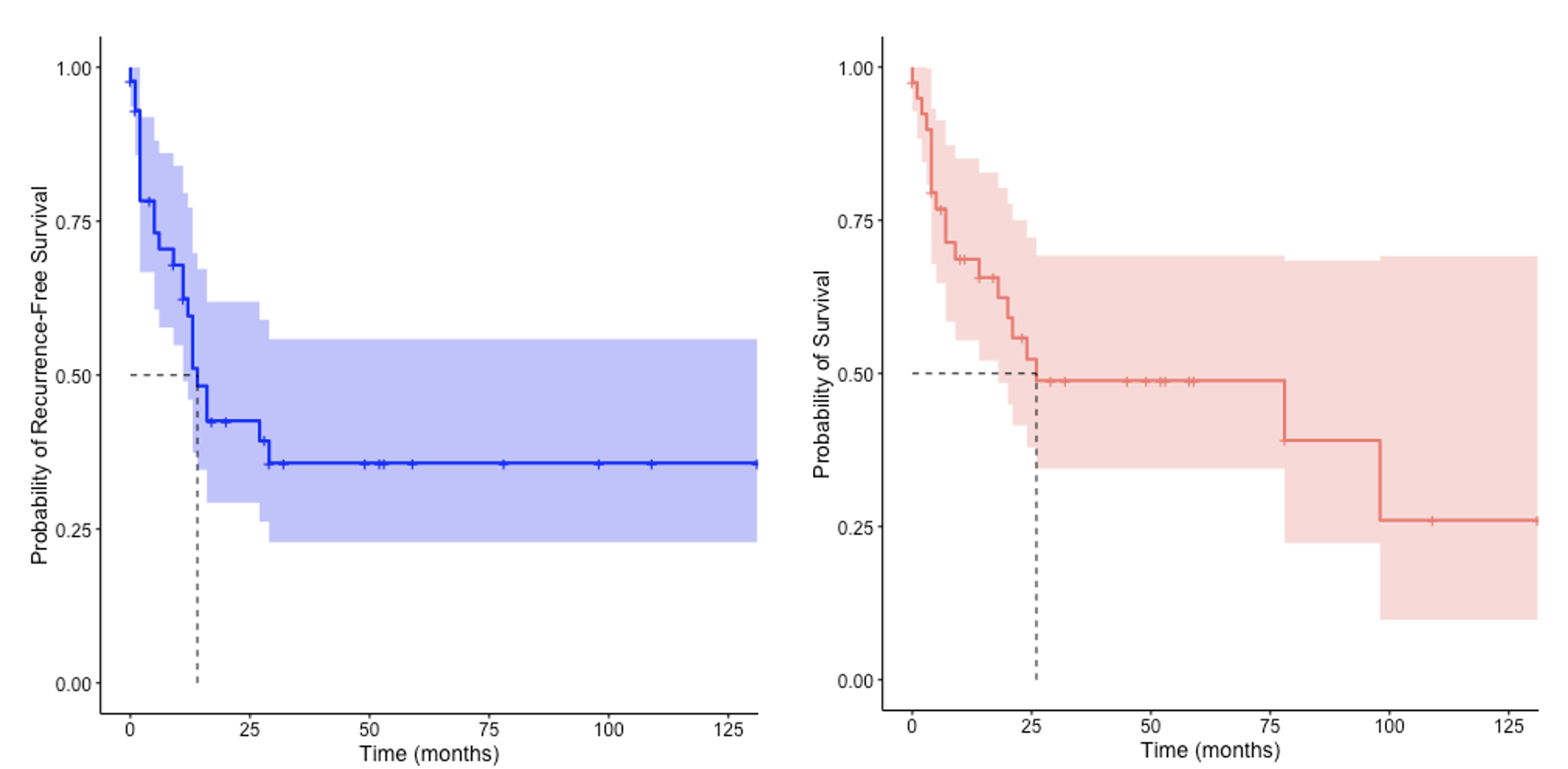


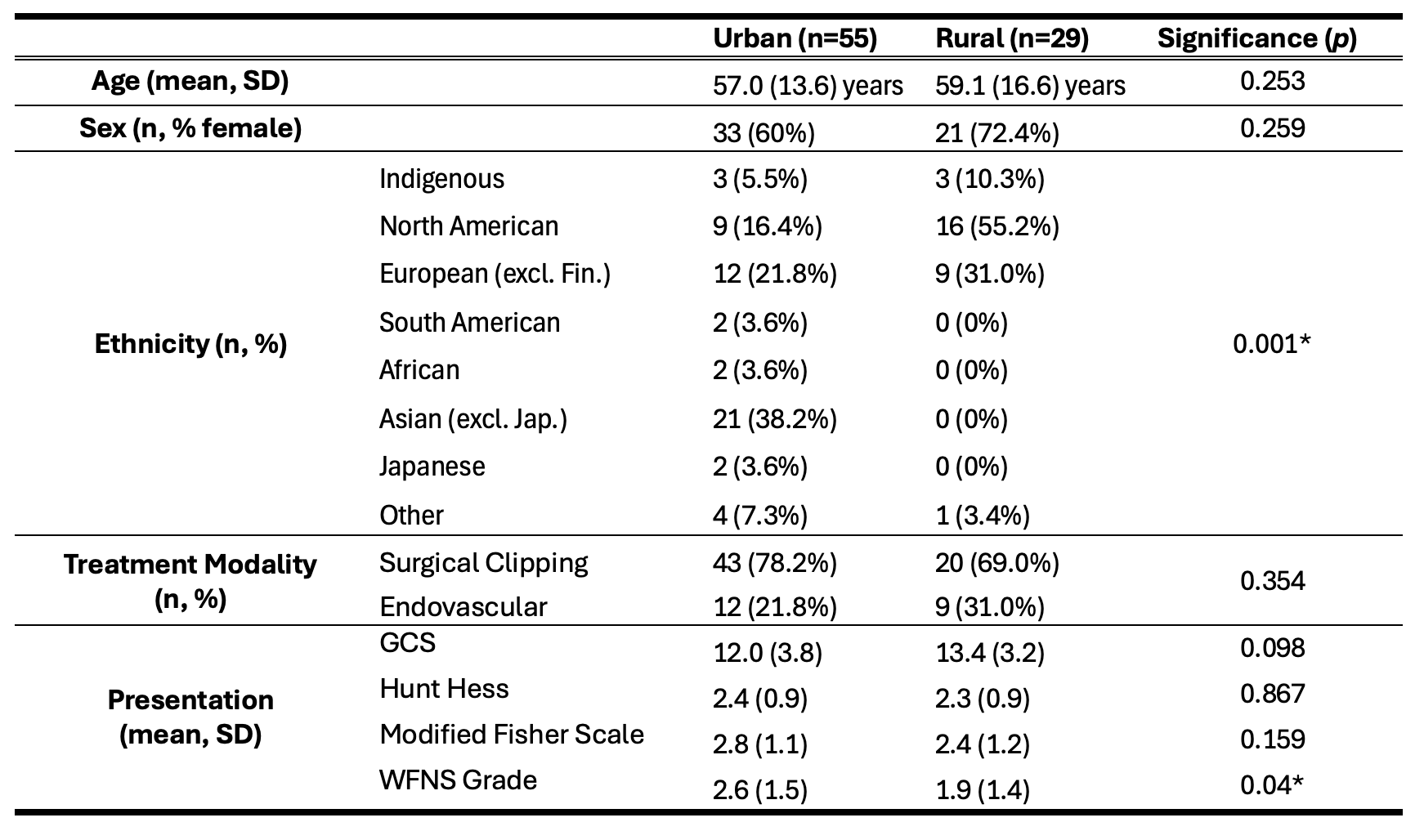
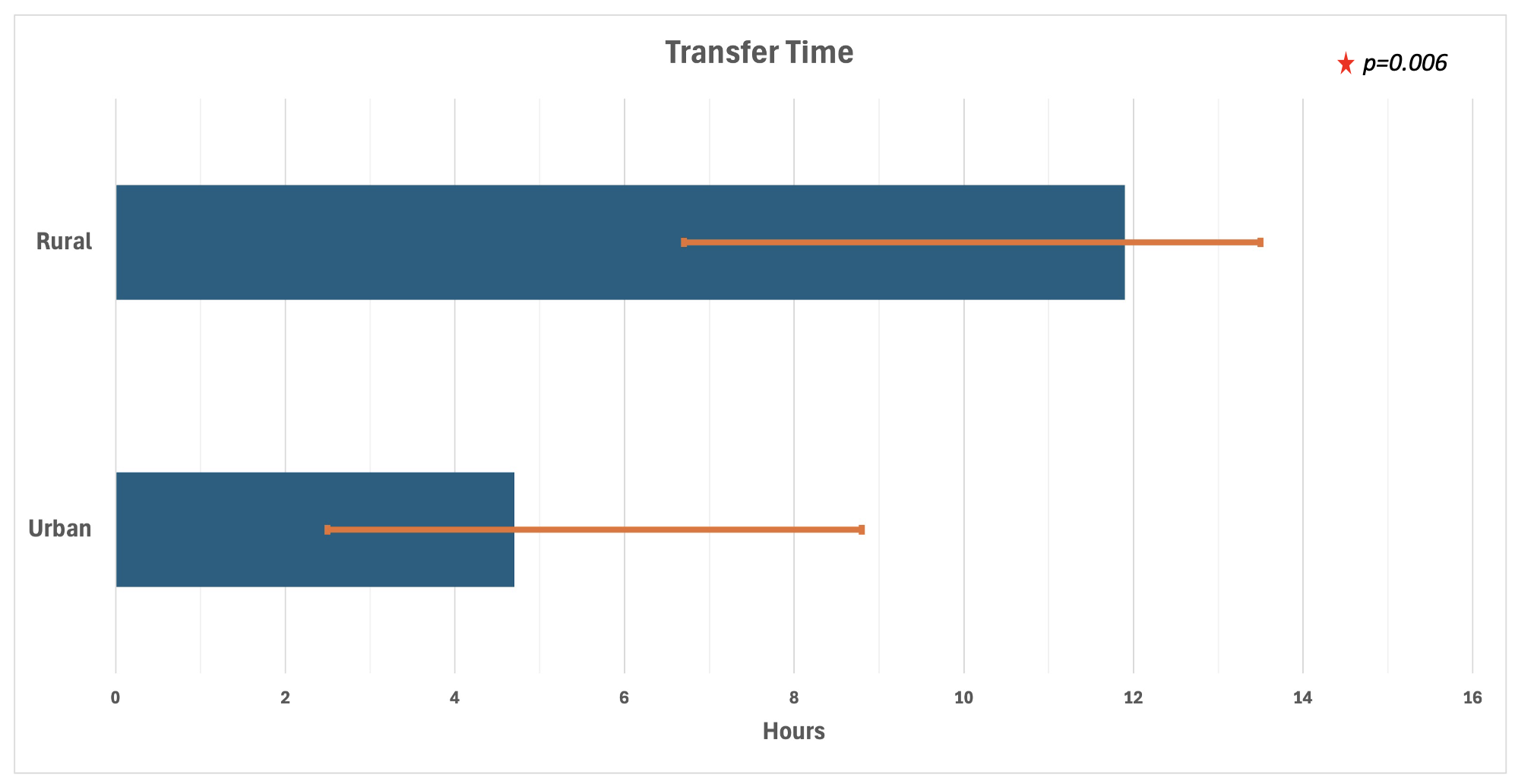
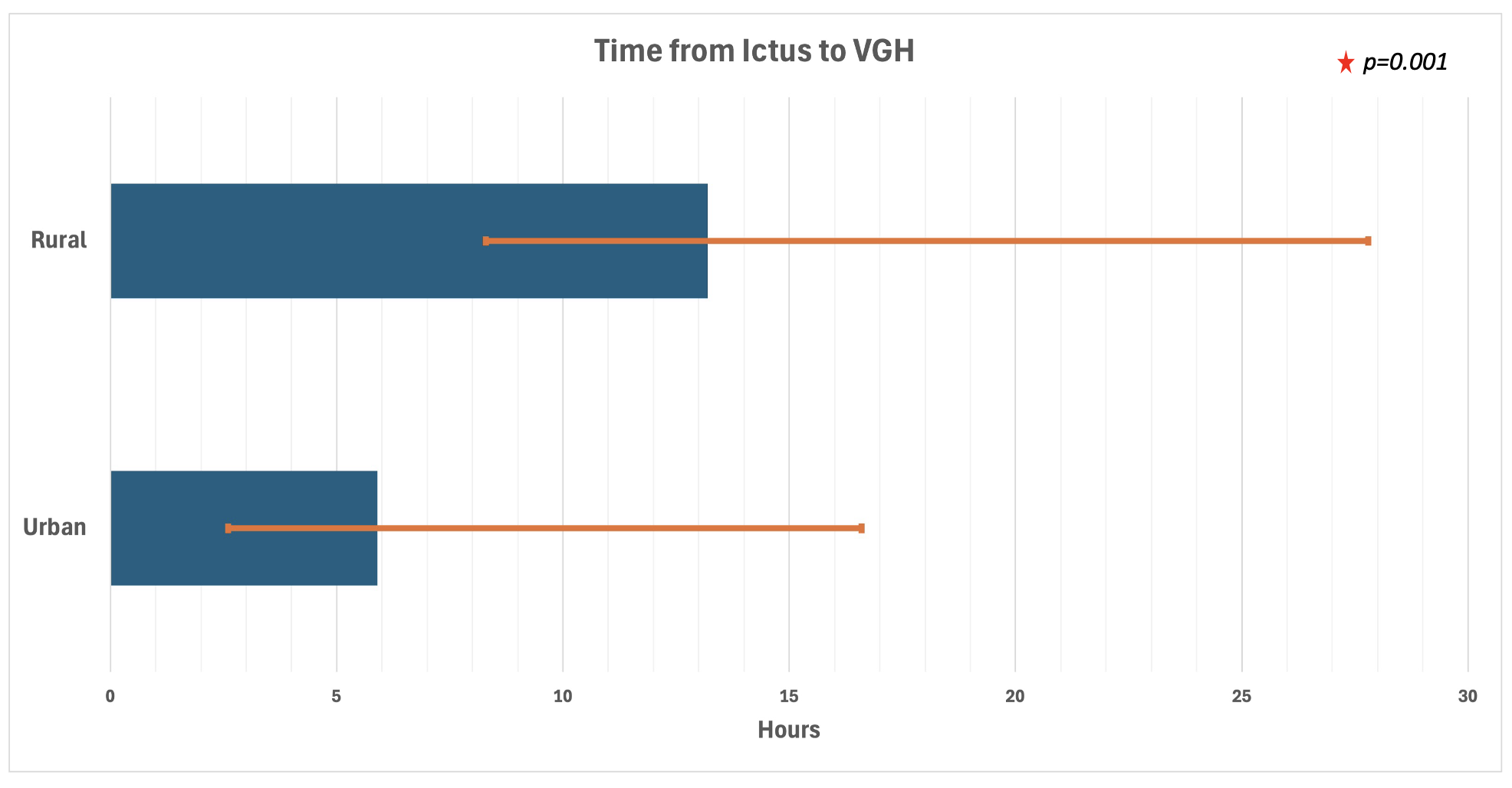
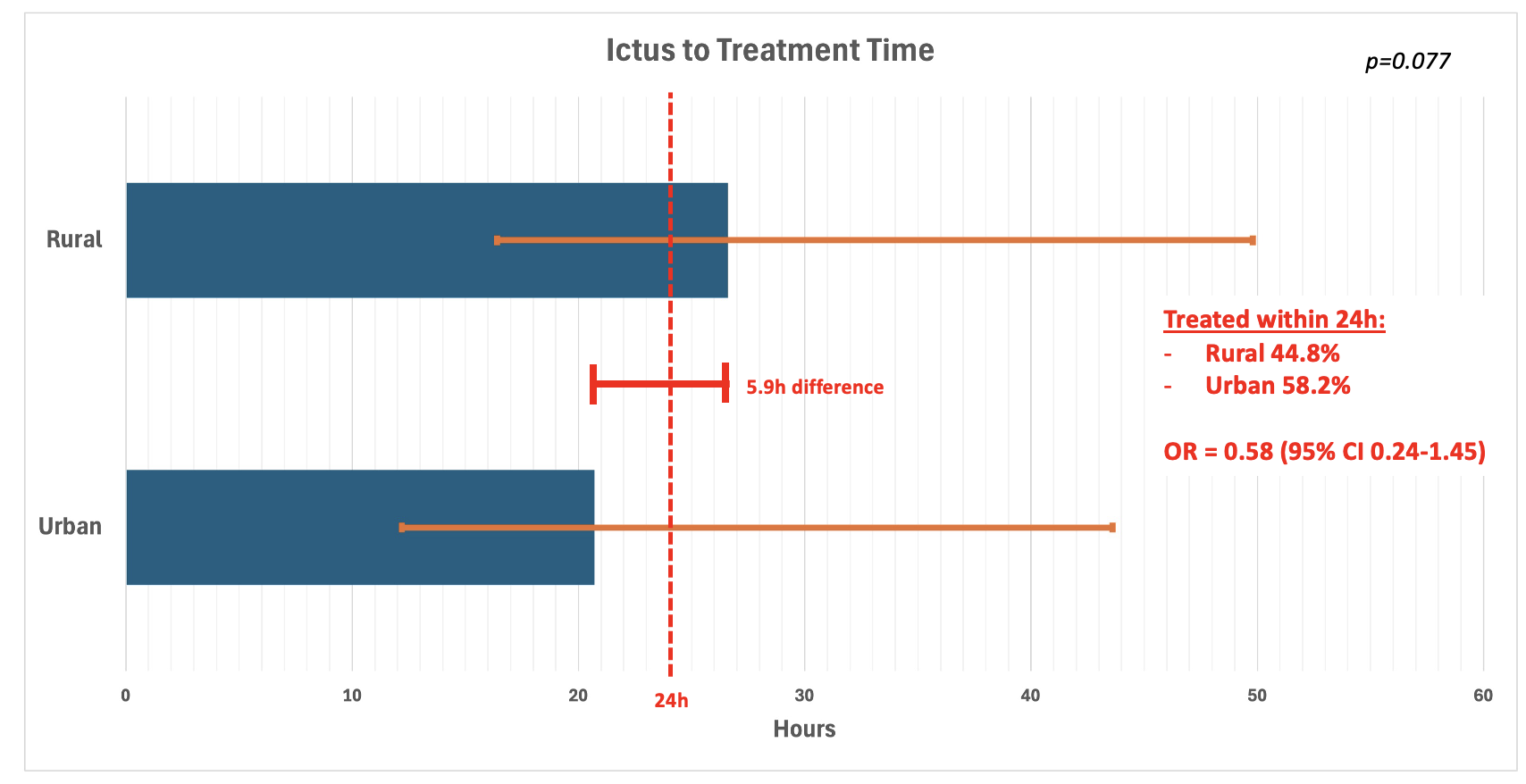
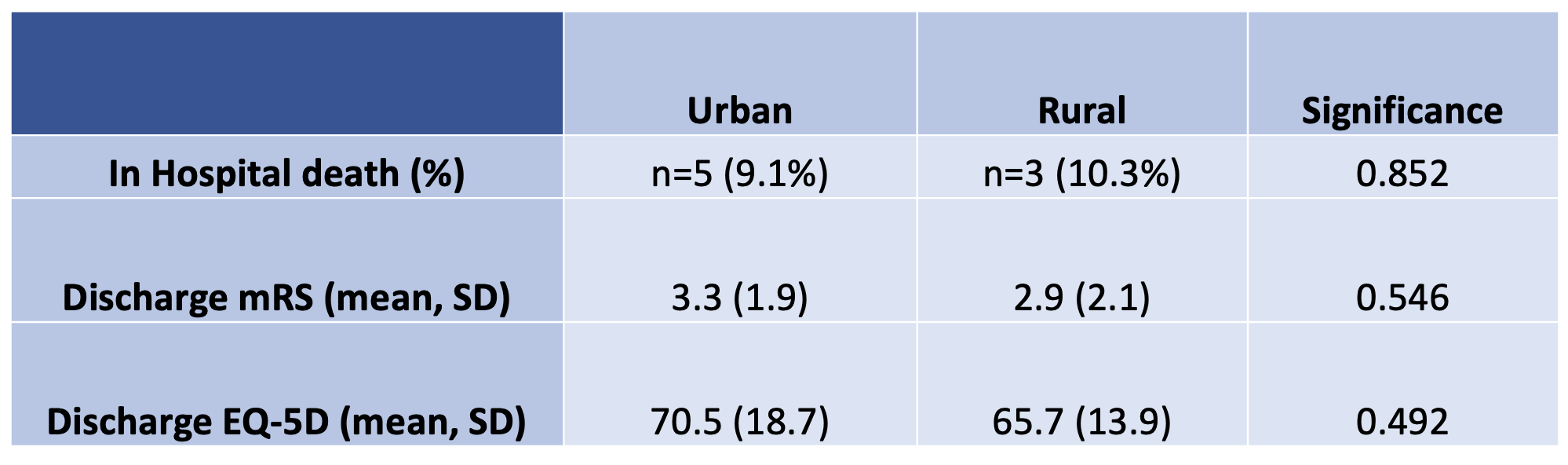

Pituitary neuroendocrine tumors (PitNETs) arise from the anterior pituitary gland and affect between 77 and 116 individuals per 100,0001-3. The endoscopic endonasal approach is now the preferred surgical technique due to its minimally invasive nature and favorable outcomes.
However, this approach carries a risk of new permanent postoperative pituitary deficiencies, occurring in 4–10% of cases4-6. Accurate intraoperative identification of the pituitary gland is crucial: when the gland is not correctly visualized, 46–67% of patients experience hormonal insufficiency7-8, compared to only 3.5% when it is successfully identified7. These findings underscore the importance of reliable gland localization during surgery to reduce endocrinologic complications.
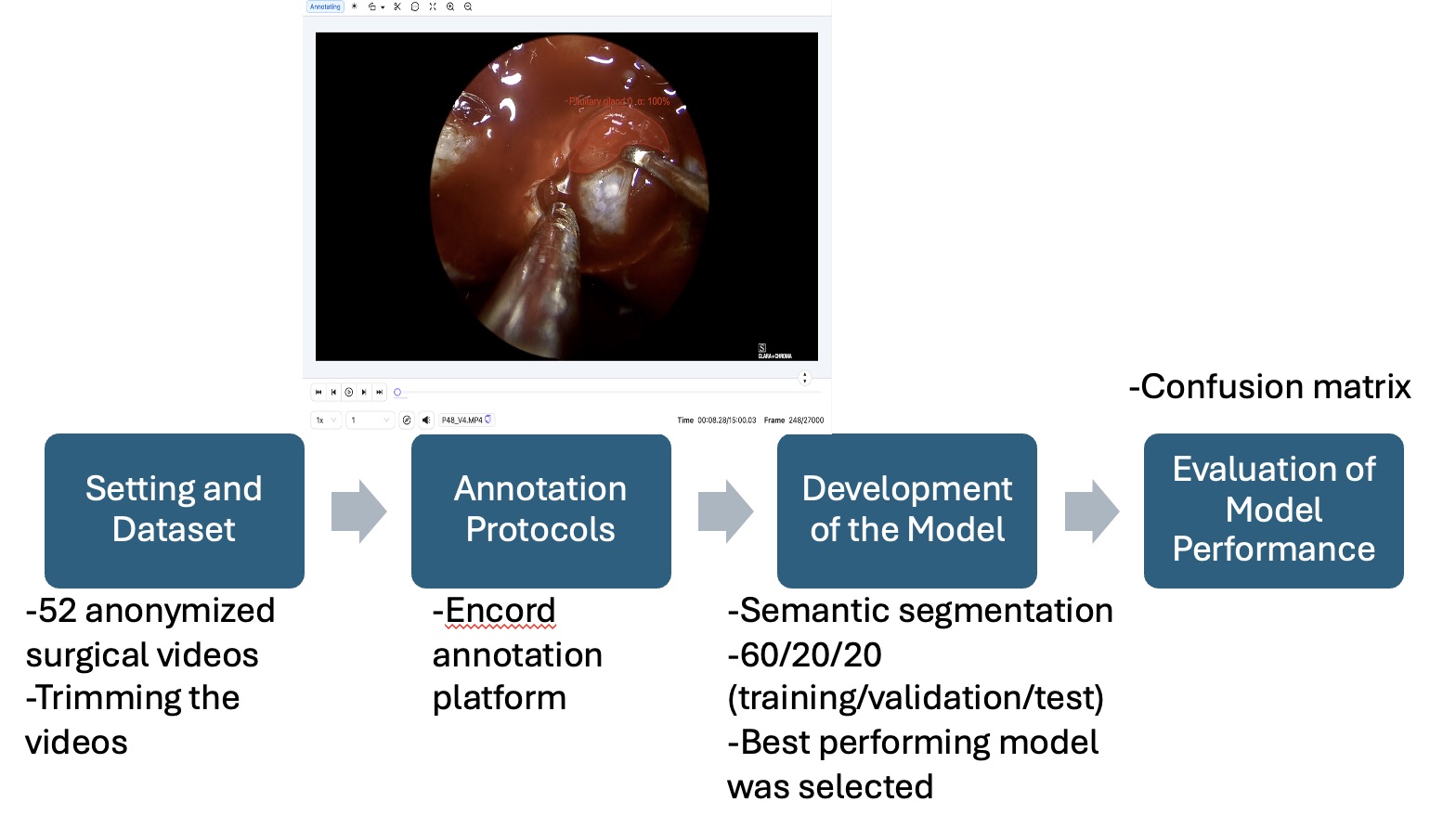
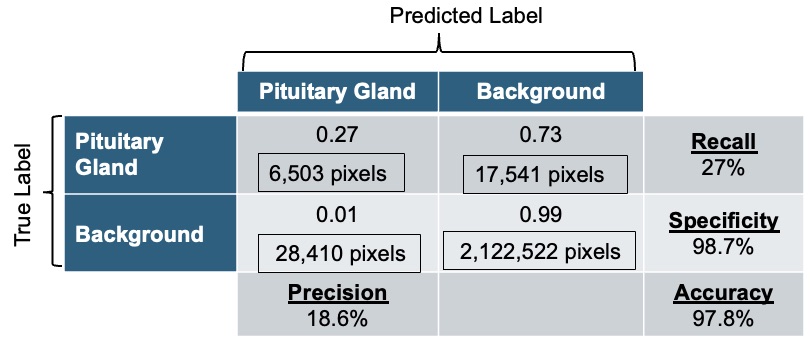
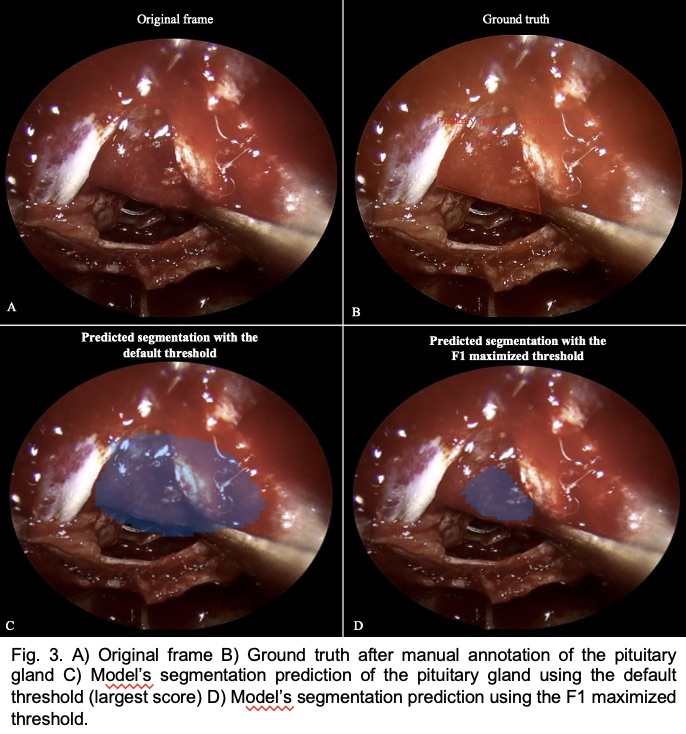
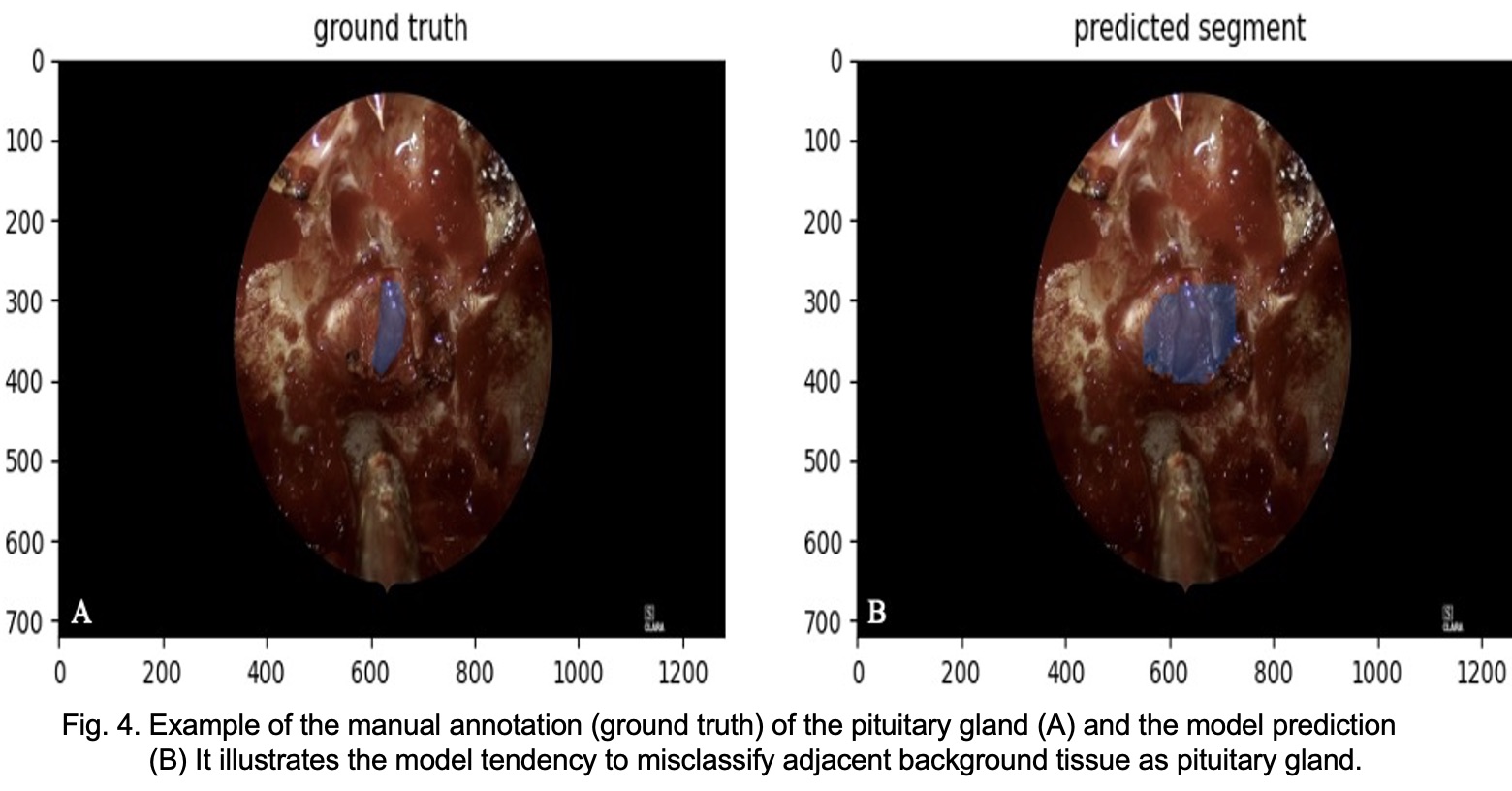
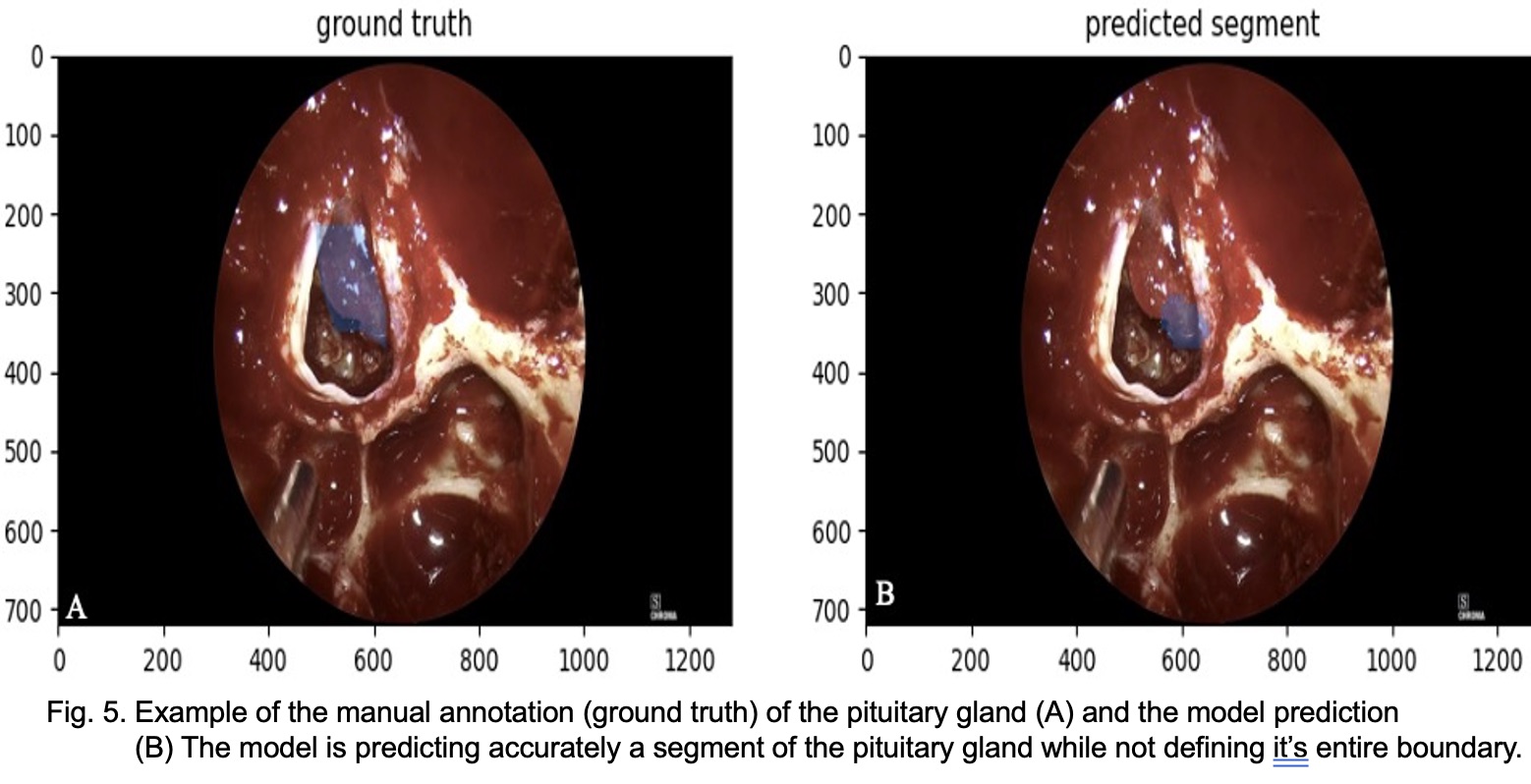
Canadian neurosurgery residency programs have an alarming 28.4% attrition rate—seven times higher than the average for most other specialties (1–4%)1-4 and double that of US neurosurgery programs5-6. Canadian data for this issue is over 30 years old7, highlighting the need for updated research. This study identifies factors contributing to Canadian neurosurgery attrition rates.
Data from 8 of 14 programs showed an average attrition rate of 14.1% (range: 0%–28.6%).
Interviews with 7 program directors and 7 former residents (from 7 programs) identified key factors contributing to attrition, listed in descending order of frequency mentioned during interviews:
High workload
Poor work-life balance
Gender-related challenges for women
Evolving aspirations over time
Limited job opportunities in Canada
High responsibility level
High workload:
Neurosurgery residents experience a high workload due in part to a hidden curriculum that discourages leaving after call, creating pressure to prove commitment. This intense environment, combined with staffing shortages and a strong sense of responsibility toward patient care and co-residents, often prioritizes service needs over residents’ own education.
Poor work-life balance:
Residents struggled to achieve a satisfying work-life balance, largely due to the high workload. Seeing their attending physicians face the same difficulties made them realize they were likely to encounter similar struggles in the future—highlighting a lifestyle and career path that felt misaligned with their personal values.
Gender-related challenges for women:
Some challenges were specific to women, particularly related to pregnancy, raising children, and navigating an environment that remains predominantly male-dominated.

Meningiomas exhibit considerable clinical and biological heterogeneity. We previously identified four distinct molecular groups (immunogenic, NF2-wildtype, hypermetabolic, proliferative) that address much of this heterogeneity. Despite the utility of these groups, the stochasticity of clustering methods and the use of multi-omics data for their discovery limits the potential for classifying prospective cases. We sought to address this by constructing a dedicated DNA methylation-based classifier.
Using an international cohort of 1698 meningiomas, we constructed and rigorously validated a machine learning-based molecular classifier using only DNA methylation data as input (Figure 1). Original and newly-predicted molecular groups were compared using DNA methylation, RNA sequencing, copy number profiles, whole exome sequencing, and clinical outcomes.
Figure 2. Our classifier faithfully recreates the biology of ground-truth molecular groups based on orthogonal molecular platforms which were not used in model training. A: Comparison of group-specific inferred CNAs between training (discovery) cohort and predicted MGs on the validation cohort. B: Comparison of somatic NF2 and known canonical non-NF2 meningioma mutations by actual and predicted MG. C: Relative expression of MG-specific RNA signatures, developed on the discovery cohort, on the validation cohort. D: Inferred cell-type proportions in both cohorts based on bulk RNA deconvolution.
Figure 3. Our classifier faithfully recreates the clinical outcomes of ground-truth molecular groups. Kaplan Meier curves comparing MG-specific PFS in the validation cohort (left) and discovery cohort (right) demonstrates remarkable concordance in clinical outcomes. Notably, outcomes were not used in the original MG discovery nor the current model.
We show that group-specific biology of the validation cohort is nearly identical to that of the original discovery cohort (Figure 2). Specifically, the distribution of group specific CNAs (1p loss, 1q gain, 22q loss) and somatic mutations (NF2 and established non-NF2 driver mutations) are nearly identify between cohorts and tumours classified as NF2 wildtype indeed had no NF2 mutations in the validation cohort. RNA pathway analysis revealed expected upregulation of immune-related pathways in the immunogenic group, metabolic pathways in the hypermetabolic group and cell-cycle programs in the proliferative group. Bulk deconvolution similarly revealed enrichment of macrophages in immunogenic tumours and neoplastic cells in hypermetabolic and proliferative tumours with similar proportions to those originally described. Finally, clinical outcomes in the validation cohort are nearly identical to those originally described, with median PFS of 7.4 (4.9-Inf) years in hypermetabolic tumors and 2.5 (2.3-5.3) years in proliferative tumors (not reached in the other groups, Figure 2). Importantly, these groups were discovered independent of clinical outcomes.
We present a novel meningioma molecular classifier using only DNA-methylation data as input and rigorously demonstrate its validity using a large, multi-centered cohort of 1698 patients including samples from the prospective RTOG-0539 clinical trial. This represents an important step toward increasingly personalized care for patients with meningioma and will help usher in a new era of molecularly-stratified clinical trials.
Meningiomas are the most common intracranial extra-axial lesion. Reports of meningioma regression exist, often in the context of known hormonal or vascular fluctuations, though very few describe complete resolution. Though rare, extra-axial mimics such as lymphoma and chloroma may also spontaneously regress.
A 29-year-old male presenting with new onset seizures was found to have a 22.7 x 26.6 mm left temporal extra-axial lesion, radiologically consistent with meningioma. He was otherwise healthy, and was treated with dexamethasone at initial presentation until an interim CT had confirmed persistence of the tumour’s size 1 month after diagnosis. Due to wait times and patient preference, repeat pre-operative imaging was not available prior to surgical resection 13 months later. Decision was made to proceed with resection; however, intraoperatively, no lesion was identified.
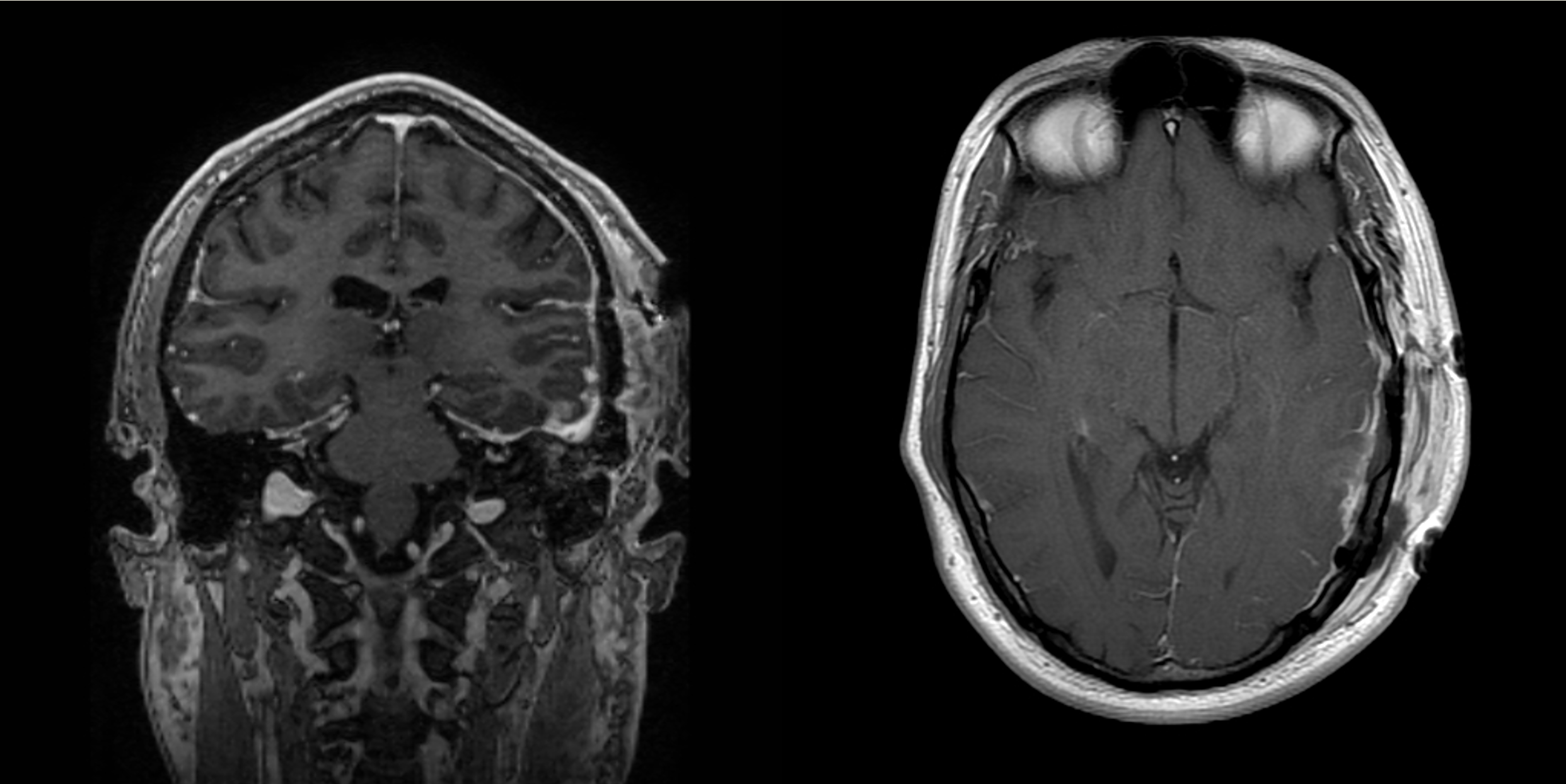
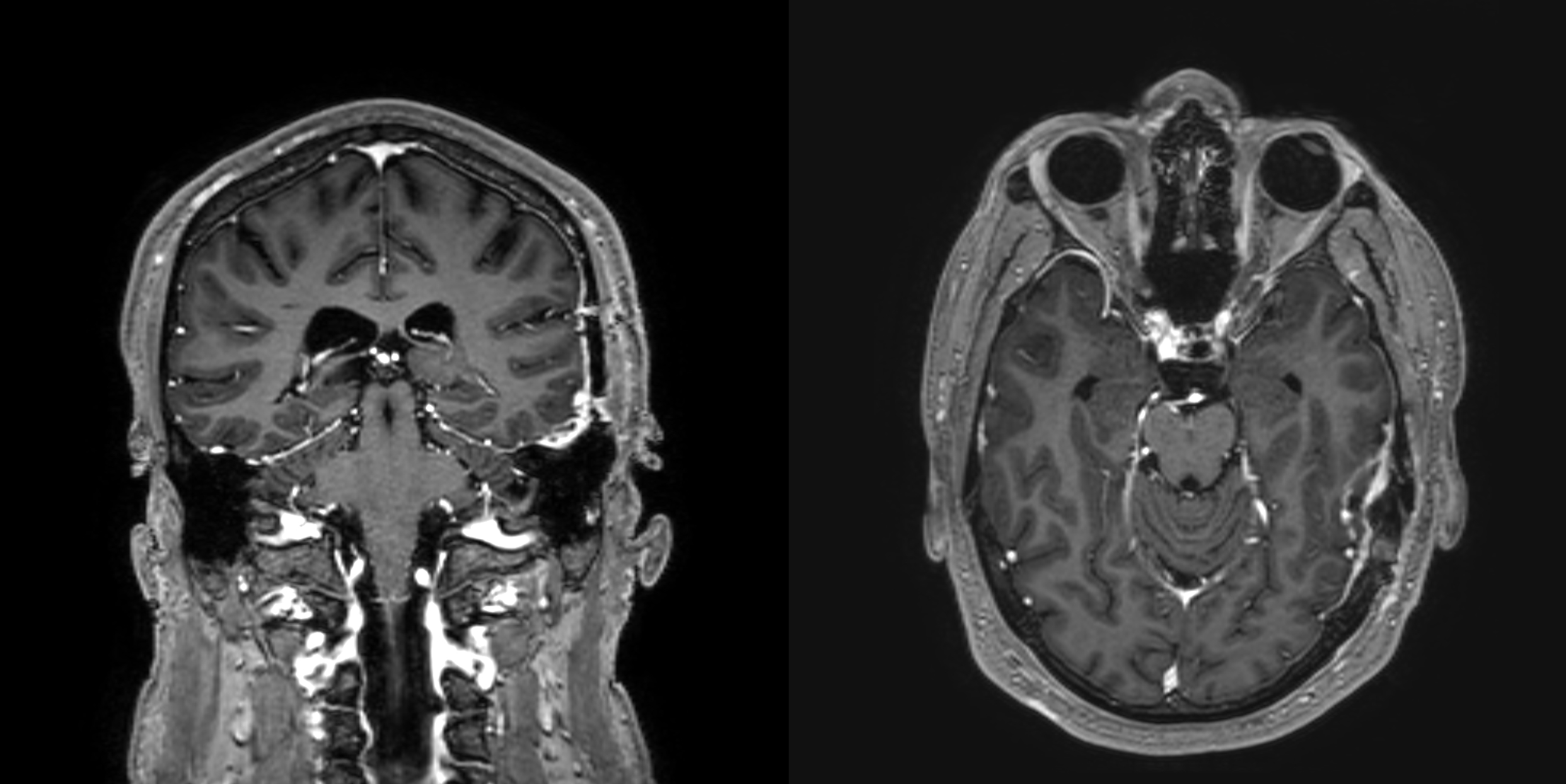
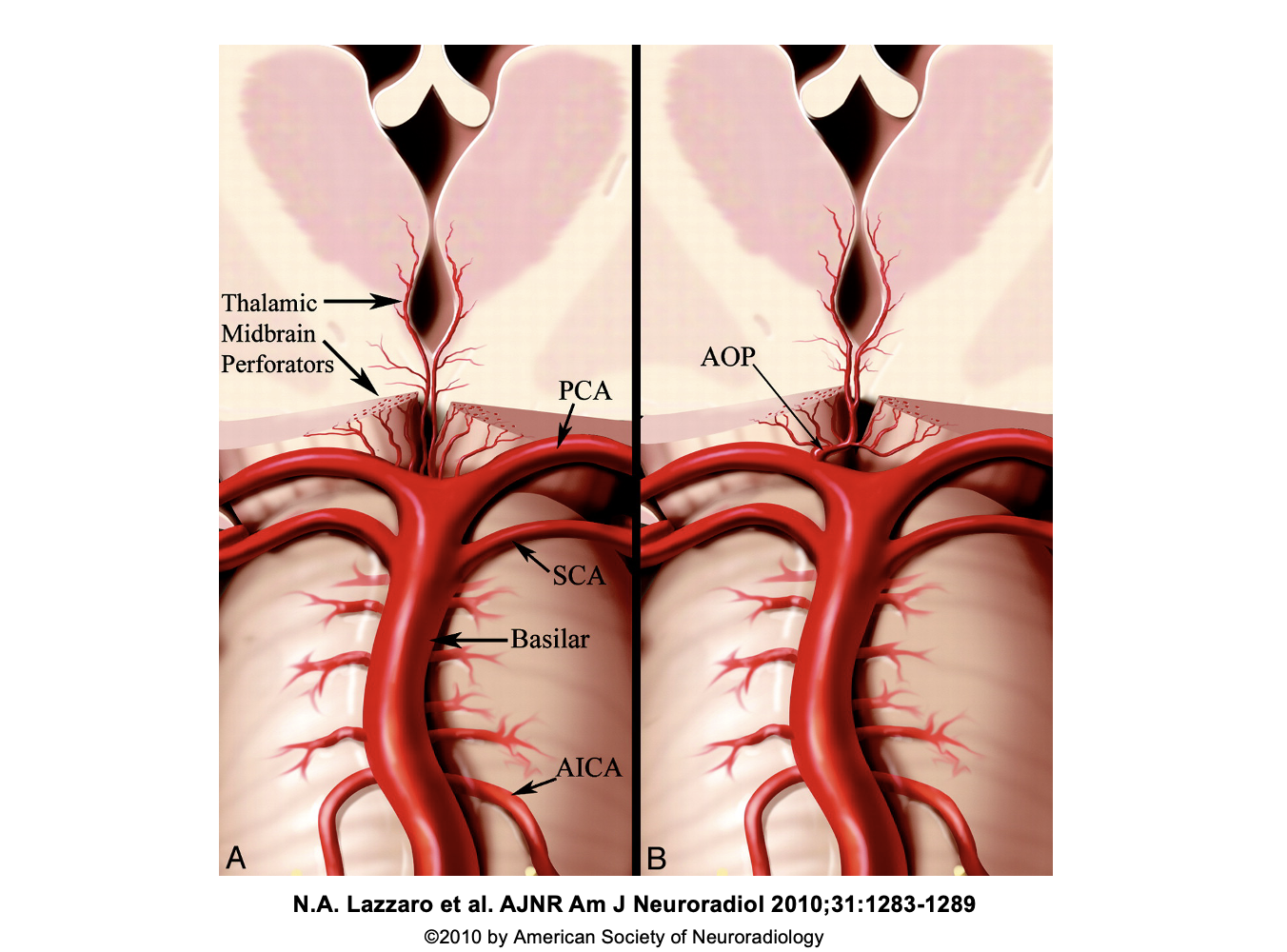
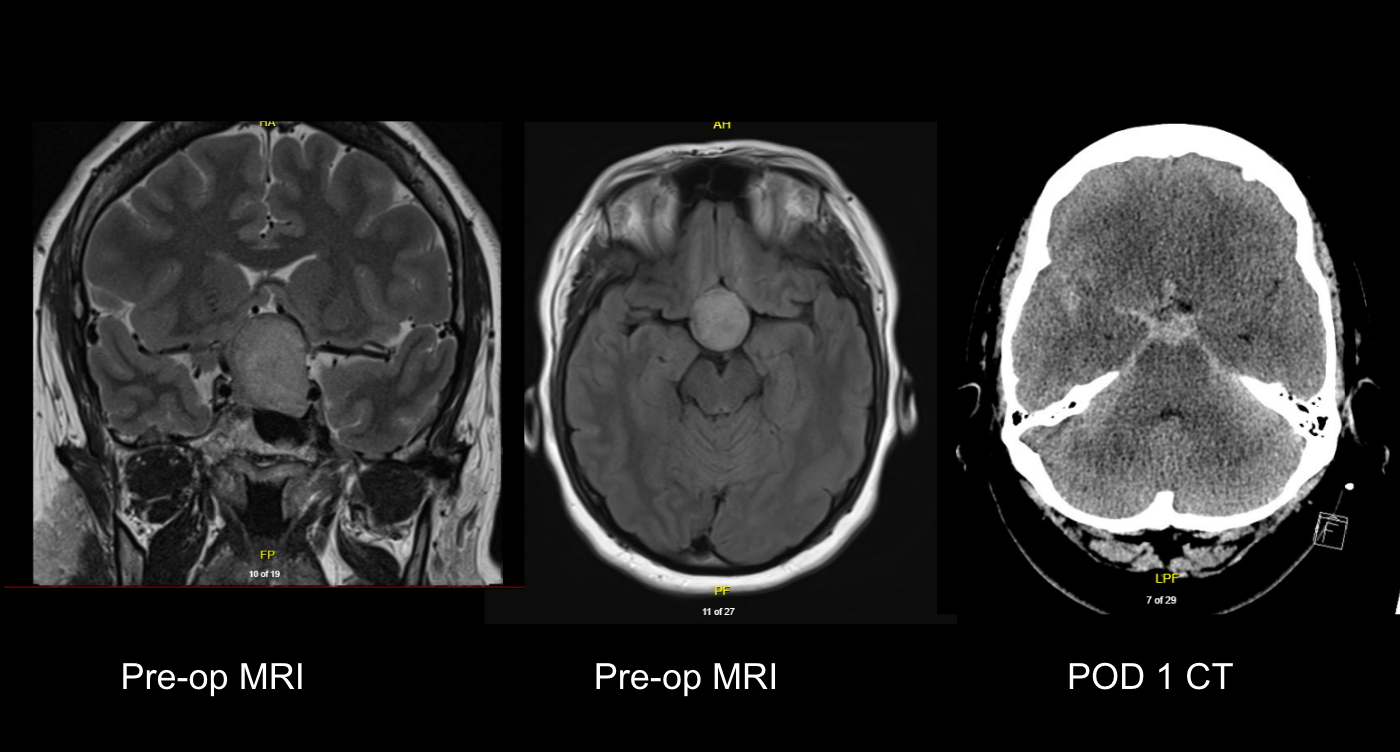
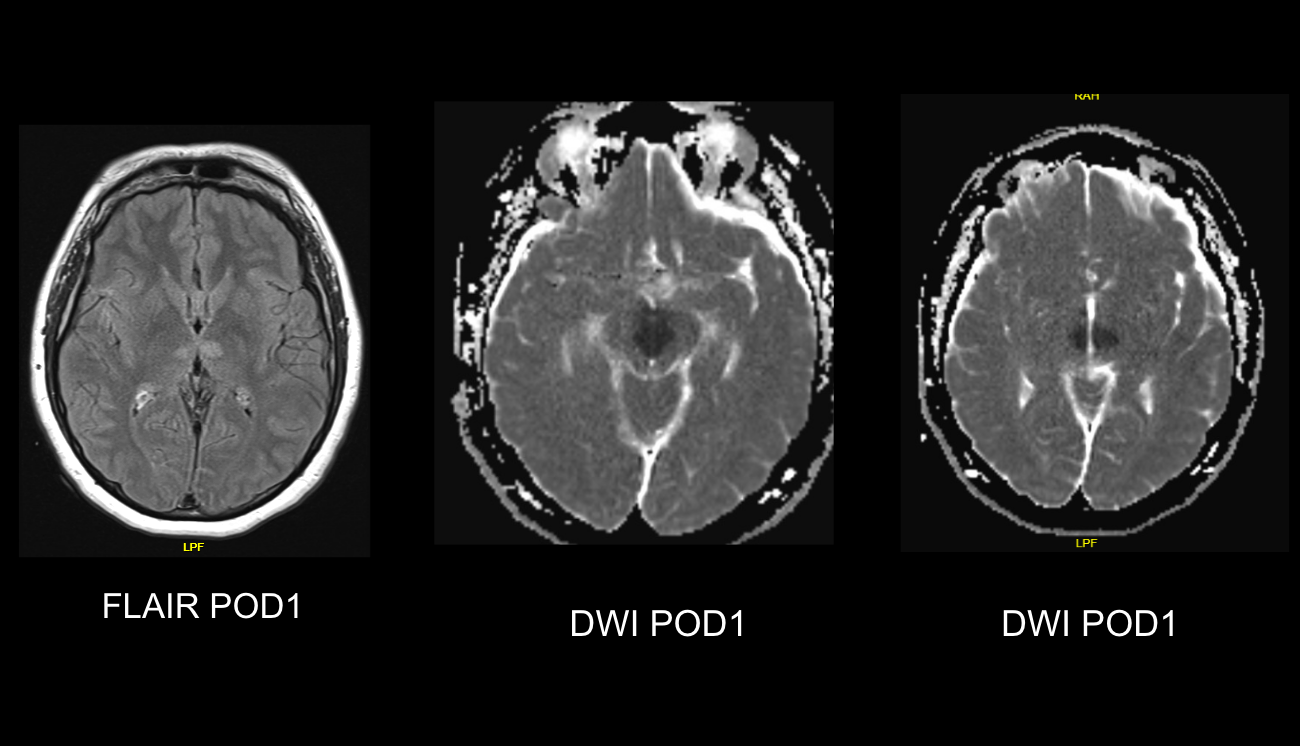
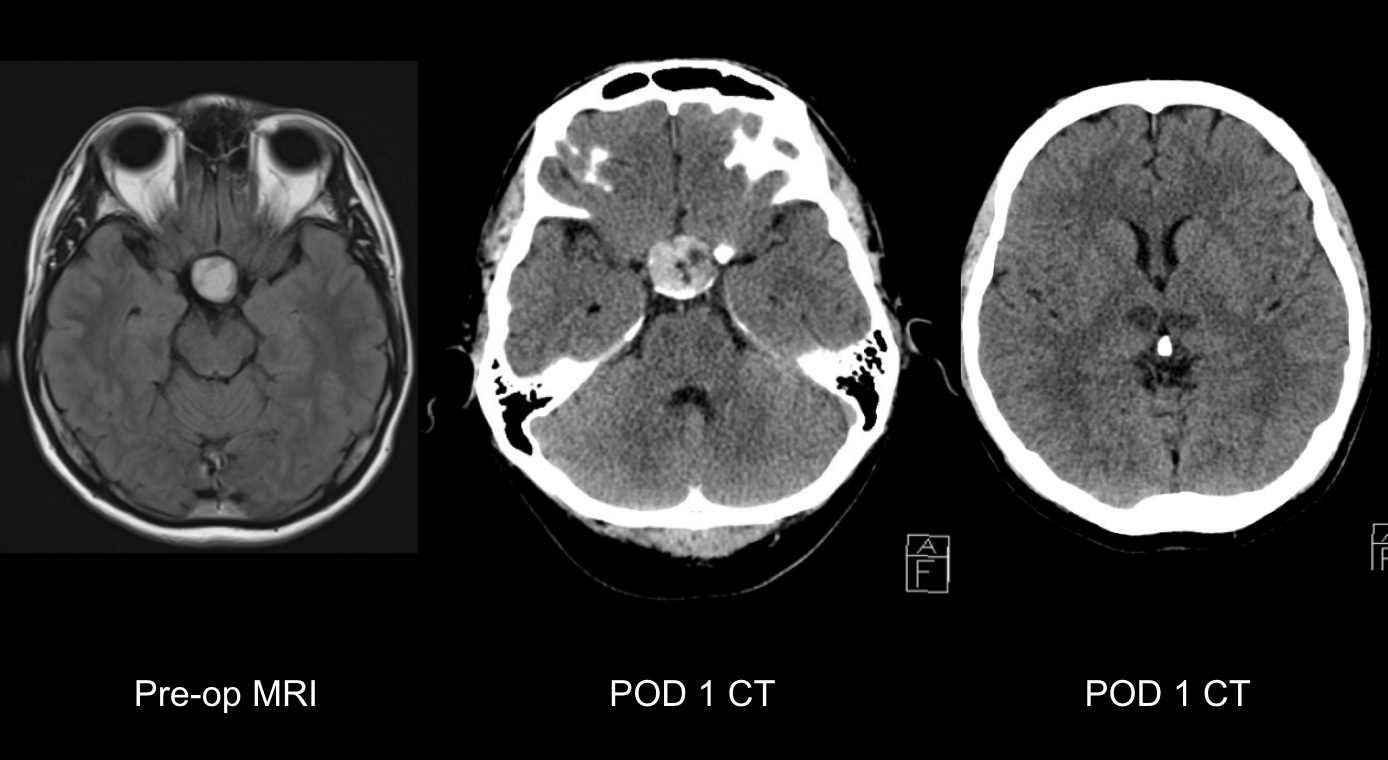
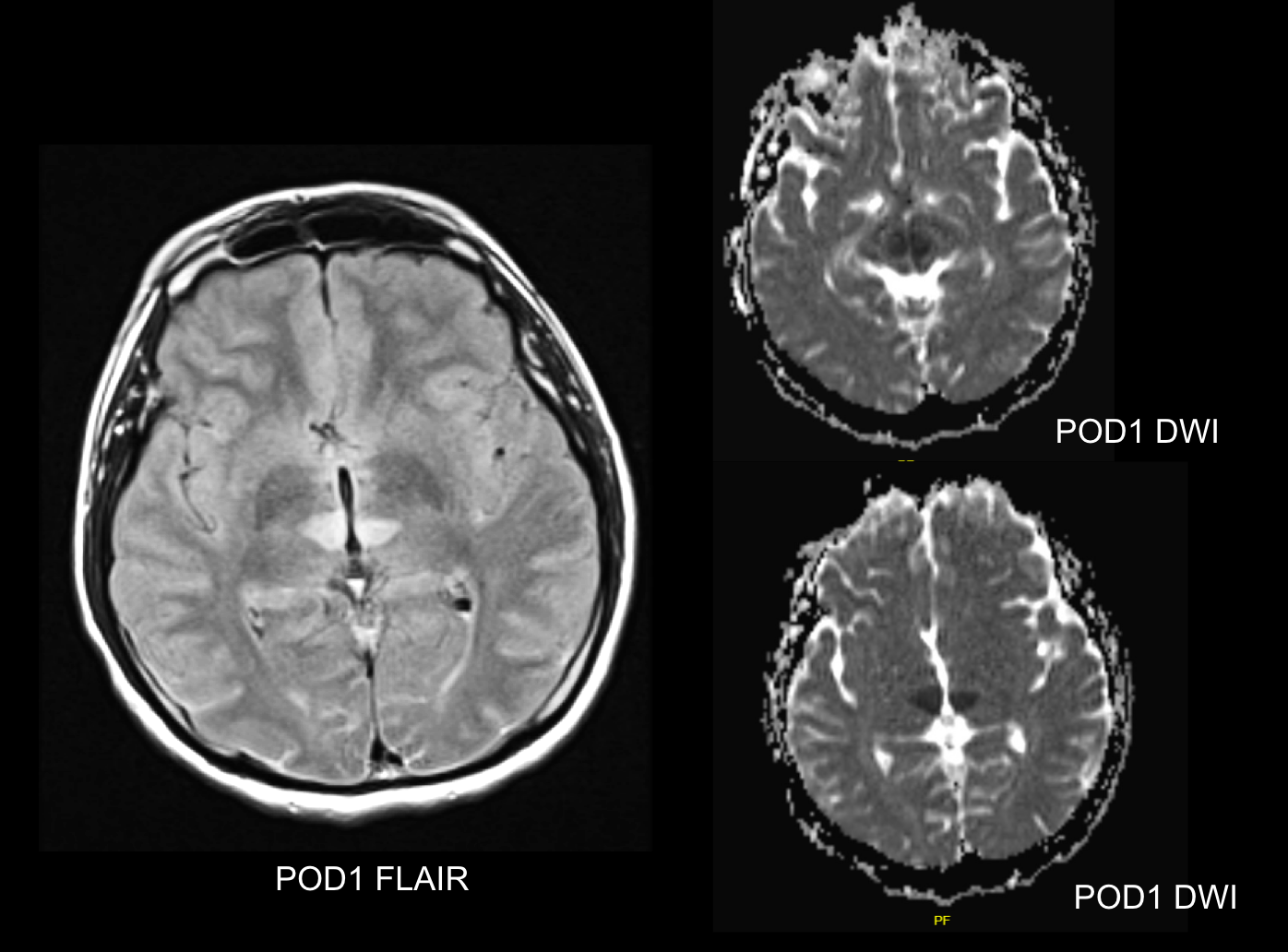
| Authors | Age and Sex | Tumour Characteristics | GOS, Follow Up |
| Sankar et al., 20088 | 50F | Firm | 4, 6 months |
| Pereira et al., 201911 | 52F | Firm | 3, 1 year |
| Aryan et al.,201613 | 40M | Firm | 3, 6 weeks |
| Konar et al., 202110 | 55F | Soft, vascular | 3, 3 months |
| Pilonieta et al.,202212 | 44F | Firm | 3, non-specified |
| Sannwald et al.,20229 | 40F | Rigid | 3, 2 years |
| Current Case 1 | 39F | Firm | 2, 6 months |
| Current Case 2 | 46M | Cystic | 3, 3.5 months |
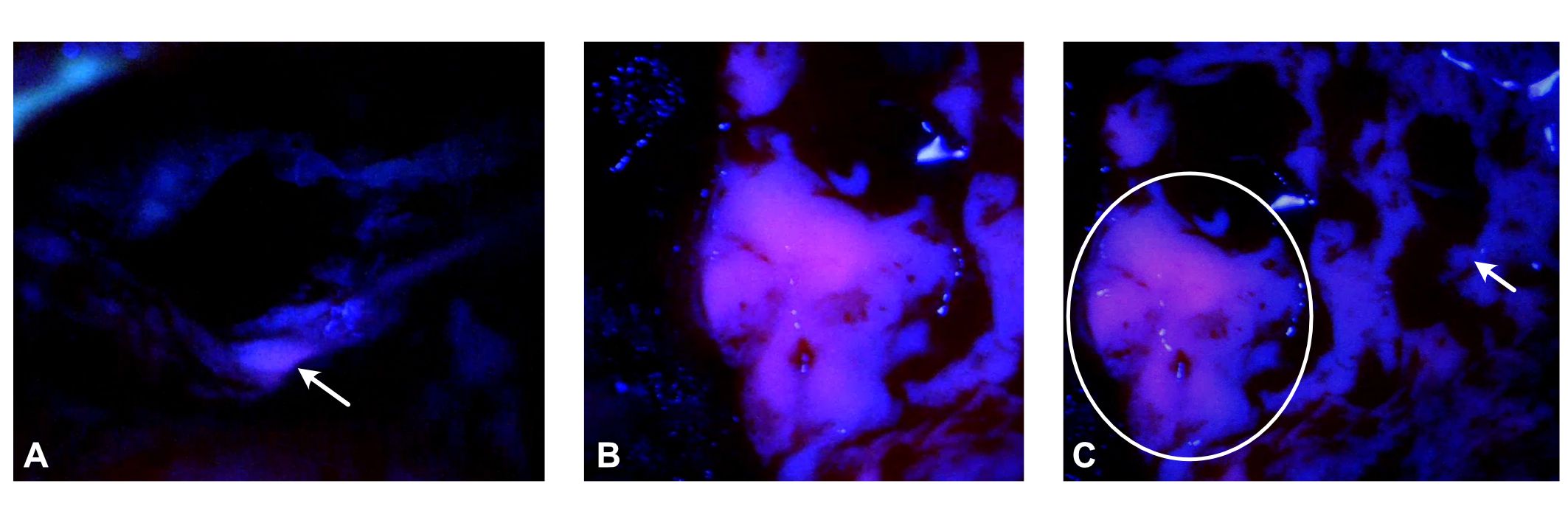
|
Pathology/ response |
5-ALA response (Number of cases) |
Total resection |
|---|---|---|
|
CNS Lymphoma |
Non (1) |
Yes |
|
Anaplastic Meningioma |
High (1) |
Yes |
|
Choroid plexus papilloma |
High (1) |
Yes |
|
Metastatic Melanoma |
Moderate (1) |
Yes |
|
Atypical teratoid rhabdoid tumor |
High (1) |
Yes |
|
Atypical Meningioma |
High (2) |
Yes |
|
Meningioma |
Moderate (1) |
Yes, except in 1 case with high response |
|
Glioneuronal tumor |
High (1) |
Yes |
|
Metastatic Adenocarcinoma |
High (1) |
Yes |
Seven databases (Ovid Medline, PubMed, Web of Science, EMBASE, BIOSIS, Scopus, Global Health, Cochrane) were searched up to August 2, 2021, using terms related to radiosurgery and brain metastasis. A three-level screening identified relevant studies. Data extraction included study type, population, SRS details, and outcomes. Variables recorded were histopathology, resection degree, number of metastases, SRS platform, dose parameters, cavity volume, margin, time to SRS, local control at 12/24 months, overall, and progression-free survival. Significant predictors were noted.
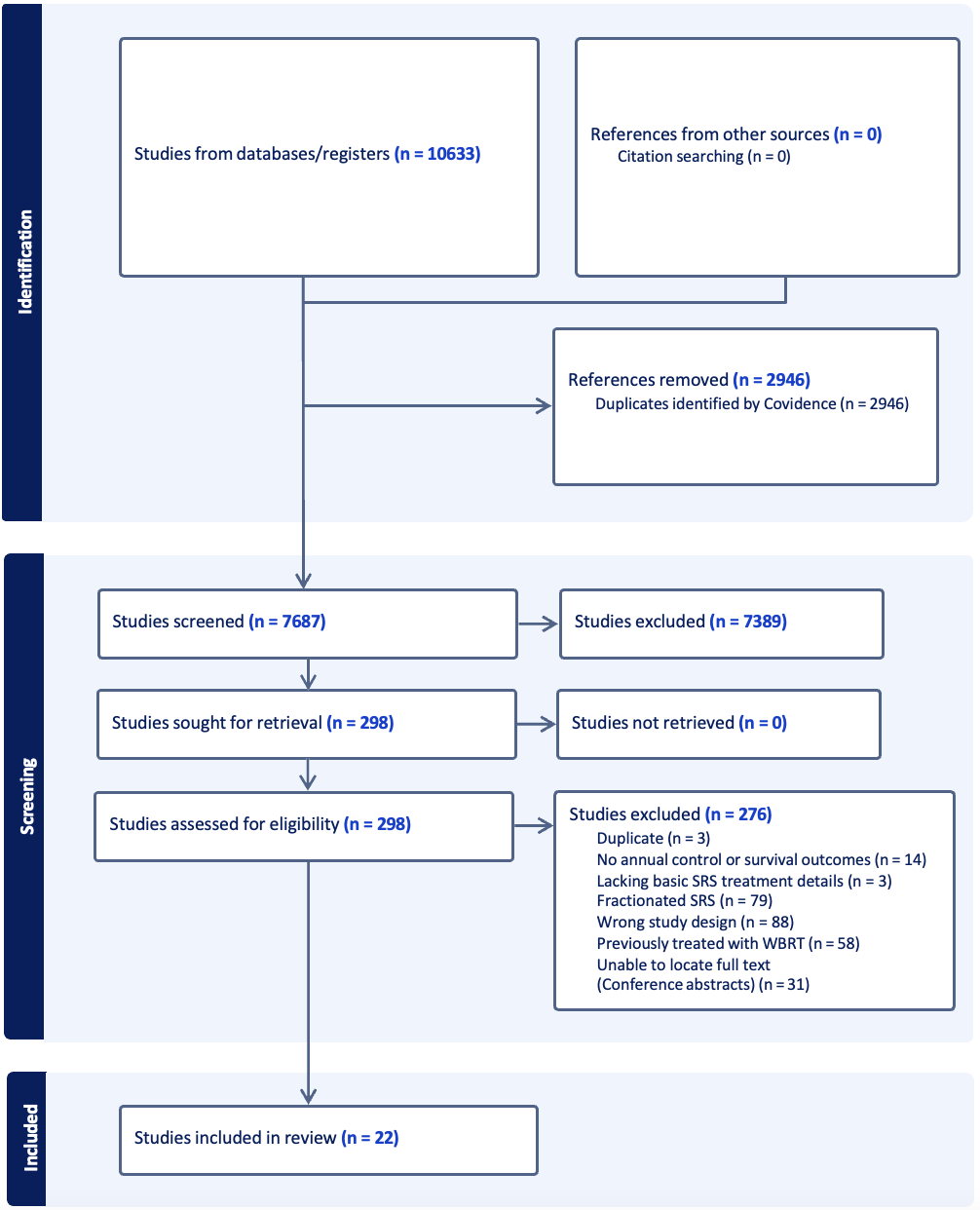
From 10,633 articles, 22 studies with 1,749 cavities. Local control at 12 months was 50–100% (median 82%, IQR 73–84.4%). Distant progression at 12 months was 36–64% (median 45.5%, IQR 38–51%) and at 24 months 39–76% (median 53%, IQR 46–55%). Histology, radiation dose, tumor size, extent of resection, treatment timing, tumor depth, and dural/pial attachment impacted local control, whereas primary disease status, surgical corridor coverage, and tumor location did not.
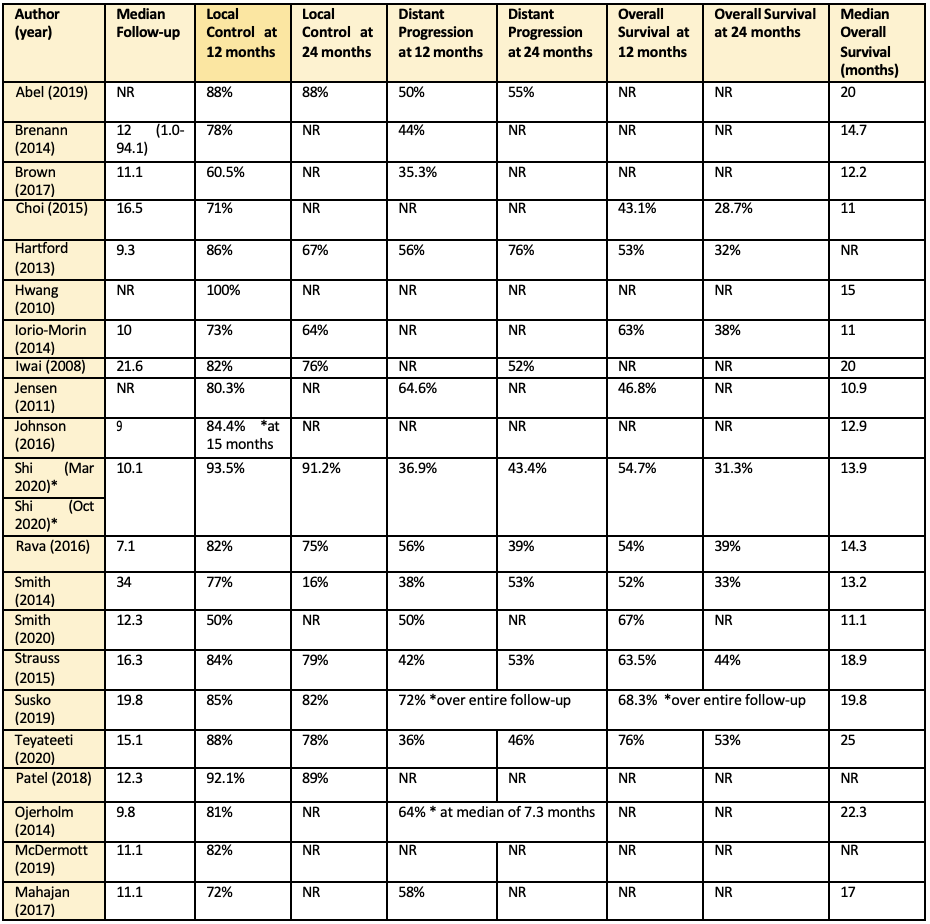
|
Patient Related Characteristics |
||
|
Sex |
Nil |
Iorio-Morin, Smith |
|
Age |
Nil |
McDermott, Smith |
|
KPS/RTOG |
Nil |
Iorio-Morin |
|
Focal Neurological Deficits |
Nil |
Iorio-Morin |
|
Primary Disease Related Characteristics |
||
|
Extracranial RT |
Nil |
Iorio-Morin |
|
Progression of Primary |
Nil |
Iorio-Morin |
|
GPA |
Nil |
Mahajan, Strauss |
|
Systemic Disease Status |
Nil |
Mahajan |
|
Hormonal Therapy |
Nil |
Shi |
|
Factors |
Studies |
|
|
Tumor Related Characteristics |
||
|
|
Significant on MVA |
Not Significant on MVA |
|
Histology |
Brennan |
Abel, Iorio-Morin, Jensen, Mahajan, Mcdermott, Ojerholm*, Rava, Shi, Smith, Strauss, Teyateeti, Patel |
|
Dimensions: |
||
|
Pre-op Diameter |
Brennan, Jensen |
Harford*, Ojerholm, Rava, Teyateeti, Patel |
|
Cavity Diameter |
Mahajan |
Abel, Brennan, Jensen, Mcdermott, Rava |
|
Cavity Volume |
Jensen |
Ioro, McDermott, Rava, Strauss, Susko, Teyateeti, Patel |
|
Extent of Resection |
Ojerholm |
Abel, Hartford, Iorio-Morin, Jensen |
|
Attachments (Pial, Dural) |
Brennan, Susko |
McDermott, Teyateeti |
|
Location (Supra, Infratentorial) |
Nil |
Brennan, Iorio-Morin, Jensen, McDermott, Ojerholm, Rava |
|
Treatment Related Characteristics |
||
|
Dose |
Iorio-Morin, Iwai, Patel, Jensen |
Brennan, Hartford, McDermott, Rava, Strauss, Susko, Teyateeti |
|
Isodose line |
Nil |
Iorio-Morin, Susko |
|
Number of Isocenters |
Nil |
Iorio-Morin |
|
Time to Treatment |
Iorio-Morin |
Brennan, McDermott, Ojerholm, Strauss*, Teyateeti |
|
Margin** |
Nil |
Shi |
|
PTV |
Nil |
Hartford, McDermott, Shi |
|
CI |
Nil |
Jensen, Rava, Susko, Abel |
|
Modified CI |
Nil |
Susko |
|
Corridor Coverage |
Nil |
Shi |
|
Univariate Analysis LR at 12 months |
HR (95% CI) |
p-value |
|
Patient Characteristics |
|
|
|
Age |
0.94 (0.89, 1.00) |
0.07 |
|
Sex |
0.90 (0.31, 2.61) |
0.85 |
|
ECOG grade at SRS |
0.94 (0.59, 1.51) |
0.81 |
|
KPS score at SRS |
1.01 (0.96, 1.06) |
0.55 |
|
Primary Disease |
|
|
|
Radiosensitivity |
2.22 (0.62, 7.86) |
0.21 |
|
Primary Disease State |
0.55 (0.16, 1.93) |
0.35 |
|
Steroid Used |
1.47 (0.50, 4.30) |
0.47 |
|
Tumor Characteristics |
|
|
|
Extent of Resection |
0.87 (0.25, 3.03) |
0.83 |
|
Cavity Volume |
1.05 (0.94, 1.17) |
0.33 |
|
Maximum Dimension |
|
|
|
Max Length |
1.02 (0.95, 1.09) |
0.49 |
|
Max Width |
0.98 (0.922, 1.05) |
0.71 |
|
Max Height |
0.99 (0.92, 1.07) |
0.87 |
|
3 cm cut-off for max diameter |
2.479 (0.71, 8.58) |
0.15 |
|
Tumor Location Depth (Superficial vs. Deep) Compartment (Supra vs Infratentorial) Pattern of Enhancement Shape (Smooth vs. Irregular) Edema (Mild vs. Moderate vs. Severe) SRS Characteristics Marginal dose Maximal dose Plan Conformity Paddick Conformity Index PIV/TVC Surgical Corridor Coverage Dural Coverage Time to SRS (TTT) in days TTT 14-days cut-off |
1.79 (0.69, 4.62) |
0.22 |
|
1.96 (0.63, 6.10) |
0.24 |
|
|
0.76 (0.39, 1.48) |
0.43 |
|
|
1.77 (0.54, 5.82) |
0.34 |
|
|
1.00 (0.45, 2.21) |
1.00 |
|
|
0.83 (0.52, 1.32) |
0.44 |
|
|
0.92 (0.73, 1.17) |
0.52 |
|
|
0.24 (0.00, 12.01) |
0.48 |
|
|
1.49 (0.37, 5.96) |
0.57 |
|
|
2.50 (0.74, 8.44) |
0.14 |
|
|
1.32 (0.46, 3.81) |
0.59 |
|
|
1.00 (0.98, 1.03) |
0.39 |
|
|
0.75 (0.21, 2.66) |
0.66 |
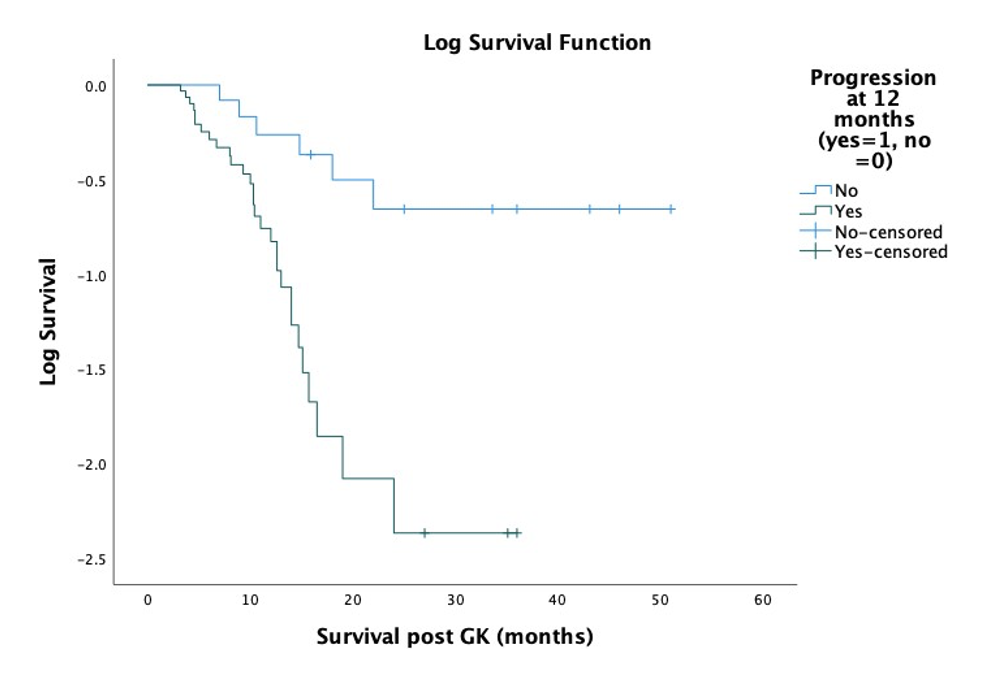
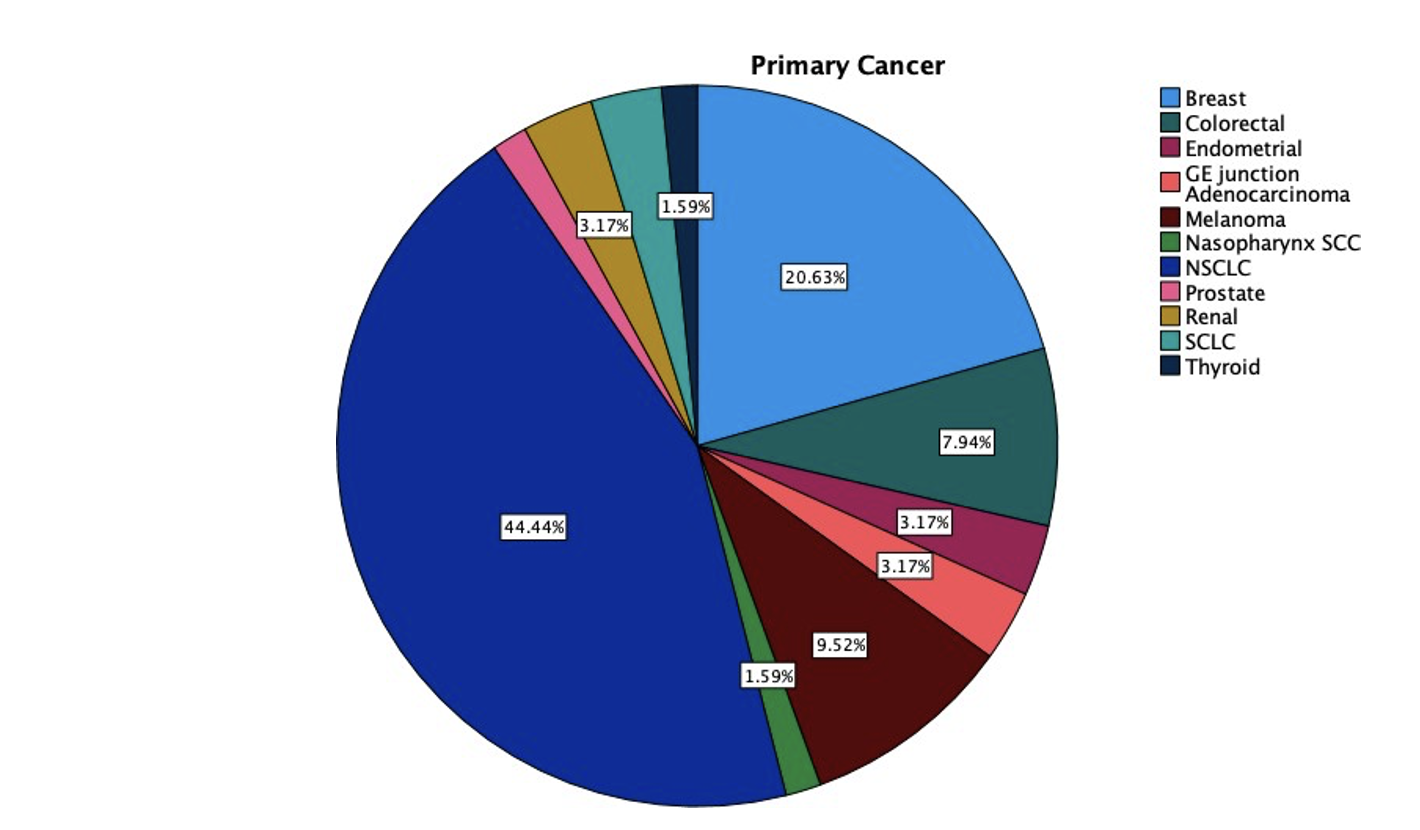
|
|
Survival at 12 months |
Survival at 24 months |
||
|
|
HR (95% CI) |
p-value |
HR (95% CI) |
p-value |
|
Patient Characteristics |
|
|
|
|
|
Age |
1.01 (0.96, 1.07) |
0.58 |
1.01 (0.96, 1.07) |
0.61 |
|
Sex |
0.75 (0.25, 2.21) |
0.60 |
1.12 (0.39, 3.18) |
0.83 |
|
ECOG |
1.50 (0.93, 2.43) |
0.09 |
1.63 (0.95, 2.80) |
0.07 |
|
KPS |
0.96 (0.092, 1.01) |
0.13 |
0.93 (0.87, 0.92) |
0.02 |
|
Primary Disease Characteristics |
|
|
|
|
|
Radiosensitivity |
0.88 (0.28, 2.76) |
0.83 |
0.62 (0.19, 1.97) |
0.42 |
|
Disease state (active vs. remission) |
1.97 (0.47, 8.26) |
0.35 |
1.89 (0.54, 6.65) |
0.31 |
|
Intracranial Progression |
|
|
|
|
|
Local at 12 months |
1.16 (0.37, 3.61) |
0.78 |
5.00 (1.25, 19.86) |
0.02 |
|
Distant at 12 months |
6.00 (1.52, 23.62) |
0.01 |
8.28 (2.53, 27.06) |
<0.00 |
|
Local at 24 months |
NA |
NA |
1.78 (6.13, 5.22) |
0.28 |
|
Distant at 24 months |
NA |
NA |
3.10 (087, 11.03) |
0.08 |

Introduction
The term “Endoscopic transorbital approach surgery-ETOA" describes a group of endoscopic surgical corridors through the orbit of the eye.
The first reported use of the orbit as an access corridor to the brain, was by the Italian psychiatrist Amarro Fiamberti, credited for being the original descriptor of the transorbital prefrontal lobotomy in 19371.
The application of ETOAs has been subsequently extended to the lesions of the anterolateral skull base such as meningiomas, schwannomas, dermoid cysts, CSF leak, and infections.
ETOA does present with limited morbidity, scars that are not easily visible,Craniotomies are not required and there is minimal brain retraction4.
The department of Neurosurgery of the McMaster University began performing ETOA in the year 2016. Upto the end of the year ending in December 2024,We had performed a total of 33 cases ON 29 patients
Methods:
This study presents a retrospective analysis of patient records was done from the year 2016 to 2024 at the Hamilton general hospital in Ontario, Canada.
The data collected included, demographic data, indication for surgery, complications, location of lesion, recurrence.
All of these surgeries were performed using a standard technique- A superior eyelid trans-orbital technique.
Results:
A total of 33 cases were done on 29 patients between the years of 2016 and 2024 Average age of patients was 47.67 with a median age of 46.
All patients had at least two weeks of follow up. the longest follow up period was 63 months of follow up the median follow up time was 4 months.
Fourteen male patients and fifteen female patients.
Patients most common indication for surgery was spheno-orbital meningioma.
| Indication | Number | Percentage |
| Spheno orbital meningioma | 11 | 33 |
| Frontal sinus mucocoele | 4 | 12.12 |
| Fibrous dysplasia | 2 | 6.06 |
| Trigeminal Schwannoma | 2 | 6.06 |
| osteomyelitis | 2 | 6.06 |
| Orbital roof fracture | 3 | 9.09 |
| Intraconal Cavernous angioma | 1 | 3.03 |
| encephalocoele with CSF leak | 1 | 3.03 |
| metastatic lesions | 2 | 6.06 |
| Orbital Cellulitis | 1 | 3.03 |
Complications:
The most common complication was transient V1 numbness, which was noted in the immediate post operative period. Headaches, transient diplopia,transient periorbital swelling,Wound infection, non diagnositic biopsy, proptosis and a cerebellar stroke were some of our recorded complications
Discussion:
The main indication for surgery in our institution was Spheno-orbital meningiomas. There is reduced rate of complications, cosmetically superior outcomes and overally high levels of patient satisfaction.
We do report that no patient from our series suffered visual loss or CSF leak as a result of this approach.
Our rate of complications in our series do mirror findings in other centrs who recorded frequent complications such diplopia, trigeminal paraesthesia, palpebral edema and periorbital ecchymosis 9,10. Our series did not record any post surgical epilepsy or patient mortality following a trans-orbital approach.
Conclusion:
Superior eyelid Transorbital approaches are a safe approach to the base of skull that have a lower complication rate in comparison to endoscopic or open alternatve approaches. The transorbital approach does have a reduced length of hospital admission and improve patient turnover. The main complications such as peri-orbital edema and facial hypesthesia tend to resolve fairly quickly.
Introduction: Hybrid Nerve Sheath Tumours (HNST) were introduced in the WHO Blue Book in the 2016 edition. Since that time, extracranial HNST are commonly identified but intracranial lesions are rare.
Methods: A systematic review of the literature was completed. Additionally, chart reviews were completed on two cases of HNST identified at our academic center.
Results: 3 reports of intracranial HNST located on a cranial nerve have been published to date. 2 cases of cranial nerve associated HNST have been identified at our academic centre.
Conclusion: HNSTs may be underreported in the cranial region.
Since the 2016 WHO classification of central nervous system tumours, hybrid nerve sheath tumours (HNST) have been recognized as tumours containing elements of more than one type of nerve sheath tumour. Although common peripherally and extracranially, few reports of intracranial HNST located on a cranial nerve have been published to date. At our tertiary care referral centre, there have been two documented cases of hybrid tumours arising on the CN VII/VIII complex. Here we describe these cases of presumed vestibular schwannoma that ultimately were diagnosed as hybrid tumours on pathological analysis. Additionally, a literature review on this topic was completed.
Chart reviews including imaging and neuropathological assessments were reviewed for two cases of HNST of CN VII/VIII tumour that occurred at a single quaternary care referral centre.
Additionally, a systematic literature search utilizing the search matrix (“hybrid” AND ((“vestibular schwannoma” OR “acoustic neuroma” OR “schwannoma” OR “neuroma” OR “cranial nerve”) AND (“intracranial” OR “CPA” OR “skull base” OR “cerebellopontine” OR “cranial nerve”))) was completed on July 11, 2024, resulting in 171 papers for screening. Ultimately 3 papers were included in the final analysis (Fig. 1)
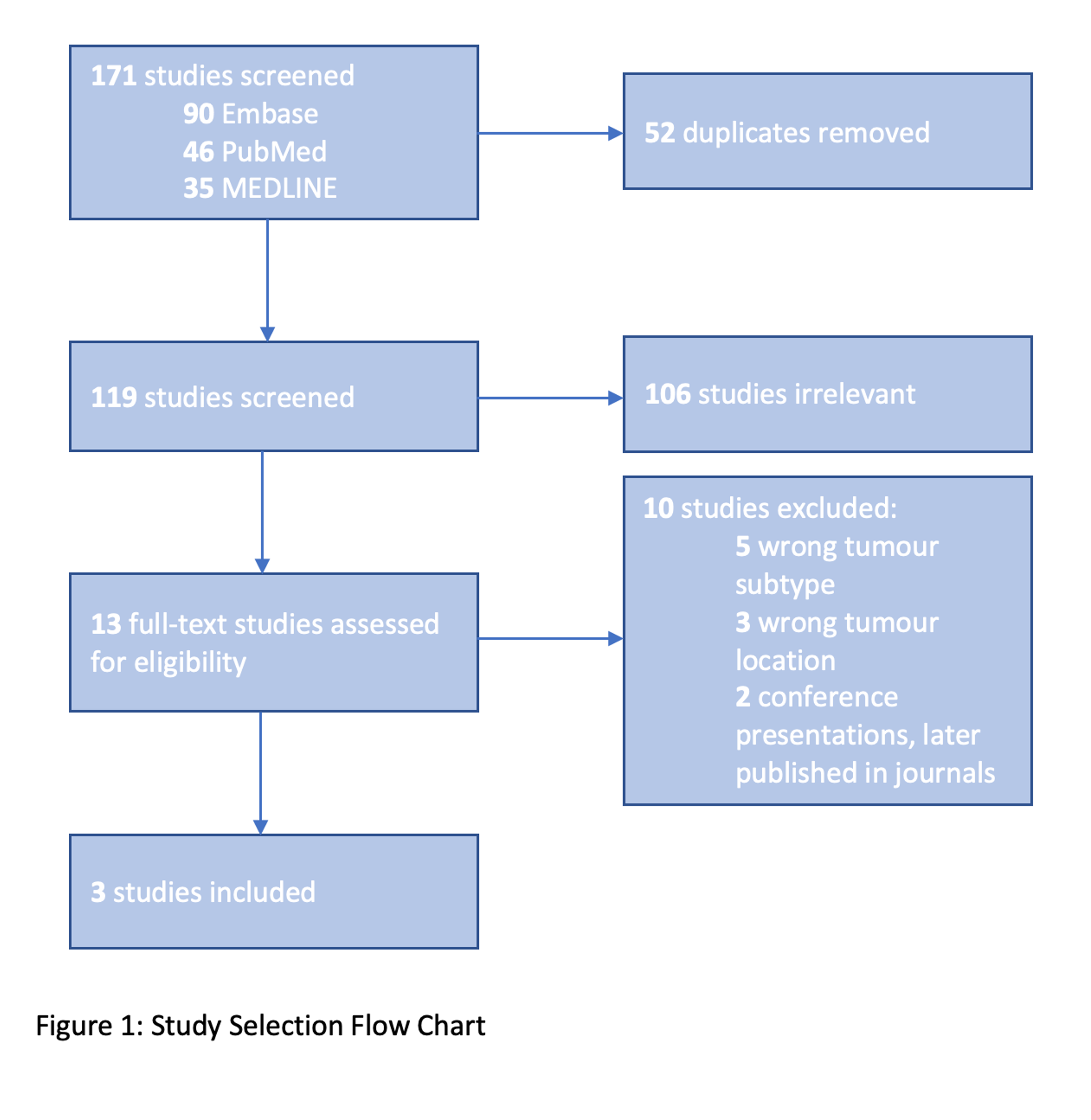
Three cases of HNST affecting cranial nerves were identified in the literature. One case of HNST of the facial nerve1 and one case of HNST of the trigeminal nerve2 were identified. Only one case of hybrid tumour located in the auditory canal has previously been reported3. We have identified two further cases of hybrid tumour in this location at our centre. A total of 643 vestibular schwannoma cases have been completed between 2001 and 2024 by this surgical team resulting in an institutional incidence of 0.31%.
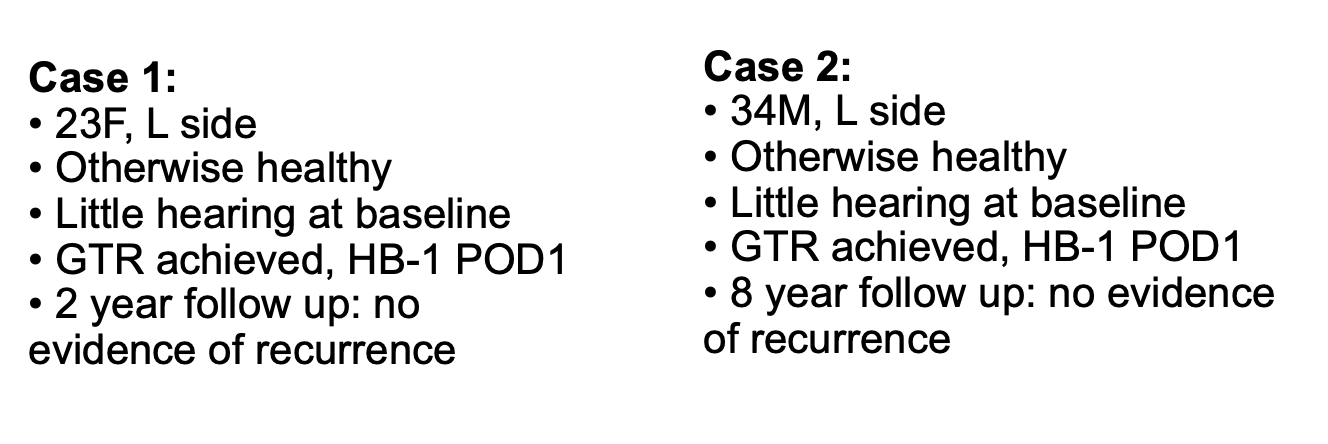
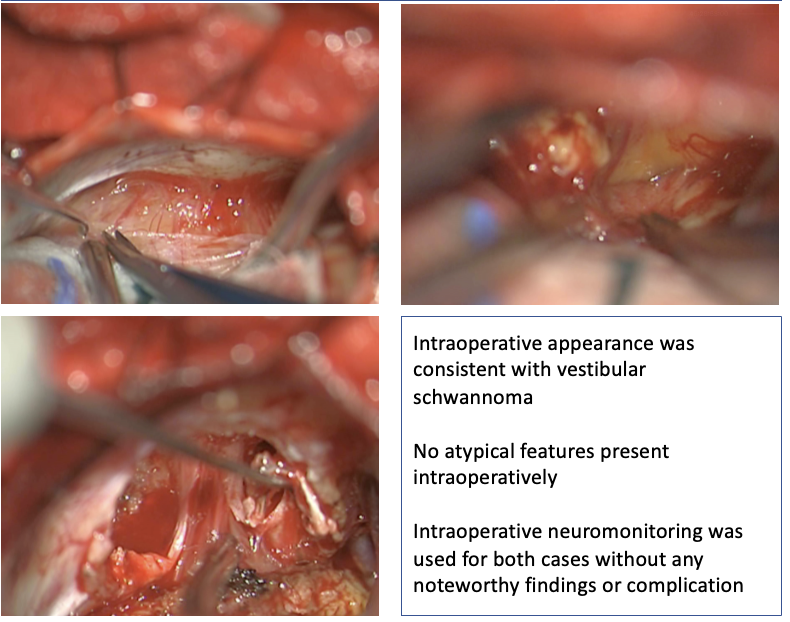
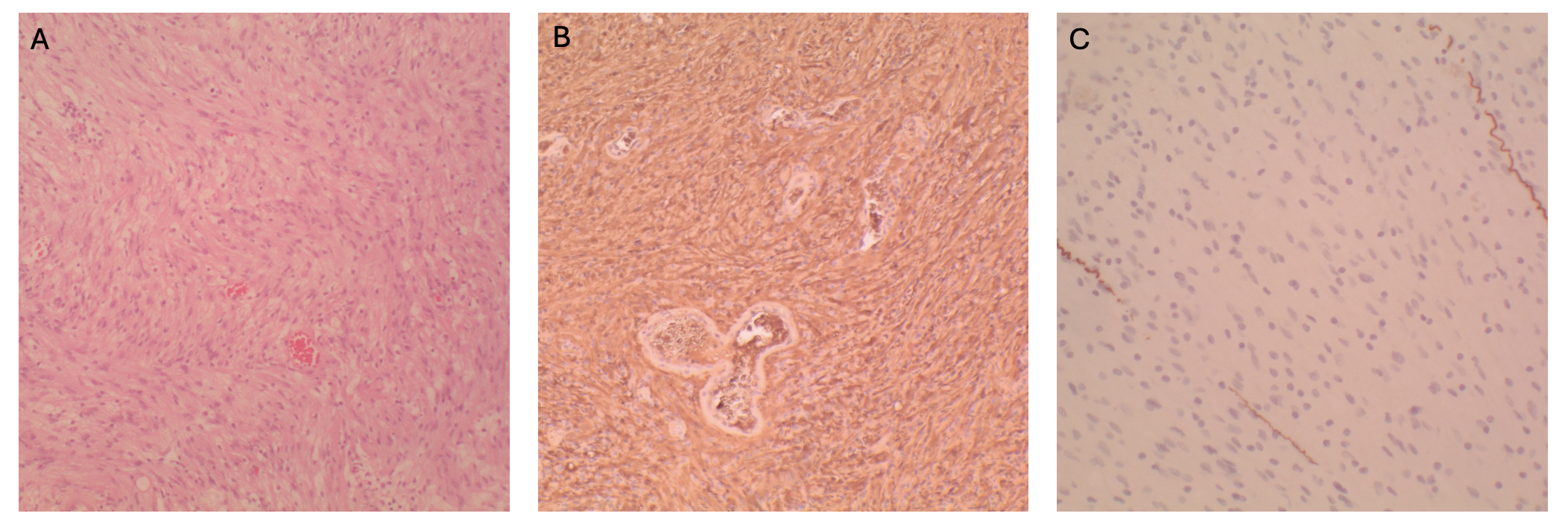
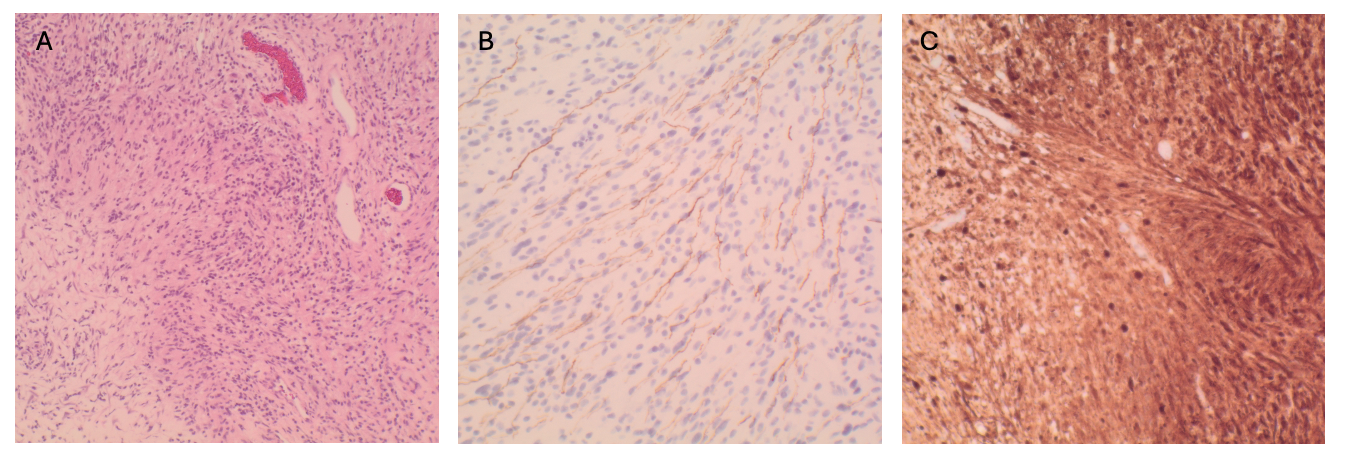
Hybrid nerve sheath tumour, schwannoma/neurofibroma subtype
HNSTs may be underreported in the cranial region.
Three cases if HNST have been reported in the literature to date. Here we describe an additional two cases occurring within the IAC, presenting as a vestibular schwannoma. Underreporting may relate to the relatively recent addition as a recognized phenomena to the list of WHO pathologies or due to insufficient tissue sampling provided to pathologists for tumours in this region to make this diagnosis.
1. Murray S, Bullock MJ, Taylor SM. A case of multiple neurofibroma/schwannoma hybrid tumors of the facial nerve. Otolaryngol Head Neck Surg [Internet]. 2015;152(3):569–70. Available from: http://dx.doi.org/10.1177/0194599814566791
2. Goyal-Honavar A, Gupta A, Chacko G, Chacko AG. Trigeminal hybrid nerve sheath tumor - a case report and literature review. Br J Neurosurg [Internet]. 2023;37(5):1326–9. Available from: http://dx.doi.org/10.1080/02688697.2020.1867061
3. Las Heras F, Martuza R, Caruso P, Rincon S, Stemmer-Rachamimov A. 24-year-old woman with an internal auditory canal mass. Hybrid peripheral nerve sheath tumor with schwannoma/perineurioma components: Correspondence. Brain Pathol [Internet]. 2013;23(3):361–2. Available from: http://dx.doi.org/10.1111/bpa.12055
VS is the most common tumour of the CPA with an annual incidence of 17.4/1 million. Typically: slow growth over time and as such, observation is a reasonable approach to management.
A portion of these tumour remain static and approximately 5-10% of these tumours will demonstrate spontaneous regression while under observation. Several previous case series have attempted to identify predictive factors for tumour growth and regression, but few have reached significance or demonstrated reproducible findings.
- No clinical factors have been identified
- No demographic factors have been identified
- Radiographic factors have been identified in small case series (Largest: N=14)
Using a clinical database of VS treated by one team at our institution, we identified 40 patients who have demonstrated significant spontaneous regression or complete resolution of their VS. All patients received a survey by mail and telephone. This survey was also distributed to a matched population of patients who had undergone resection for tumours that had demonstrated growth. For all patients who consented to participate, radiographic and clinical data was collected from patient charts in addition to survey responses. Medical comorbidities and medications provided through patient questionnaire were corroborated with patient charts. Tumor volume was approximated using the formula V = 4/3 x π x length/2 x width/2 x height/2 and nominal logistic regression was completed using JMPv17 with 50% tumor reduction as the reference value.
Of the 39 patients, 14 patients were excluded due to incomplete data
A total of 25 patients demonstrating spontaneous regression were included in radiographic analysis
Imaging features including degree of cystic component, presence of CSF in the IAC, smooth/irregular shape, and extension into IAC were not found to be predictive of regression in this study.
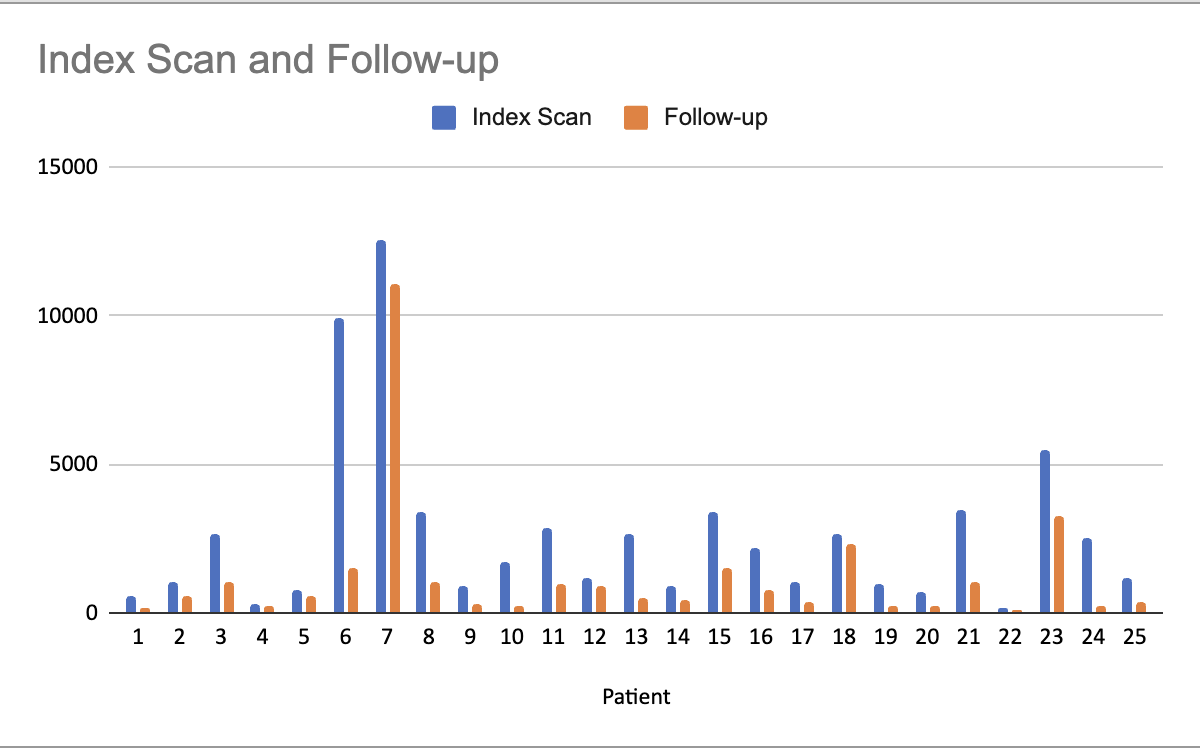
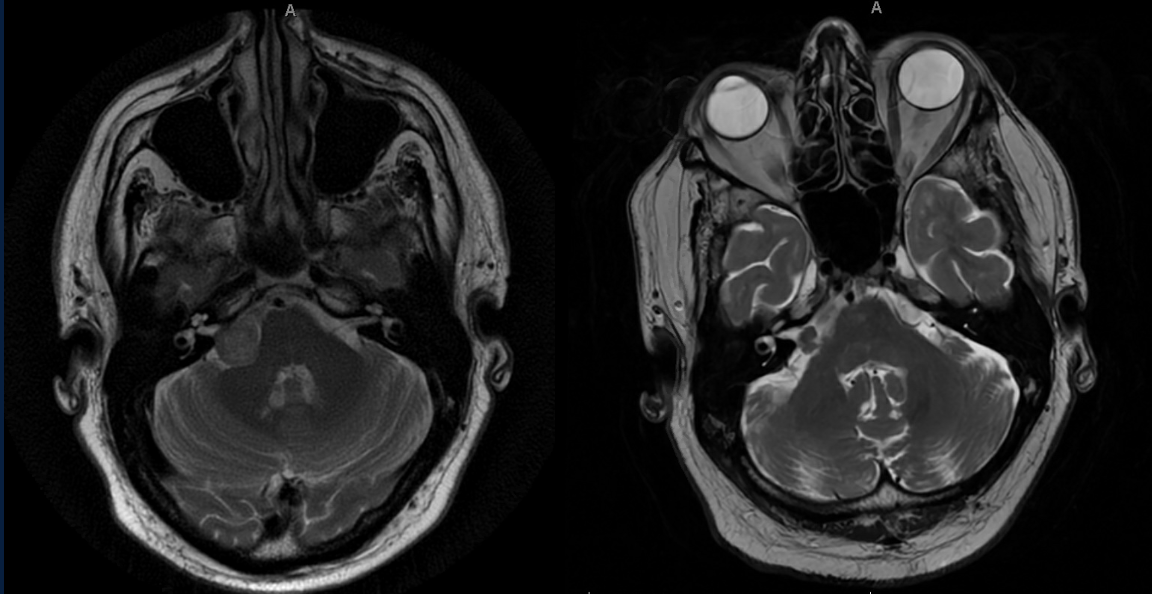
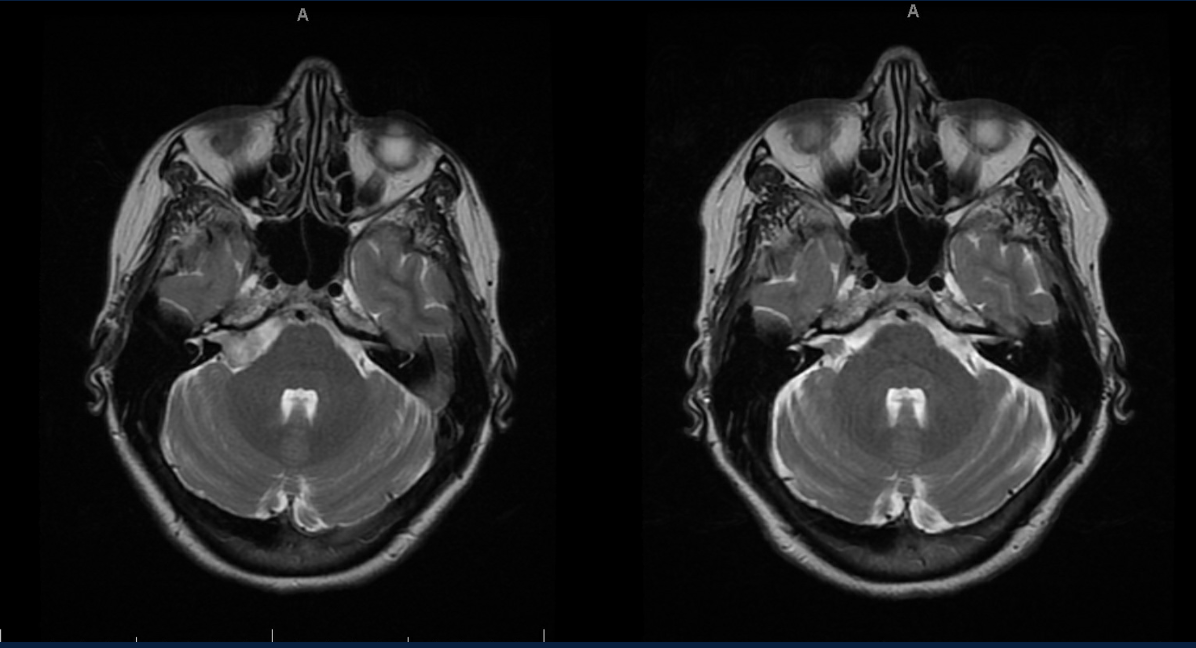
There was a response rate of 18/39 for both the spontaneous regression group as well as the control group. Although the surveys were distributed to a sex matched cohort, due to partial response rate, the final groups are not matched.
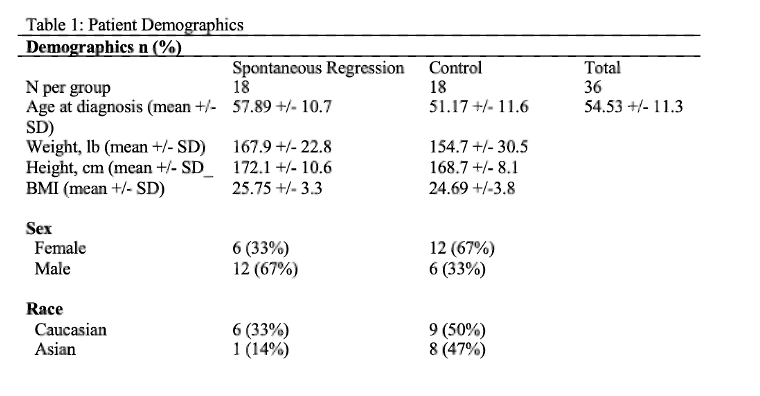
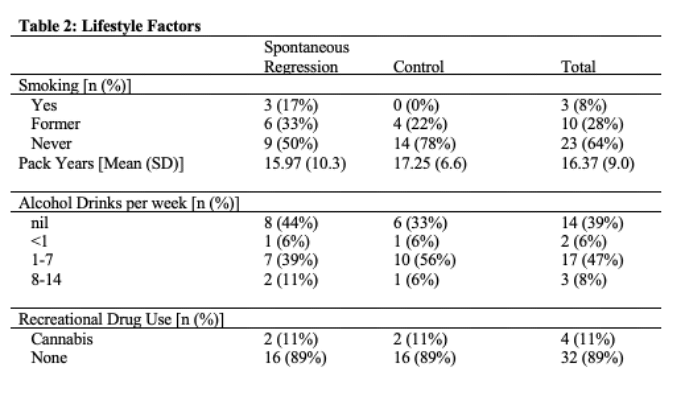
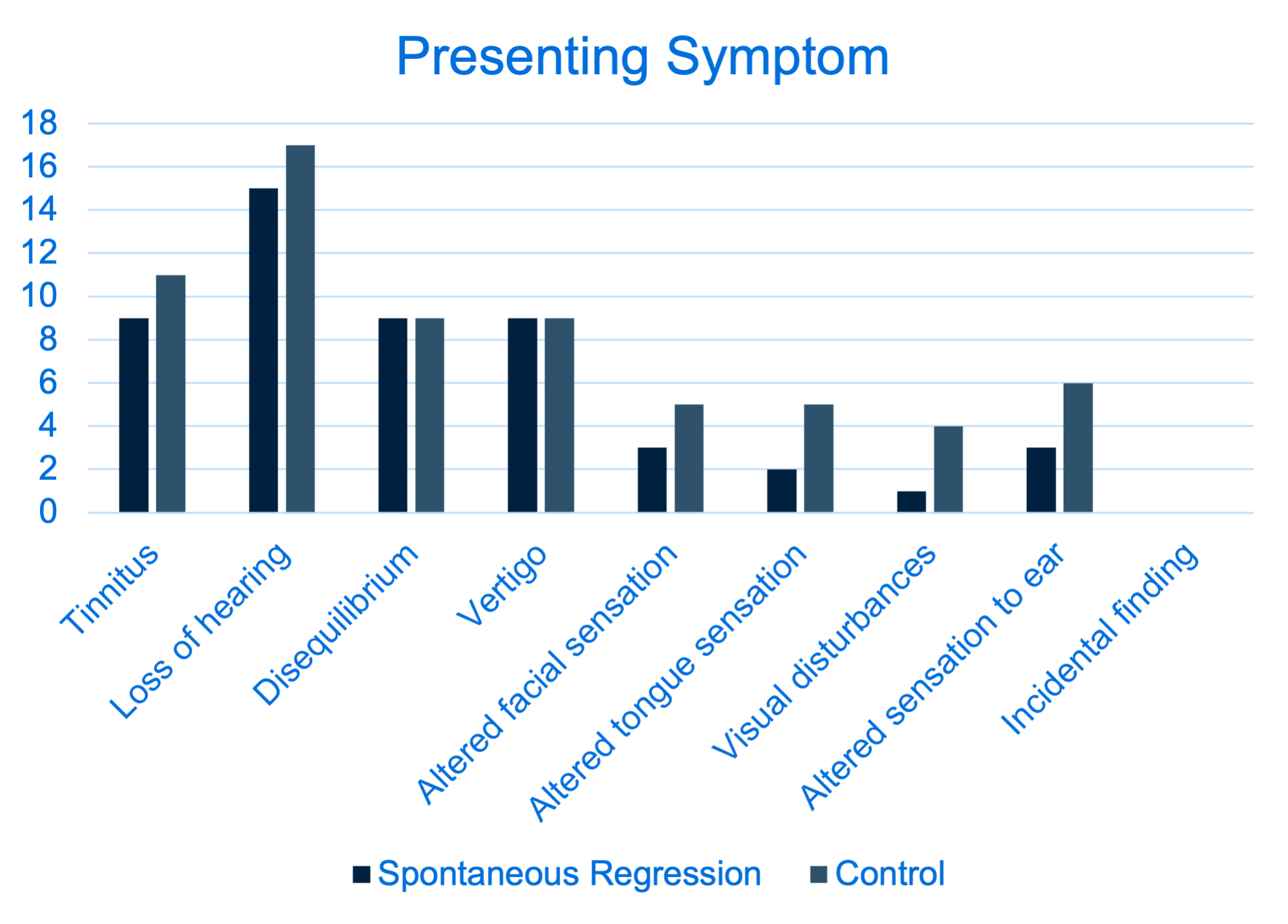

INTRODUCTION
METHODS AND RESULTS
|
Patient demographics and general characteristics |
||
|
Variable |
|
|
|
Asa Class, no (%) |
I |
2 (0.4%) |
|
II |
54 (10.2%) |
|
|
III |
388 (73.5%) |
|
|
IV |
84 (15.9%) |
|
|
Approach/Location |
|
|
|
Sellar/Suprasellar, no. (%) |
434 (80.1%) |
|
|
Anterior cranial fossa, no. (%) |
62 (11.4%) |
|
|
Posterior cranial fossa, no. (%) |
46 (8.5%) |
|
|
Blood loss (Mean in ml - min/max) |
340(100-3500) |
|
|
LOS (Mean in days) |
|
9.76 |
- Patients who developed a CSF leak had a significantly longer length of stay (p < 0.001). Additionally, the presence of a CSF leak was associated with a higher rate of 30-day readmission (p < 0.001), as well as the development of sepsis (p = 0.021) and diabetes insipidus (p < 0.001) in the postoperative period.
|
|
|||
|
Variable |
No CSF leak (n=502) |
CSF leak (n=40) |
p value |
|
Mean BMI in kg/m2 |
26.1 |
30.4 |
0.001 |
|
Mean LOS in days |
9.21 |
16.7 |
<0.001 |
|
Intraoperative CSF leak, no. |
234 |
40 |
0.001 |
|
Nasoseptal flap use |
468 |
30 |
0.001 |
|
Readmission at 30 days, no. |
13 |
31 |
< 0.001 |
|
PostOp. DI, no. |
12 (2.2%) |
60 (11.1%) |
< 0.001 |
- Surgical access to the clival region represents a formidable challenge due to its midline position, deep-seated location, and intricate neurovascular relationships.
- In recent years, extended endoscopic endonasal approaches (EEA) have emerged as a minimally invasive alternative, providing a direct corridor to this complex anatomical region.
- This report reviews the clinical presentation and outcomes of patients who underwent an endoscopic endonasal approach for the treatment of skull base lesions involving the clivus, detailing our surgical experience.
|
Chordoma extent of resection analysis |
|||
|
Variables |
GTR (6) |
STR (7) |
p value |
|
Mean PreOp Vol |
9.3 |
12.6 |
0.369 |
|
Midline location |
5 (38.5%) |
2 (15.4%) |
0.048 |
|
Mean blood loss |
425ml |
893 ml |
|
|
PostOp CSF leak |
1 |
1 |
0.99 |
|
Persistent oftalmoparesis at last FU |
1 (7.7%) |
3 (23.1%) |
0.033 |
|
Recurrence at last FU |
0 |
3 (23.1%) |
0.067 |
The endoscopic endonasal approach is a safe and effective alternative for managing clival pathologies. Its potential advantages include avoiding craniotomy and brain retraction, reducing neurovascular manipulation, and minimizing morbidity. While major complications have been rare, this technique does have limitations.
- Anterior skull base meningiomas are a heterogeneous group of tumors classified based on their primary site of attachment.
- Surgical intervention may be considered depending on the tumor’s size, anatomical relationships, and associated neurological deficits.
-This study aims to evaluate the clinical outcomes of patients with anterior skull base meningiomas who underwent EEA for tumor resection.
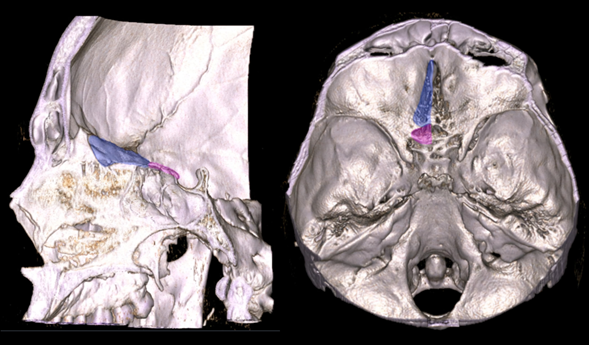
Twenty-five patients underwent an extended endoscopic endonasal approach for the resection of anterior skull base meningiomas. Seventeen patients (68%) had meningiomas located in the tuberculum sellae–planum sphenoidale region, while eight patients (32%) had olfactory groove meningiomas.
|
Patient demographics and general characteristics |
||||
|
Variable |
|
|
|
p value |
|
Tumor location, no (%) |
Olfactory groove |
|
8 (32%) |
|
|
Planum-Tubercullum |
|
17 (68%) |
||
|
Clinical presentation, no(%) |
Olfactory groove |
Headaches |
8 (100%) |
|
|
Hyposmia |
5 (62.5%) |
|||
|
Planum-Tubercullum |
Visual changes |
12 (70.58%) |
||
|
Headaches |
4 (23.52%) |
|||
|
III nerve dysfunction |
1 (5.88%) |
|||
|
Hyposmia |
1 (5.88%) |
|||
|
ASA Class, no (%) |
Olfactory groove |
III |
5(20%) |
|
|
IV |
3(12%) |
|||
|
Planum-Tubercullum |
III |
16(64%) |
||
|
IV |
1(4%) |
|||
|
Pre operative mean tumor volume (cm 3) |
|
|
|
0.03 |
|
Olfactory groove |
19.54 |
|
||
|
Planum-Tubercullum |
7.04 |
|
||
|
Lumbar drain, no. (%) |
|
|
|
0.294 |
|
Olfactory groove |
2 (8%) |
|
||
|
Planum-Tubercullum |
8 (32%) |
|
||
|
|
|
|
|
0.312 |
|
Nasoseptal flap, no. (%) |
Olfactory groove |
8 (32%) |
|
|
|
|
Planum-Tubercullum |
15(60%) |
|
|
|
LOS (Mean in days) |
|
|
|
0.46 |
|
Olfactory groove |
11.1 |
|
||
|
Planum-Tubercullum |
11.1 |
|
||
|
Readmission at 30 days, no. |
Planum-Tubercullum |
2 |
|
|
|
Post Operative characteristics |
||||
|
Variable |
|
|
|
p value |
|
Pathology WHO grade, no. (%) |
I |
23 (92%) |
||
|
II |
2 (8%) |
|||
|
Complications, no. (%) |
CSF leak |
4 (16%) |
||
|
Vascular Injury |
1 (4%) |
|||
|
Resection, no (%*), mean tumor volume in cm3 |
Total - Near total |
|
|
|
|
Olfactory groove |
7(87.5%) - 15.97 |
|
||
|
Planum-Tubercullum |
14 (82.4%) - 5.42 |
|
||
|
Subtotal |
|
|
0.03 |
|
|
Olfactory groove |
1(12.5%) - 37.41 |
|
||
|
Planum-Tubercullum |
3(17.6%) - 10.84 |
|
||
|
Recurrence, no (%) |
|
|
1 (4%) |
|
|
*Based on tumor location |
||||
The endoscopic endonasal approach is a safe and effective alternative for managing anterior cranial fossa meningiomas. Its potential advantages include avoiding craniotomy and brain retraction, reducing neurovascular manipulation, and minimizing morbidity. While major complications have been rare, this technique does have limitations.
This approach should be part of the cranial base surgeon’s armamentarium and considered a viable option for selected patients with these complex pathologies.
| Patient demographics and clinical characteristics | ||
| Number of patients | 7 | |
| Female sex, n (%) | 5 (71.4%) | |
| Age, mean (Min-Max) | 52 (24-78) | |
| Pathology, n (%) | ACTH-producing adenoma | 4 |
| GH-producing adenoma | 2 | |
| Non-functioning adenoma | 1 | |
| Tumor size, n (%) | <10 mm | 6 (85.7) |
| >10 mm | 1 (14.3) | |
| PostOperative outcomes | |||
| Tumor type | ICG Visualization | Tumor resection | Biochemical cure |
| ACTH-producing adenoma | 4 (100%) | GTR | Yes |
| GH-producing adenoma | 2(100%) | GTR | Yes |
| Non-functioning adenoma | 1(100%) | GTR | NA |
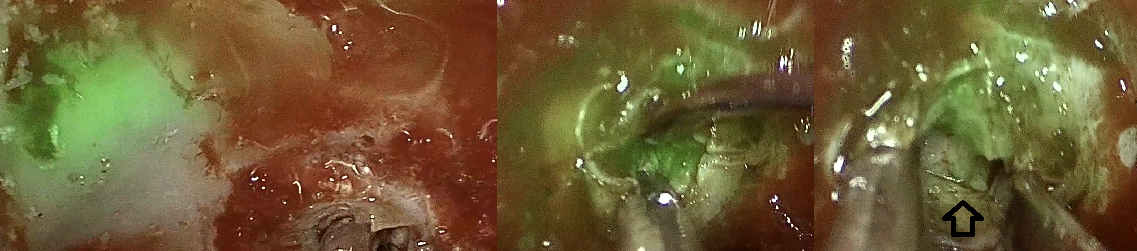
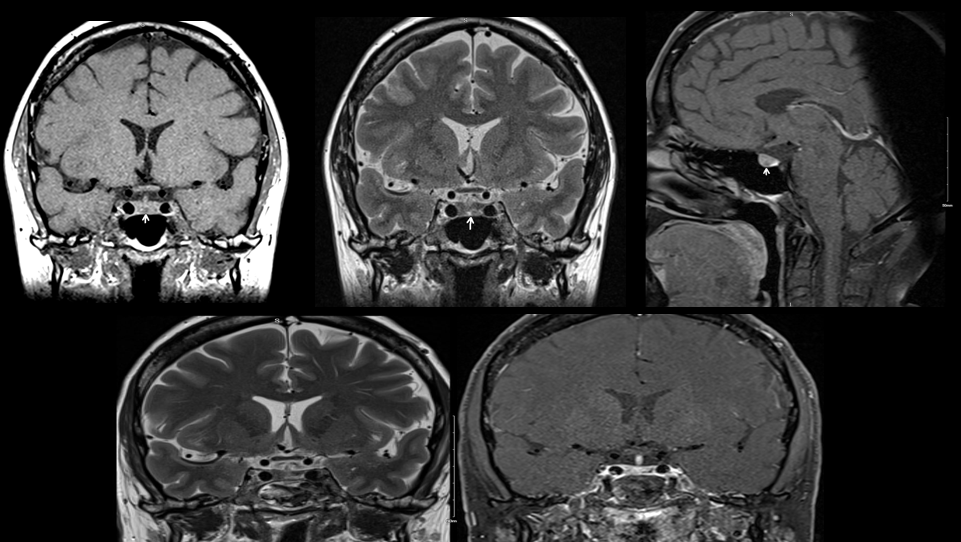
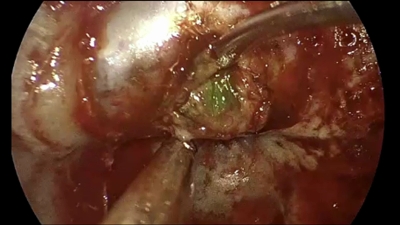

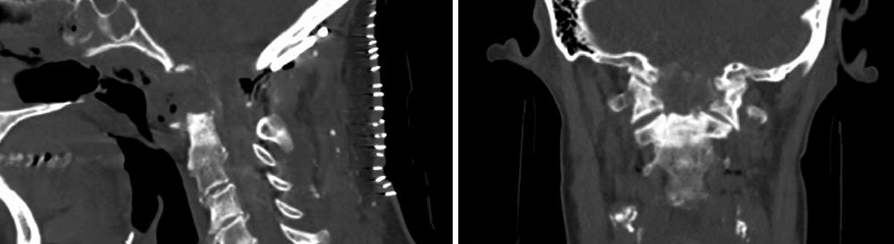
| Pre Operative - Operative characteristics | |||
| Variable | |||
| Presentation symptoms | Myelopathy | 13/17 (76%) | |
| Paresthesias - Sensory symptoms | 10/13 (77%) | ||
| Difficulty with fine hand movements | 7/13 (54%) | ||
| Walking disturbances - Neck pain | 9/13 (69%) | ||
| Headaches | 5/17 (29%) | ||
| Lower cranial nerve symptoms - Dizziness | 3/17 (18%) | ||
| Tinnitus | 2/17 (12%) | ||
| Pathologic conditions | C1/C2 pannus | 11/17 (65%) | |
| Chiari malformation type I | 2/17 (12%) | ||
| Basilar invagination 3/17 (18%) | 3/17 (18%) | ||
| Previous odontoid fracture 1/17 (6%) | 1/17 (6%) | ||
| Surgical procedure | Two-stages | 11/17 (65%) | |
| One stage | 2/17 (12%) | ||
| Endoscopic only | 3/17 (18%) | ||
| PostOperative characteristics - Complications - Outcomes | ||
| Variable | ||
| Extubation | Immediately | 7/17, 41% |
| Prolonged | 10/17, 59% | |
| Intra operative CSF leak | 4/17, 24% | |
| Vascular injury | 1/17, 6% | |
| Dysphagia | 8/17, 47% | |
| Infection | 3/17, 18% | |
| Myelopathy resolution | Complete | 14/17, 82% |

We aimed to molecularly characterize this RTOG-0539 Clinical Trial cohort to identify biomarkers of RT response and therapeutic targets.
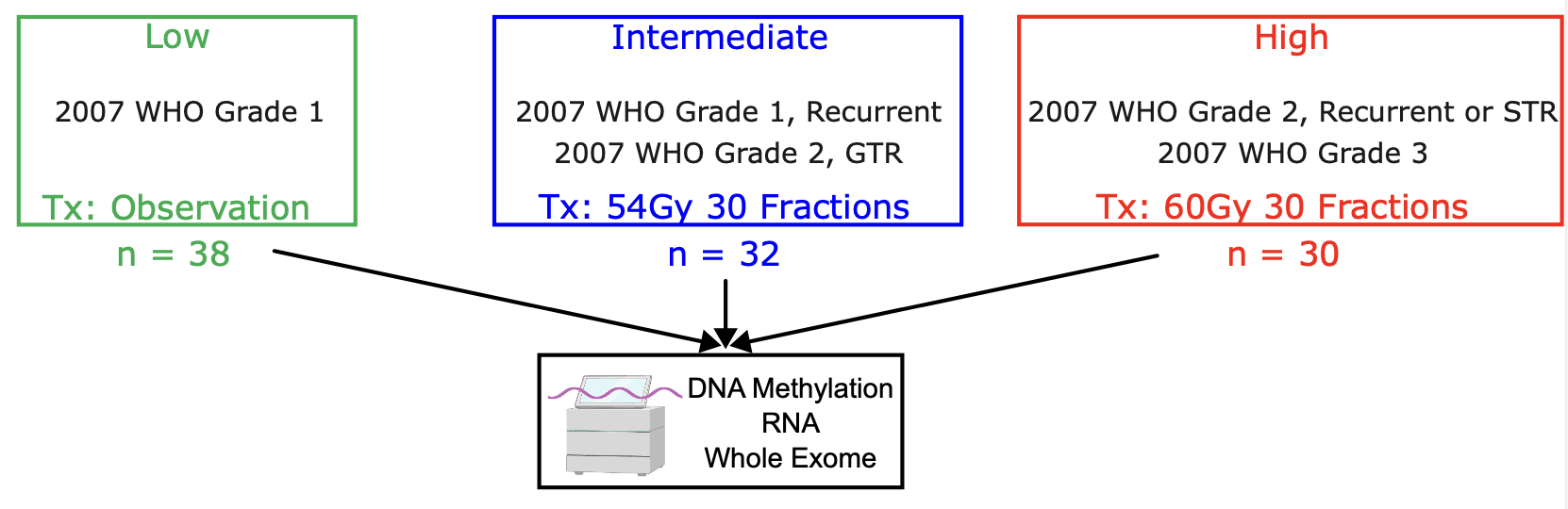
Figure 1: RTOG-0539 risk stratification schema and RT assignment
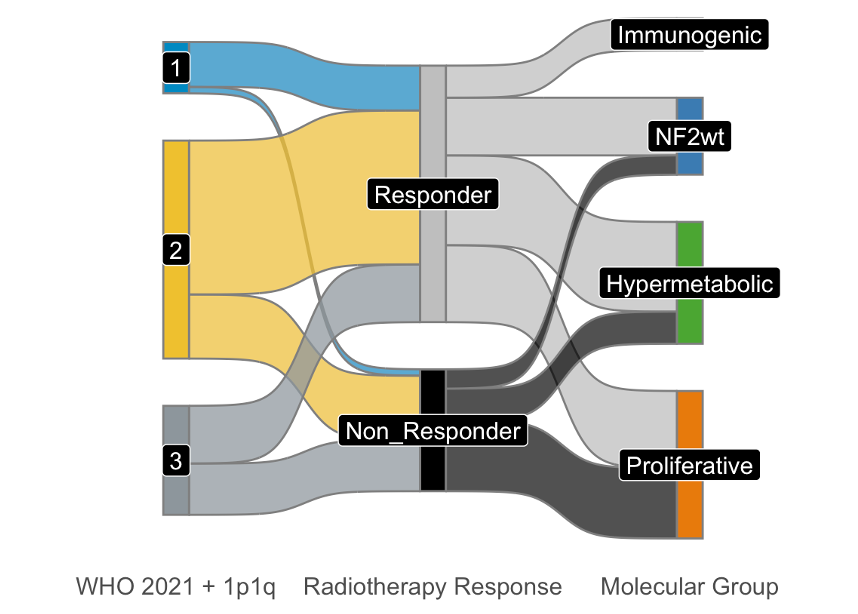
Figure 2: Distribution of WHO Grade and Molecular Groups by RT Response.
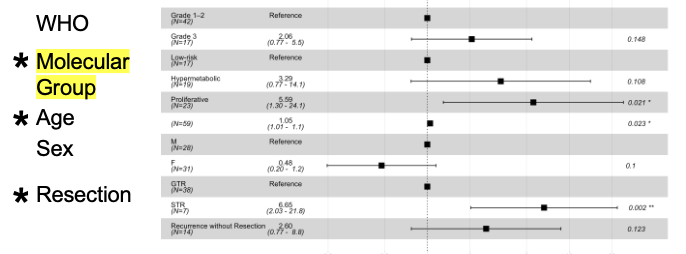
Figure 3: Multivariable analysis showing molecular group as an independent predictor of progression-free survival.
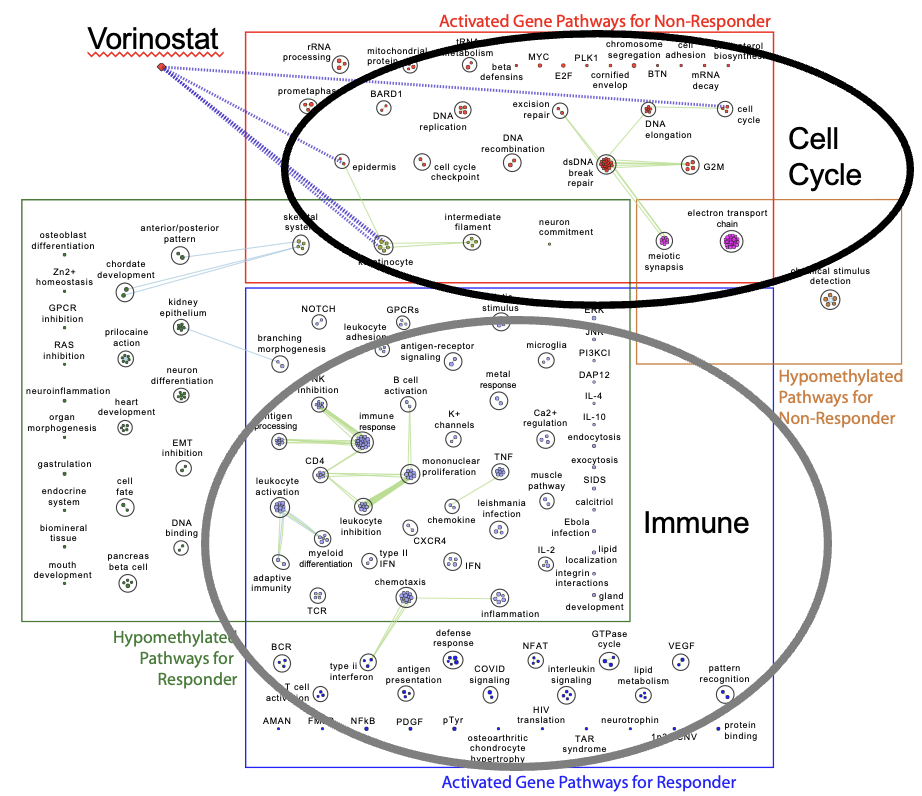
Figure 4: Cell cycle regulatory pathways enriched in RT non responders vs. immune pathways in responders. Non responder associated pathways susceptible to vorinostat.

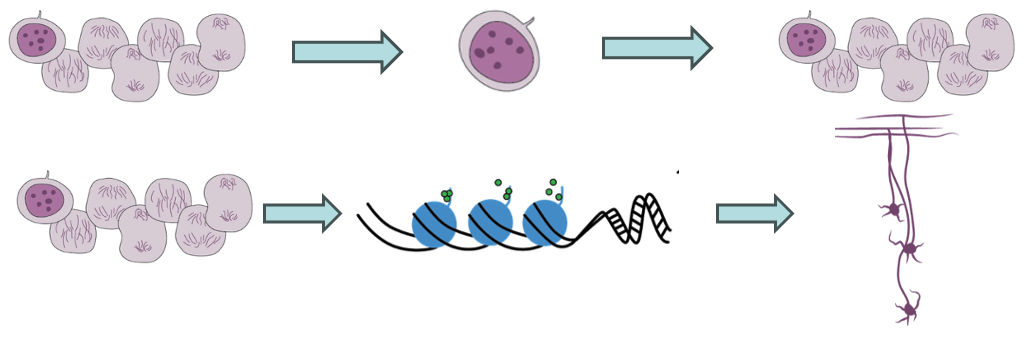
Figure 1: GNP differentiation and SHH-MB formation.
Treatment-resistant MB cells continually lead to tumor recurrence. Targeting cell cycle regulation can lead to neuronal differentiation of MB cells.
This study aims to evaluate the hypothesis that Cyclin D1 and Ezh2 are trapped within a negative feedback loop in dividing granule neuron precursors (GNPs) and medulloblastoma (MB) cells.
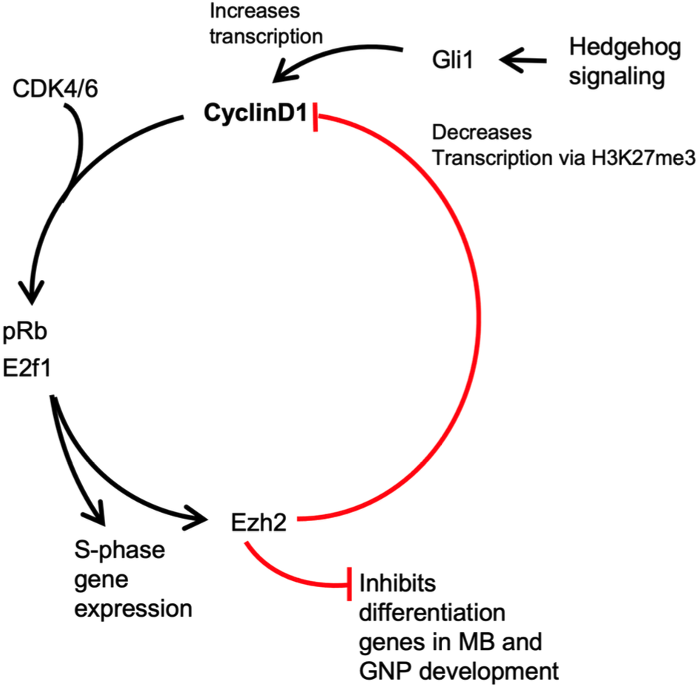
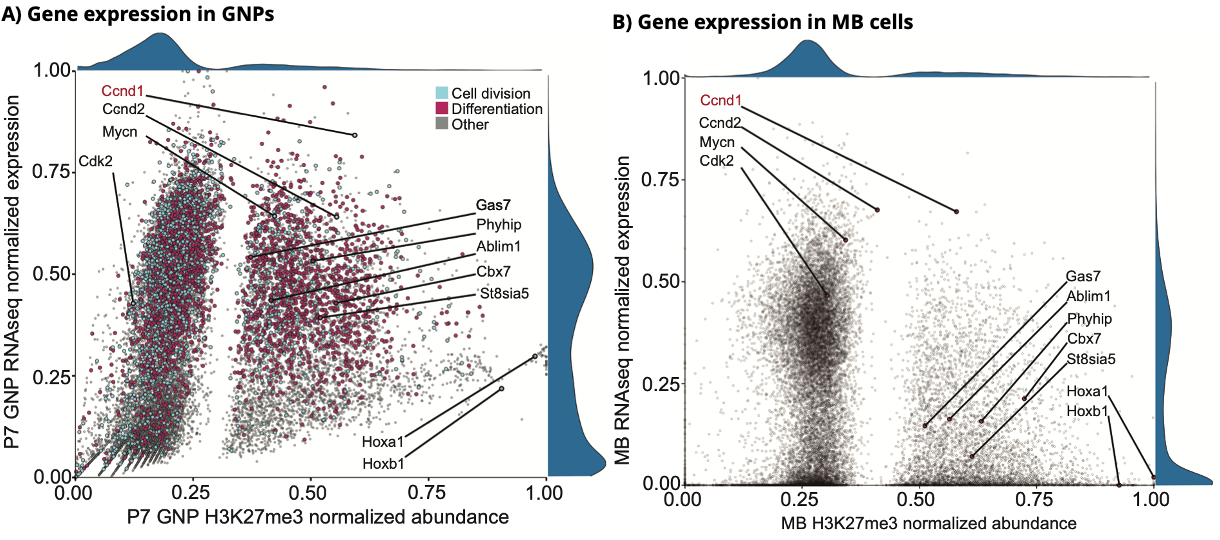
Figure 3: H3K27me3 levels were quantified at transcriptional start sites via ChipSeq and compared to RNASeq transcriptional expression levels in P7 GNPs (A) and MB cells (B). Paradoxically, Cyclin D1 was ranked in the top 11.21% of expressed genes while being heavily marked by the repressive histone mark H3K27me3 (top 7.58%) in GNPs. In MB cells, Ccnd1 was again found to be heavily marked by H3K27me3 and highly expressed (within the top 15.24% and 1.44%, respectively).
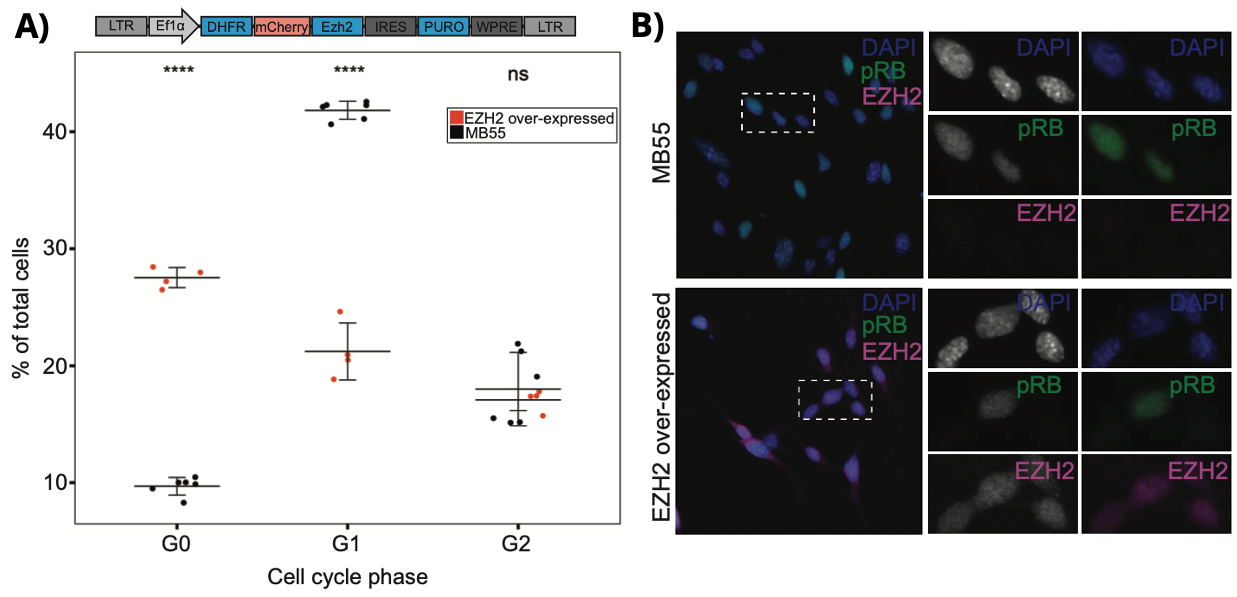
Figure 4: A stable MB cell line was created with an inducible degron construct that allows a TMP dose-dependent increase in EZH2 protein abundance. (A) Ezh2 overexpression at 10µM TMP resulted in a 2.7-fold increase in the proportion of G0-arrested cells relative to MB cells compared to wildtype cells (P<0.0001). (B) Immunofluorescent imaging of cell cultures from control (MB55) and Ezh2 over-expressed cells.
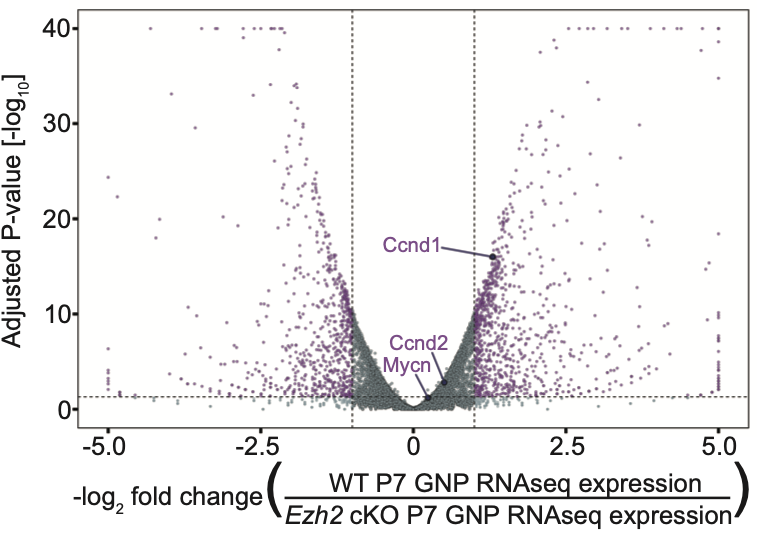
Figure 5: Differential gene analysis in GNPs following Ezh2 cKO. Significant changes are indicated with P ≤ 0.05 and log2FC ≥ 1. Ezh2 cKO GNPs had a significant increase in Cyclin D1 (Ccnd1) expression compared to Ezh2 wt mice (Log2FC: 1.301, Adjusted P-value: 16.001).
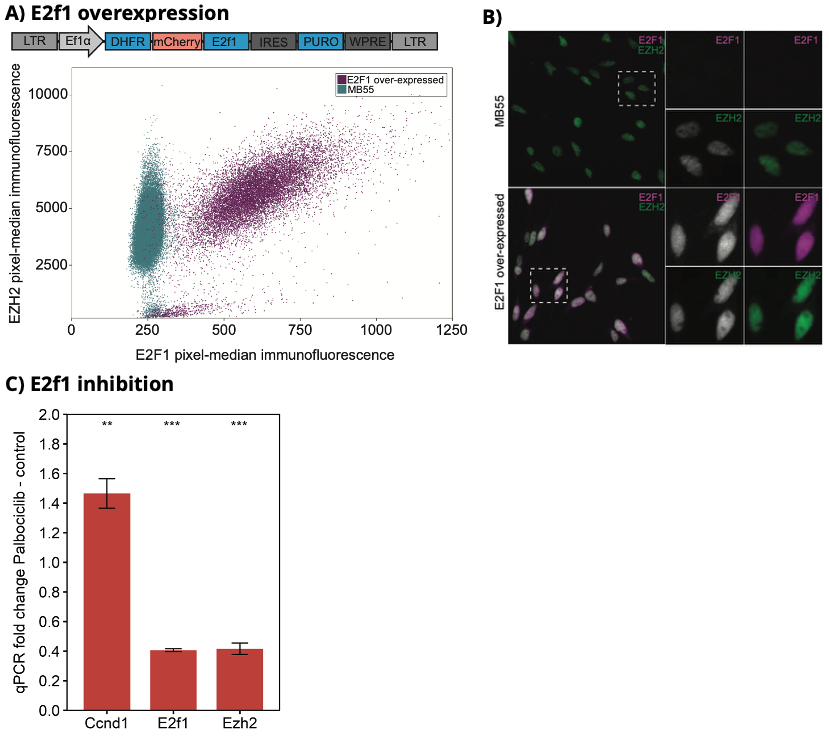
Figure 6: A stable MB cell line was created with an inducible degron construct that allows TMP dose-dependent increases in E2f1 protein abundance. (A) Increased E2f1 expression (TMP:10µM) demonstrated an increase in Ezh2 transcript and protein levels. (B) Immunofluorescence imaging of cell cultures from control (MB55) and E2f1 over-expressed MB cells. (C) The effect of decreased pRb/E2f1 activity on EZH2 expression via CDK4/6 inhibition. Treatment with Palbociclib resulted in a 58.4% decrease in EZH2 expression and a 46.5% increase in Cyclin D1 levels.
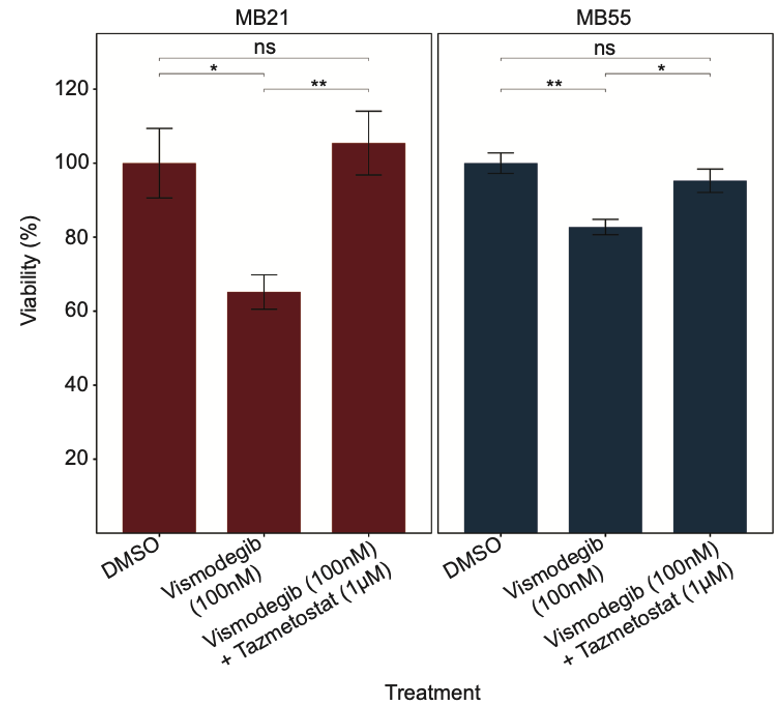
Figure 7: To test our model, SHH MB, which have constitutively active SHH signaling, were treated with Vismodegib, an inhibitor of the SHH pathway SMO. As expected, treatment with Vismodegib resulted in decreased cell viability relative to control (MB21: P-value<0.05; MB55: P-value<0.01). Addition of Ezh2 inhibitor Tazemetostat (1µM) resulted in a significant increase in cell viability compared to cells treated with Vismodegib alone (MB21: P-value<0.01; MB55: P-value<0.05).
Dermoid cysts are rare, benign intracranial lesions arising from abnormal folding of the neuroectoderm during embryogenesis, sequestering mesenchymal and ectodermal cells. Classically occuring in the midline, near the sella or in the posterior fossa, we report a case of an intracranial dermoid cyst presenting along the left supratentorial convexity with extension into the sylvian fissure.
A 33-year-old female presented following a three-year history of intermittent paresthesia’s involving the right side of her face and her right hand lasting approximately 1 minute, occurring with increasing frequency the month prior to presentation. A non-contrast head CT was performed which revealed a 4.7cm hypodense lesion with peripheral calcification contiguous with the calvarium. MRI was performed revealing a 4.3 x 3.4 x.4.8cm extra-axial, pre-dominantly cystic, T2-hyperintense, T1-hypointense lesion with internal septations. Post-contrast imaging revealed enhancement of the internal septation and thin linear peripheral enhancement.
The patient underwent left fronto-temporal craniotomy and resection of the mass. A small craniectomy was performed to detach the central calcified portion contiguous with the calvarium. Intra-operatively, the lesion had a soft consistency with a distinct plane separating it from the underlying parenchyma. Intralesional hair was seen, concerning for a dermoid cyst. The mass was debulked with ultrasonic aspiration and GTR was achieved. The patient recovered well post-operatively, with complete resolution of her paresthesias.
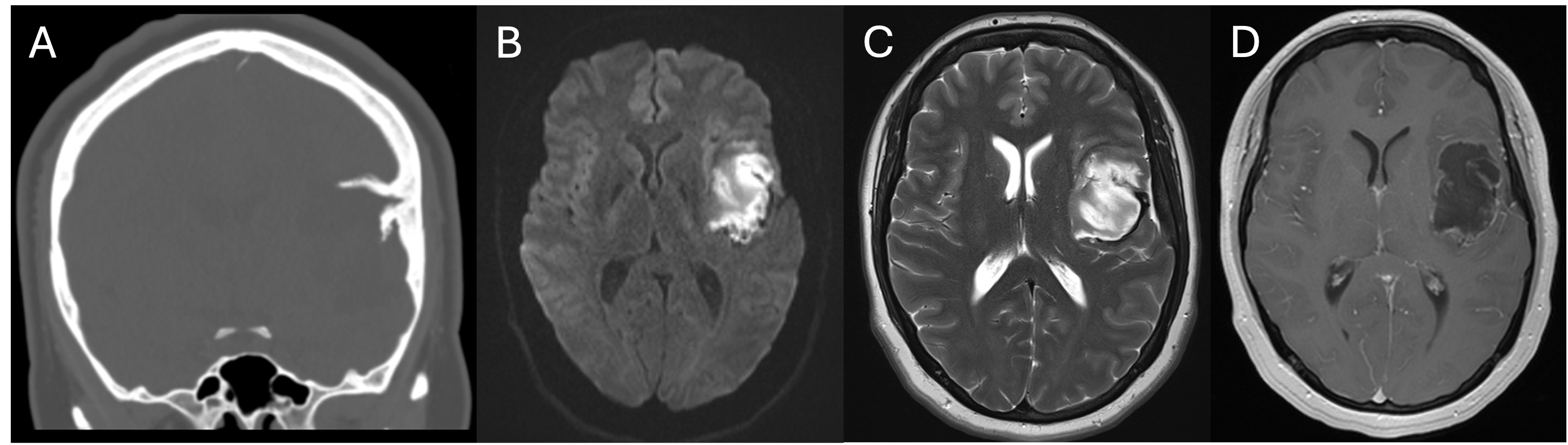
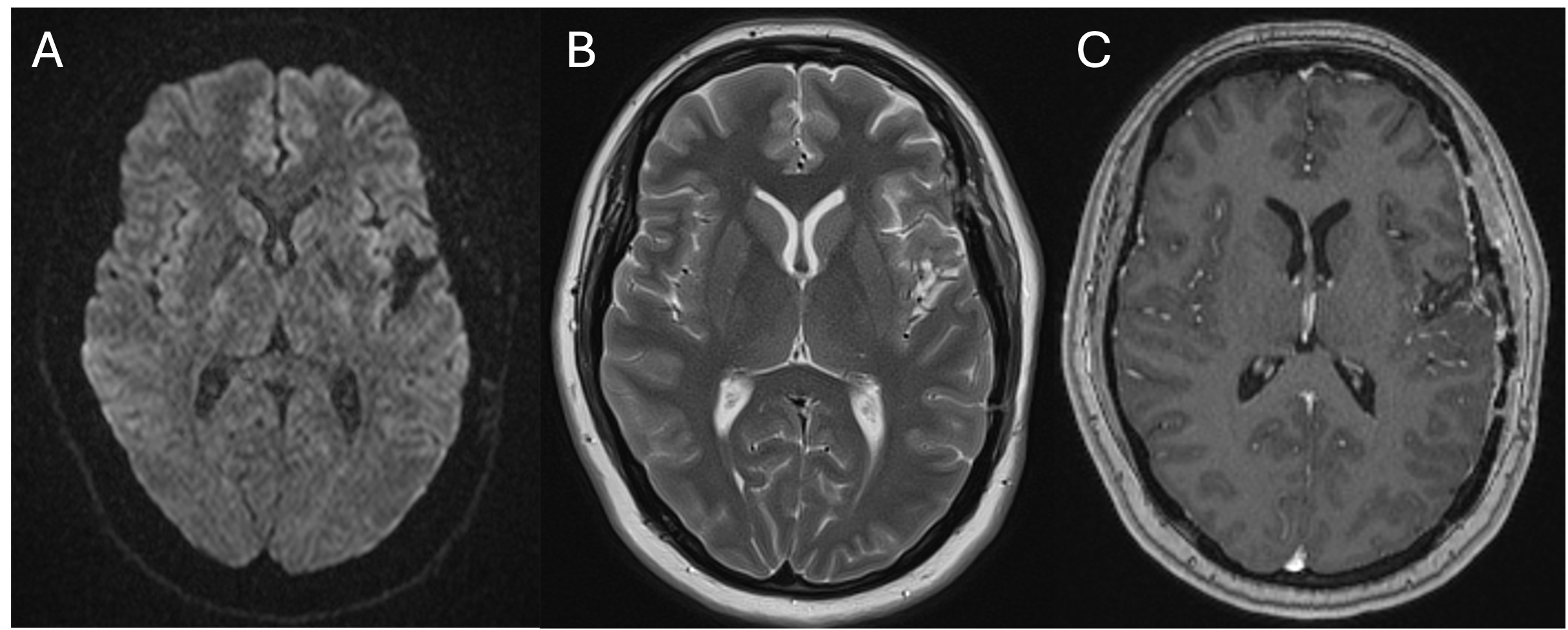
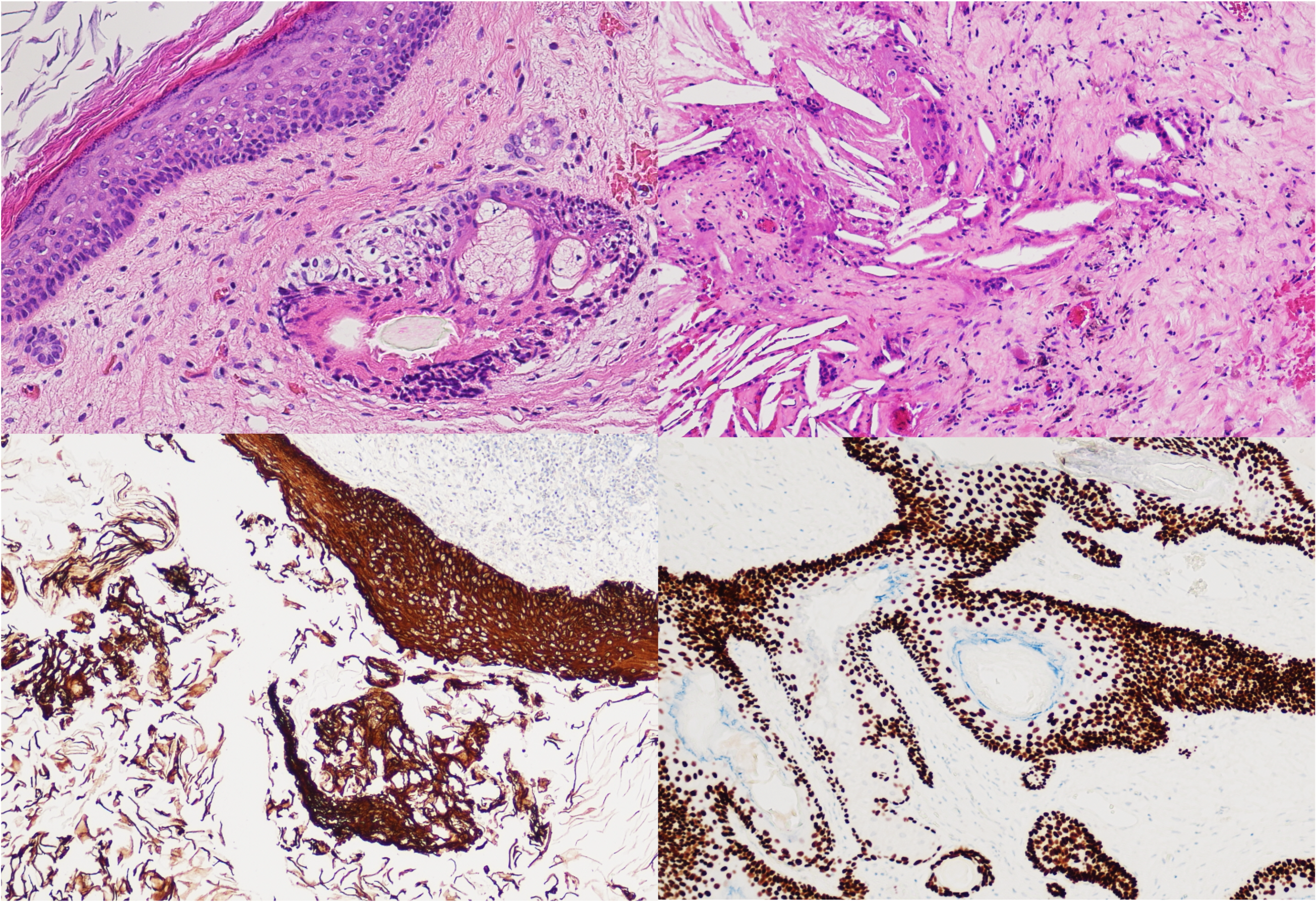
1. Lunardi P, et al. (1989) Chemical meningitis in ruptured intracranial dermoid. Case report and review of the literature. Surg Neurol 32:449–452.
2. Shehadi JA, et al. (1999) Temporal dermoid cyst with a partial dermal sinus tract. Canadian Journal of Neurological Sciences 26:321–324.
3. Barkley AS, et al. (2019) Frontotemporal Dermal Sinus Tract with 2 Connected Intradiploic Dermoid Cysts: A Rare Case and Review of the Literature. World Neurosurg 127:350–353.
4. Abbas S, et al. (2024) Dermoid cyst, unusual location of the pterion: About a case and review of literature. Radiol Case Rep 19:863–866.
5. Anand D, et al. (2014) Sylvian fissure dermoid cyst -A rare case. Journal of Clinical and Diagnostic Research 8:RD01–RD02.
6. Haider AS, et al. (2016) A Nonoperative Approach for Neurosurgical Management of a Sylvian Fissure Dermoid Cyst. Cureus 8:.
7. Obled L, et al. (2020) Rare Case of Giant Supratentorial Dermoid Cyst. World Neurosurg 135:72–75.
8. Mishra MK, et al. (2023) Intracranial Interdural and Extradural Cerebellar Convexity Dermoid Cyst: A Case Report of Rare Tumor at the Rarest Location. Asian J Neurosurg 18:631–635.
Acute ischemic stroke remains a significant cause of morbidity and mortality in Canada. Following the publication of several landmark clinical trials in 2015, mechanical thrombectomy has become the standard of care for eligible patients with large vessel occlusions (LVOs). However, there remains significant variability in the anesthetic strategy employed during thrombectomy. The primary objective of this study was to determine whether anesthetic strategy (conscious sedation vs. general anesthesia) affects key procedural metrics, functional outcomes, and safety in patients undergoing thrombectomy.
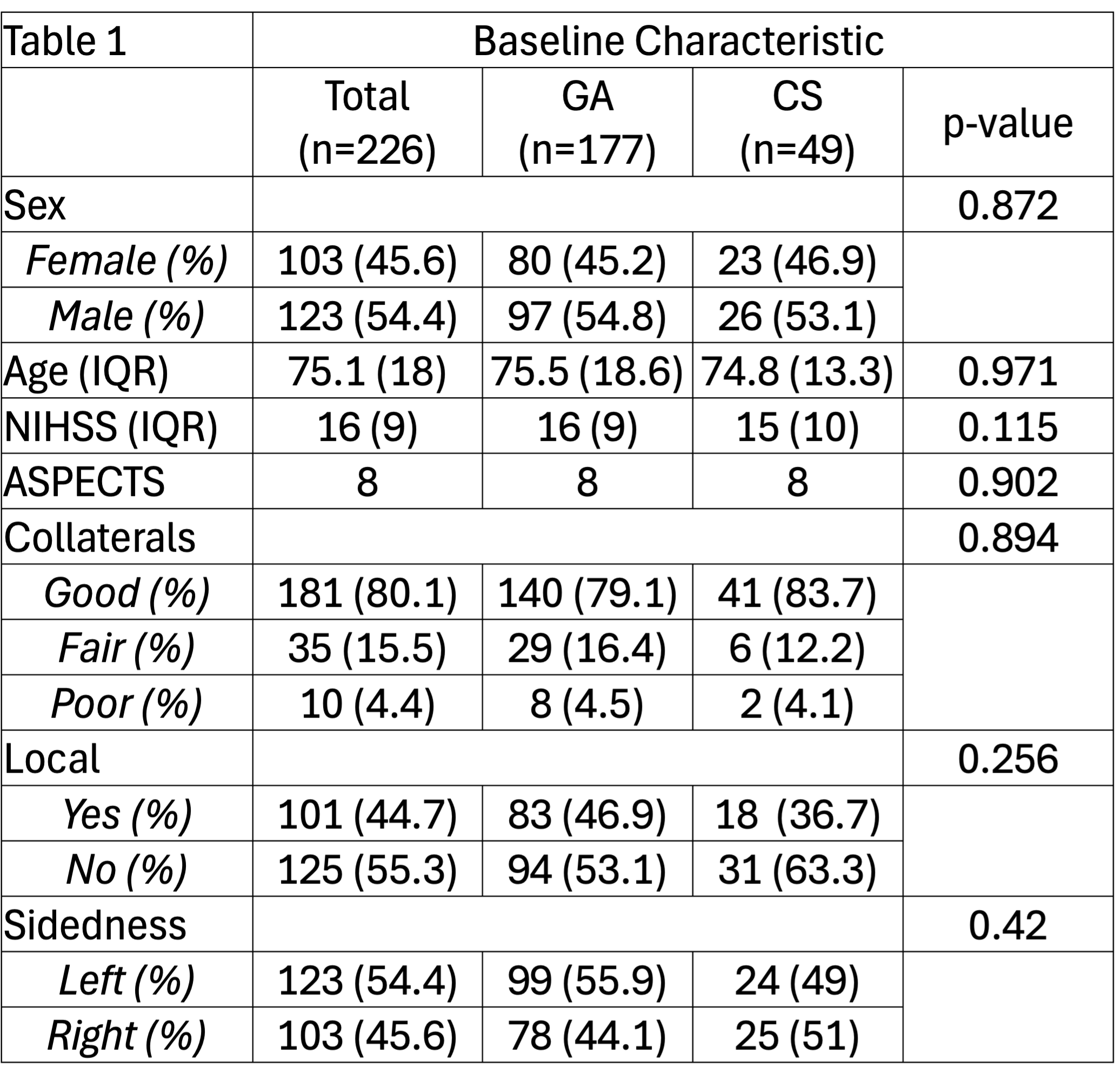
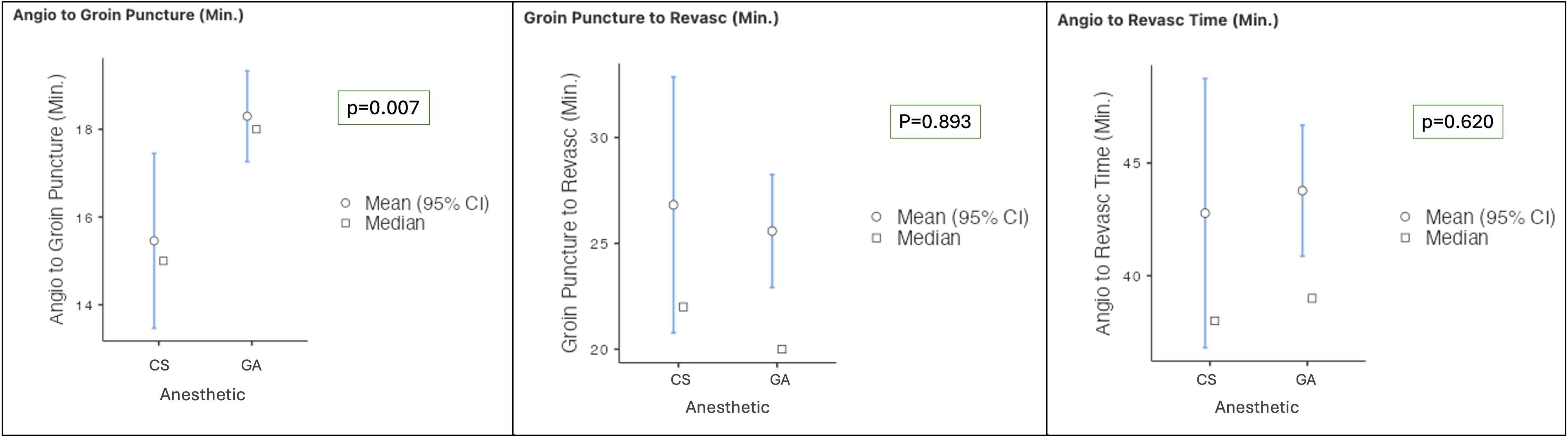
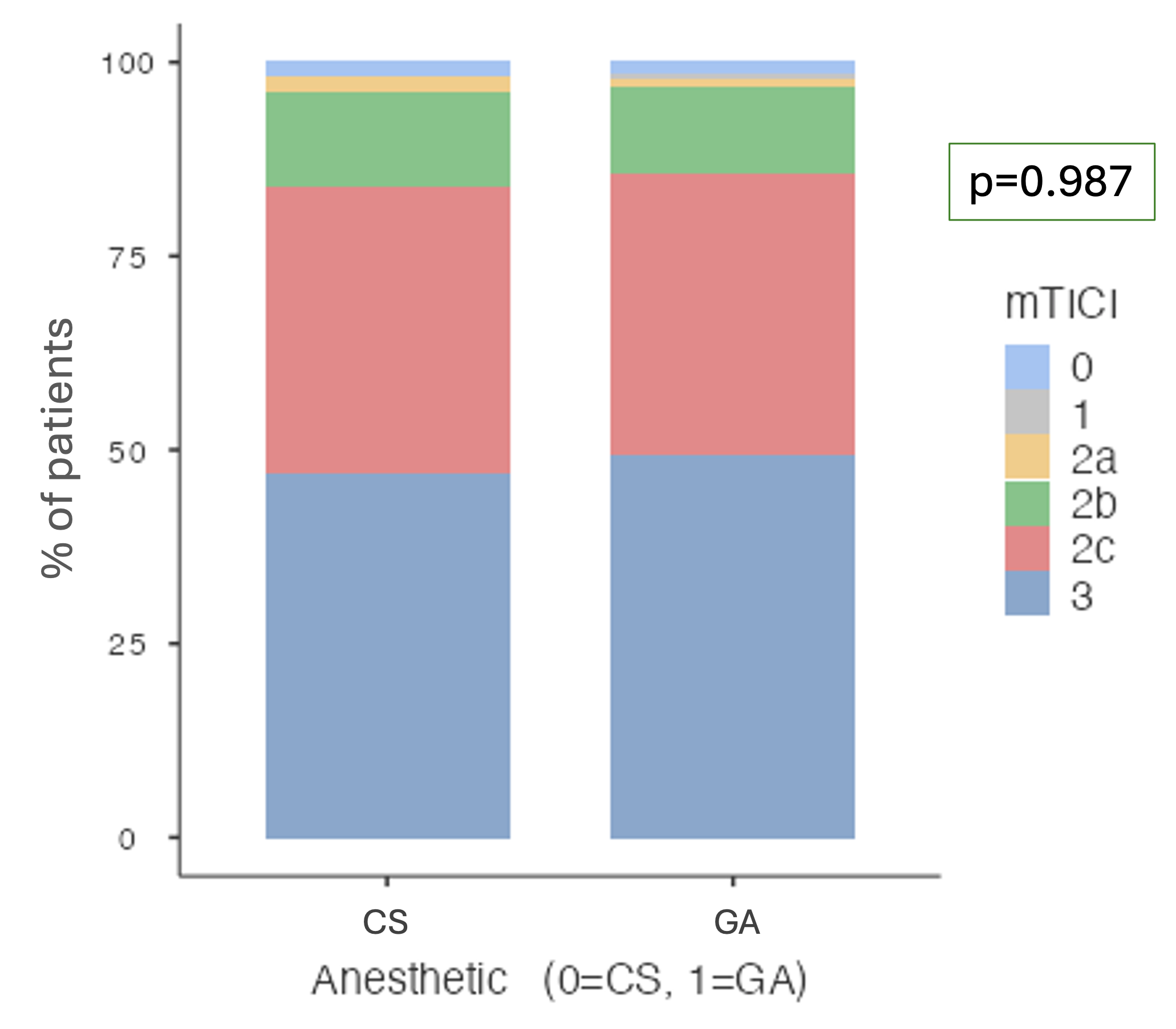
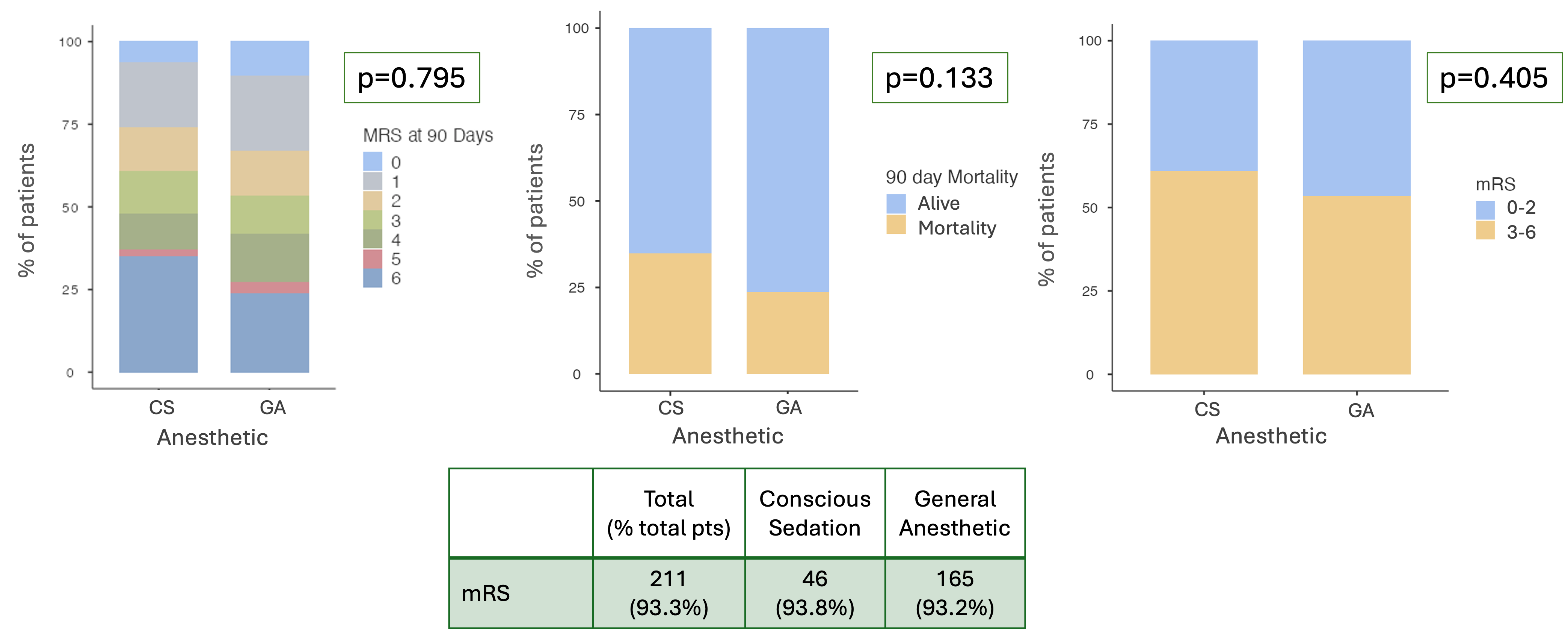
- MR CLEAN https://www.nejm.org/doi/full/10.1056/NEJMoa1411587
- ESCAPE https://www.nejm.org/doi/full/10.1056/NEJMoa1414905
- REVASCAT https://www.nejm.org/doi/full/10.1056/NEJMoa1503780
- SWIFT PRIME https://www.nejm.org/doi/full/10.1056/NEJMoa1415061
- EXTEND-IA https://www.nejm.org/doi/full/10.1056/NEJMoa1414792
- Brinjikji W et al. PMID: 25395655; PMCID: PMC8013063.
- Jing et al 2018. https://pmc.ncbi.nlm.nih.gov/articles/PMC5896359/
- Campbell et al 2023. https://www.neurology.org/doi/10.1212/WNL.0000000000207066
- Lee et al 2022. https://pubmed.ncbi.nlm.nih.gov/36188372/
- Tosello et al. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD013690.pub2/full
- Schonenberger et al, 2016. SIESTA. https://pubmed.ncbi.nlm.nih.gov/27785516/
- Sorensen et al 2019. GOLIATH. https://pubmed.ncbi.nlm.nih.gov/30926686/
- Henden et al 2017. AnStroke. https://www.ahajournals.org/doi/10.1161/STROKEAHA.117.016554?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed

Methods
Results
•Baseline Characteristics
|
Number |
Variable |
|
750 |
Total Number of Patients (N) |
|
9 (1.13%) |
Early Postoperative Visual Deterioration (n, %) |
|
52.14 |
Mean Age (years) |
|
03:42 |
Mean Operative Length (hrs:mins) |
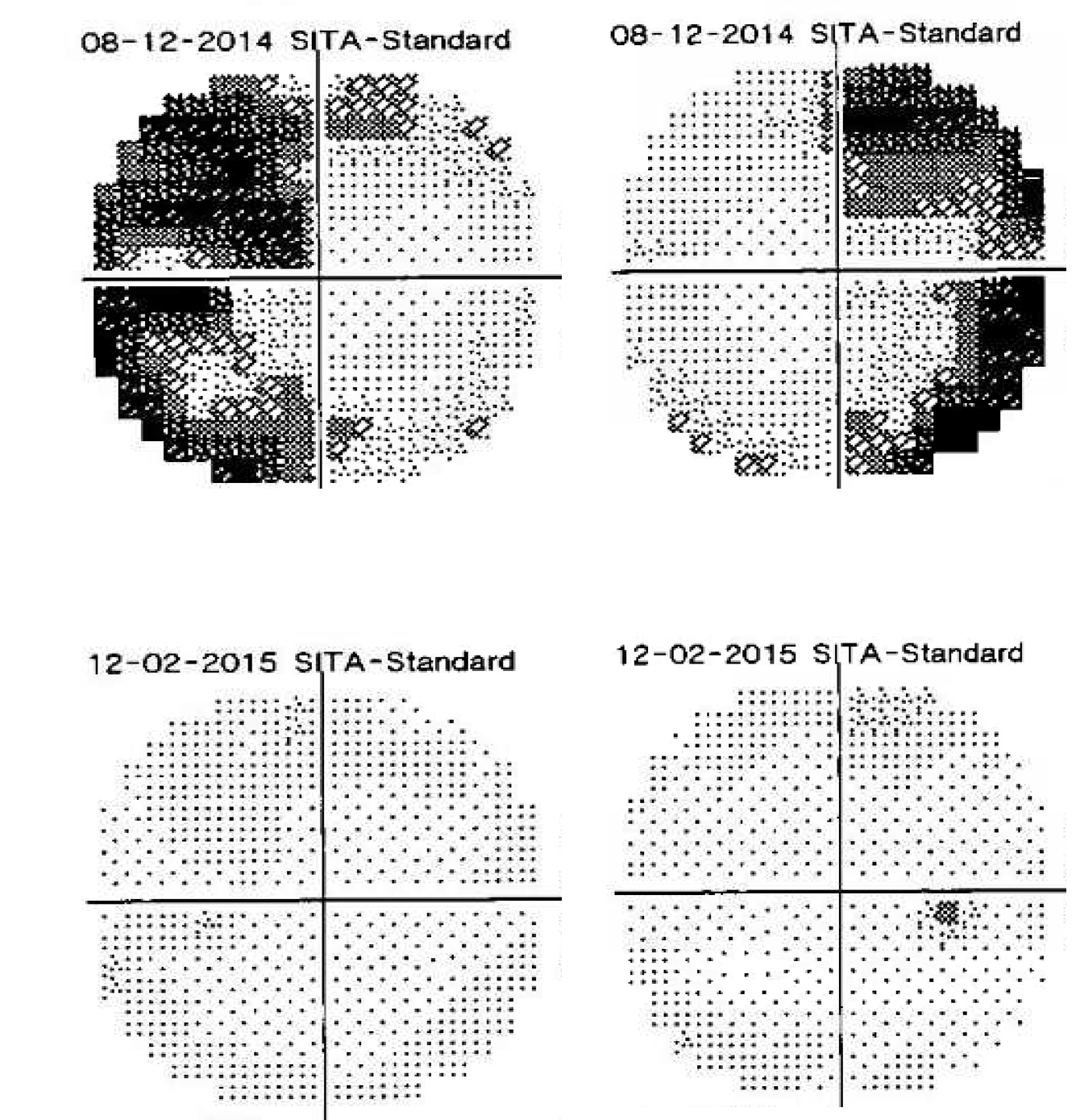

BACKGROUND:
Olfactory groove meningiomas (OGMs) comprising 13% of intracranial meningiomas. OGMs are slow-growing tumors often going undetected until reaching Giant size. These tumors can cause a variety of symptoms, including headaches, personality changes, insomnia, and visual deterioration. A little is known about the visual recovery and prediction of recurrence of giant olfactory groove meningioma patients.
This is A retrospective study conducted at a major medical center. This study included all the patients with Giant olfactory meningioma (more than 6 cm in diameter) who underwent surgery over a 22-year period (January 2000 to December 2022). Long-term outcome including visual status, recurrence and functional status were collected. Multivariable logistic regression was used to identify predictors of recurrence and functional outcome.
RESULTS:
Thirty-two patients met the inclusion criteria for this study, with a mean age of 55.8 years.The mean follow-up period was 62 months. The majority of giant OGMs were classified as WHO grade 1 (84.4%). Postoperatively, 19 patients demonstrated improvement in visual acuity and visual field deficits. Radiological recurrence was observed in nine patients (28.1%) at a mean follow-up of 56 months, with only three requiring reoperations for tumor resection. One patient developed a brain abscess, necessitating reoperation. Multivariable analysis identified patient age, Simpson grade of excision, and WHO grade as significant predictors of recurrence rate.
CONCLUSIONS:
This study demonstrates that surgery can improve visual deficits and functional outcomes. Postoperative outcomes were strongly predicted by age, resection extent, and histological grade. Developing a new predictive scale based on these parameters appears to strongly predict the Giant OGMs Long-Term outcome.
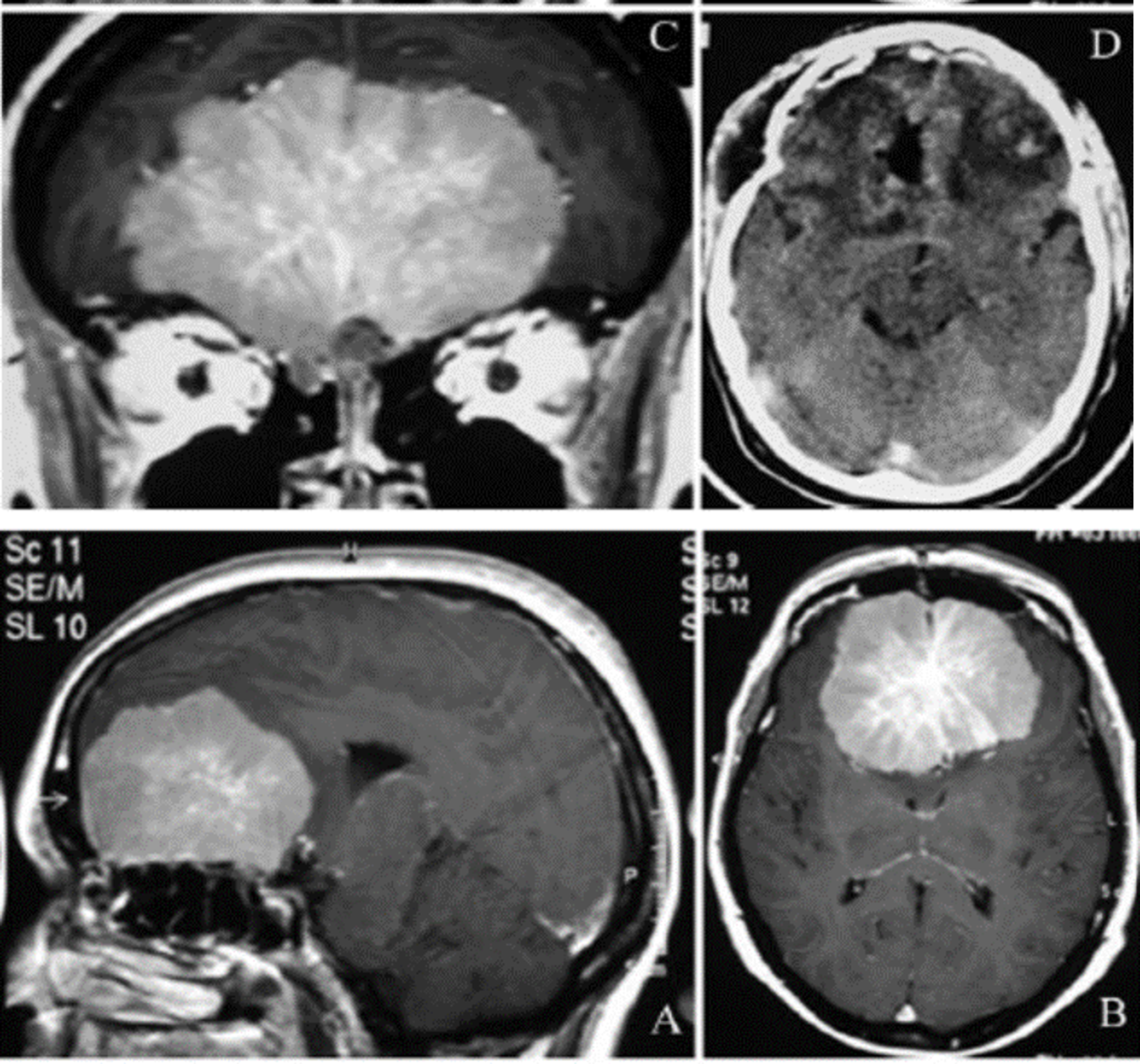
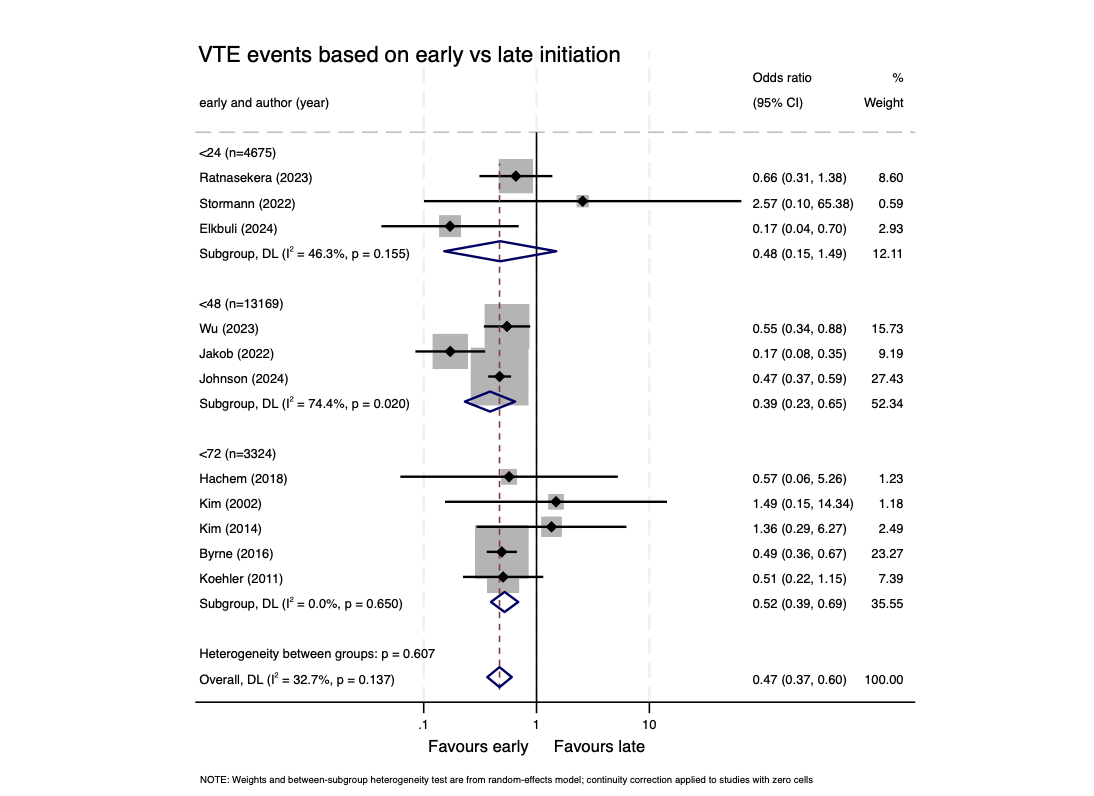
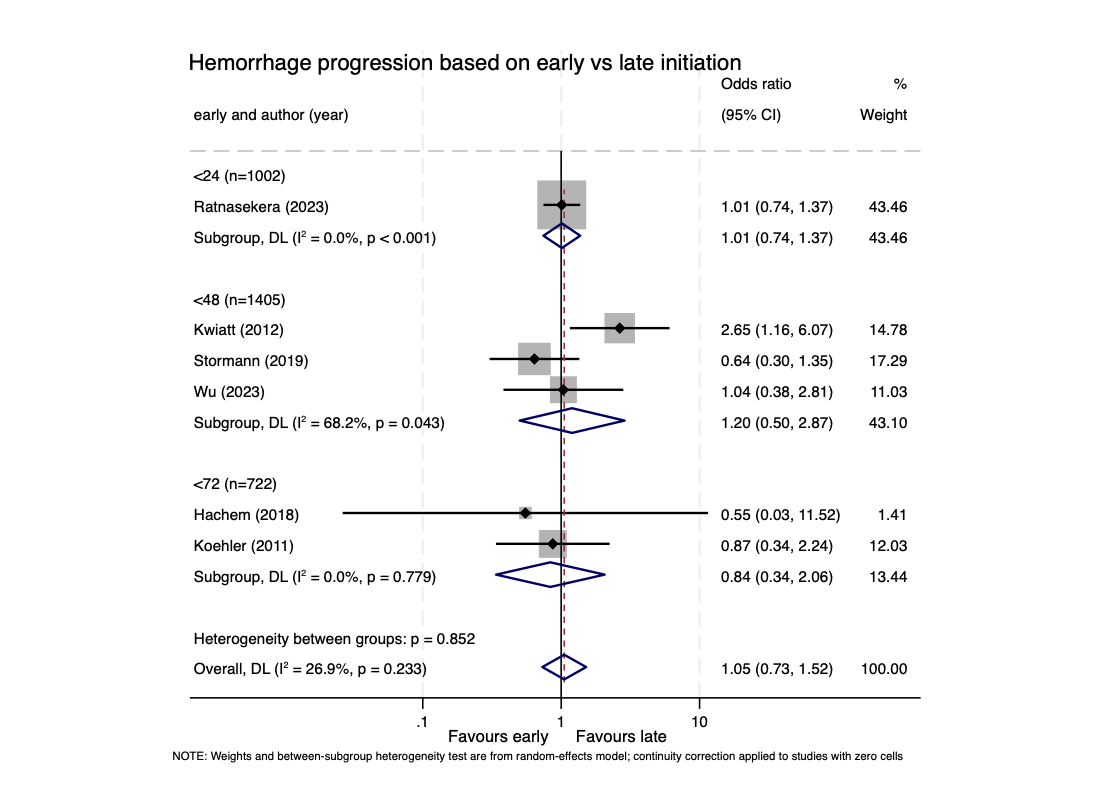
Odds ratios of intracranial hemorrhage progression following cVTEp initiation, stratified by timing
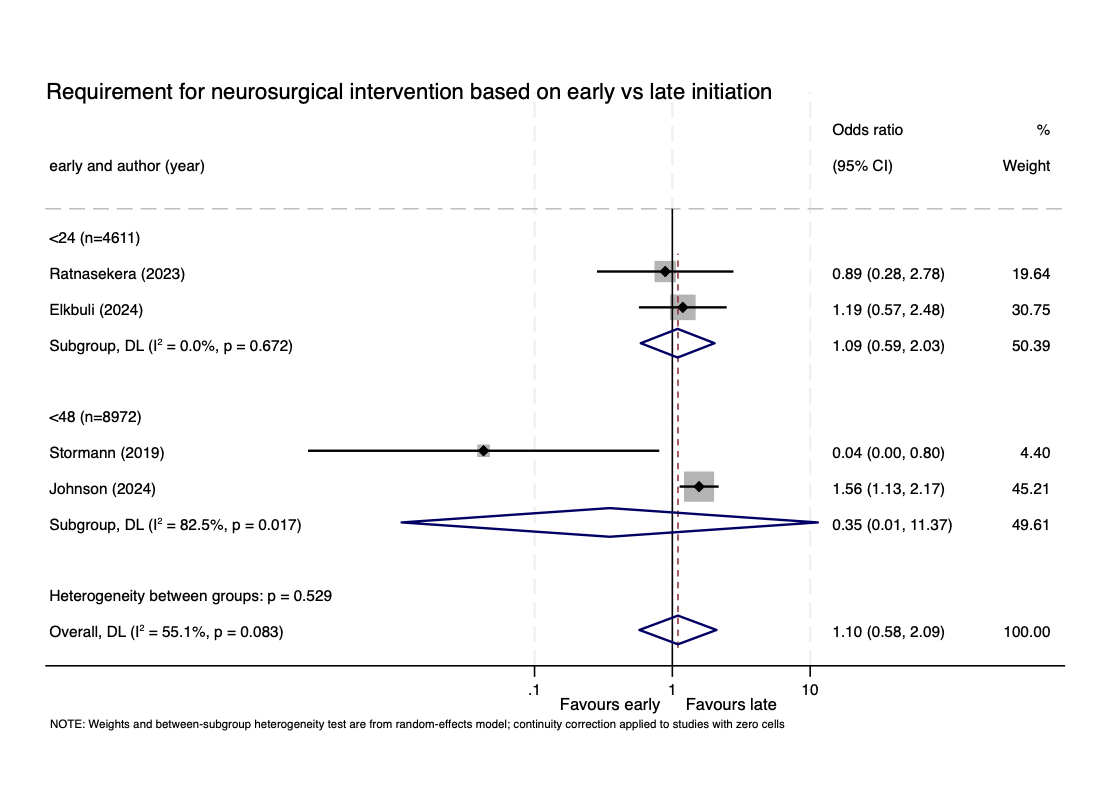
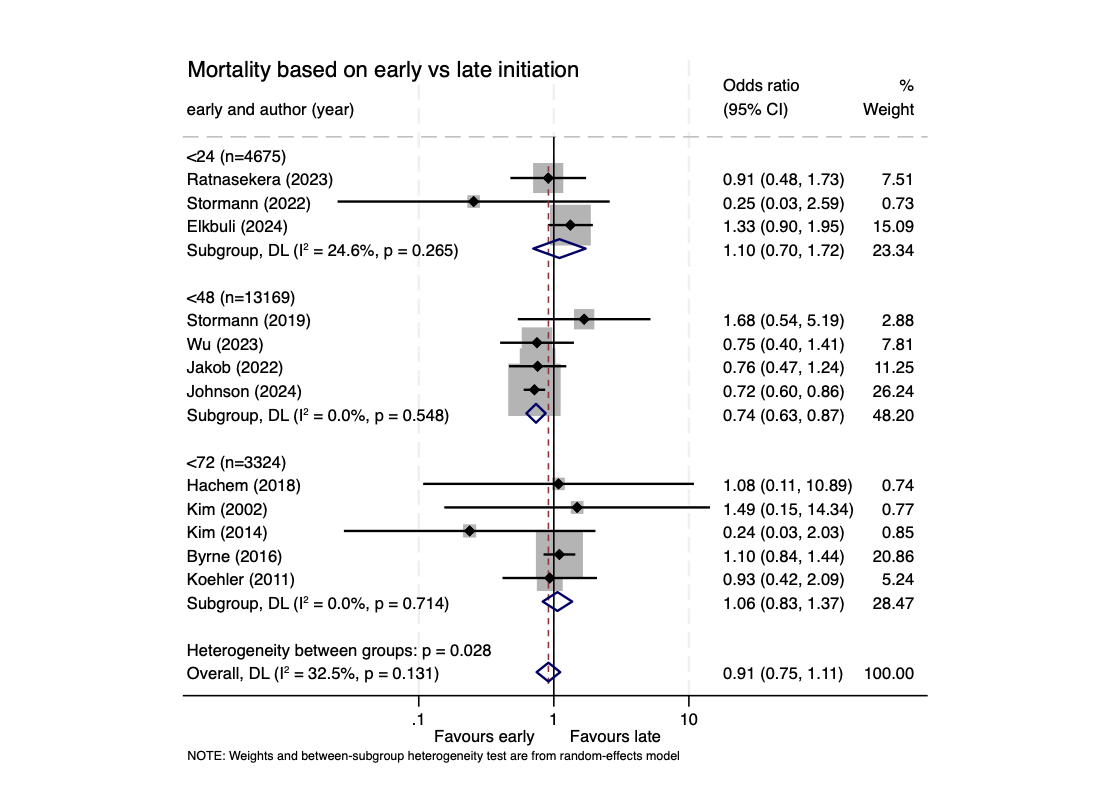

Computed tomography (CT) head scan within 24 hours of brain surgery (i.e., craniotomies) is used:
Given that postoperative brain imaging practices are variable:
Retrospective review of postoperative CT head use:
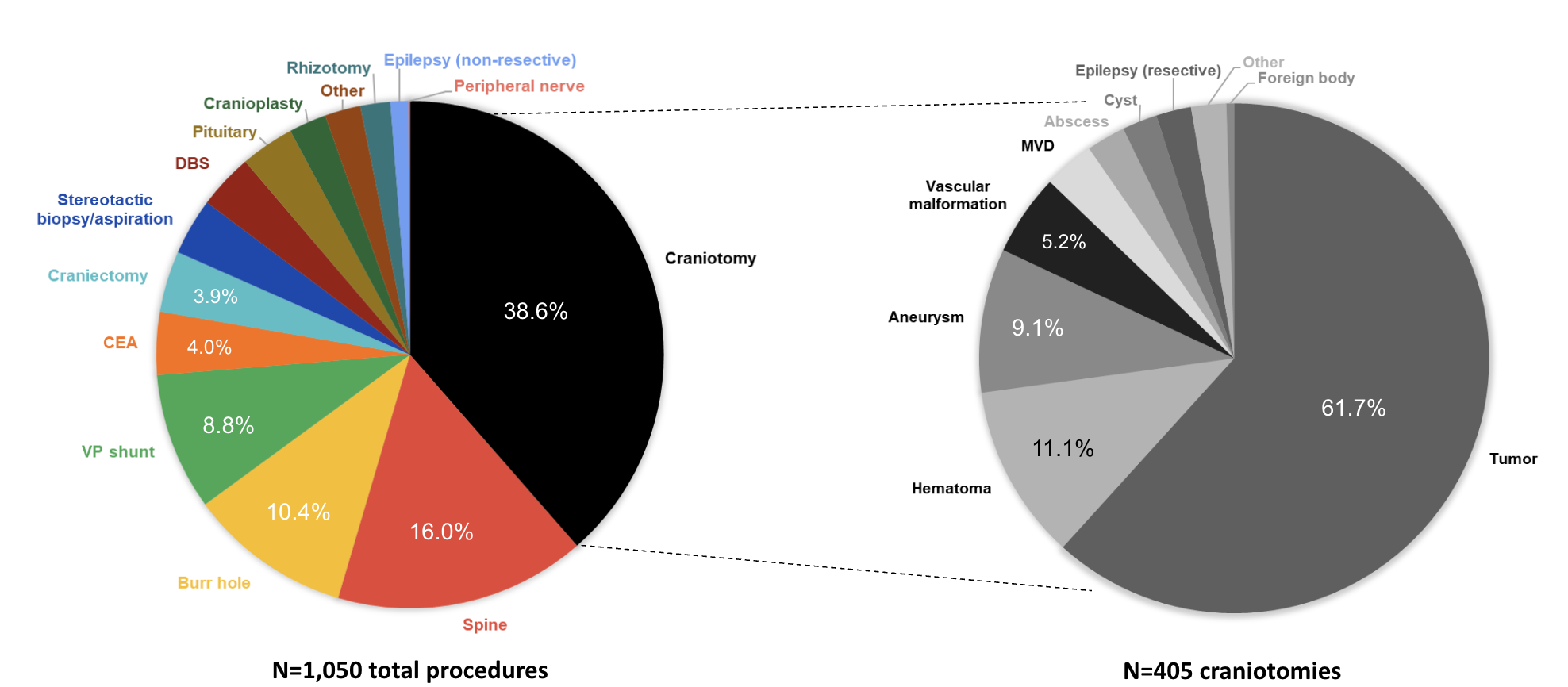
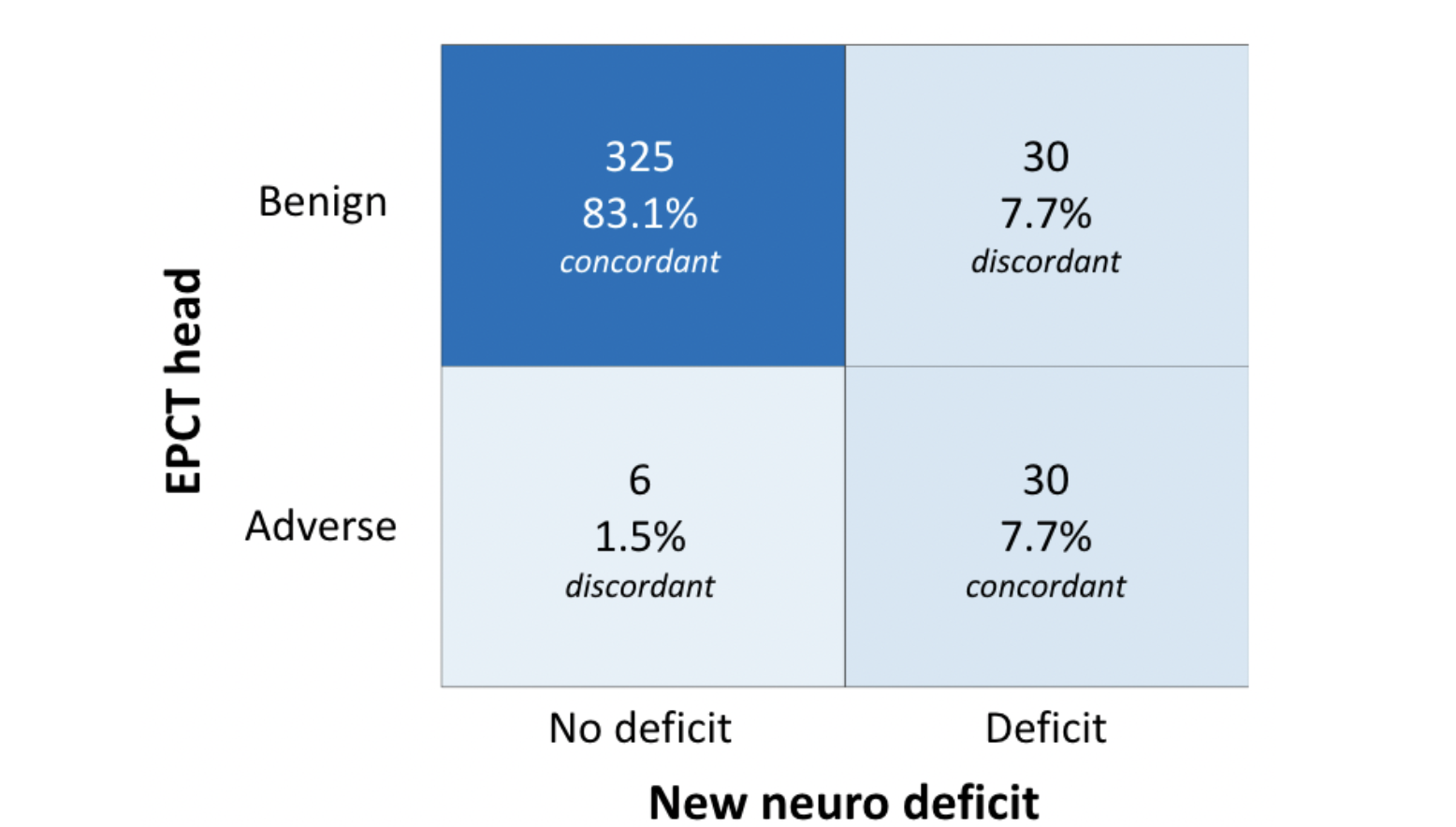
Figure 2. Contingency table of EPCT head vs. new neuro deficits. 36/391 (9.2%) patients had radiological changes on EPCT (e.g., bleeding, extensive pneumocephalus, edema, ischemia). 60/391 (15.3%) patients had neurologic deterioration on clinical exam (e.g., weakness, aphasia, visual impairment, seizure, decreased LOC, CN palsy). Radiological changes on EPCT correlate with new neuro deficits, X2 (1, N=391) = 141.1, p = 1.54e-32.
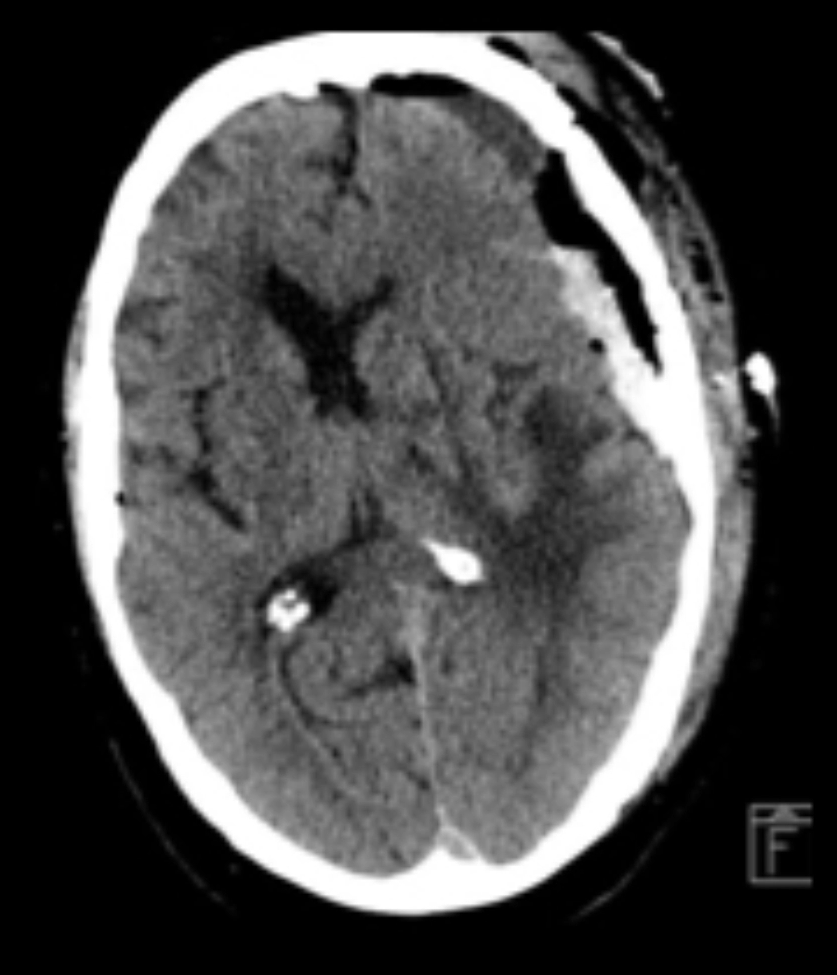
Figure 3. Example of a patient with adverse EPCT findings: Left subdural hematoma identified in the absence of new neurological deficits managed with surgical evacuation.

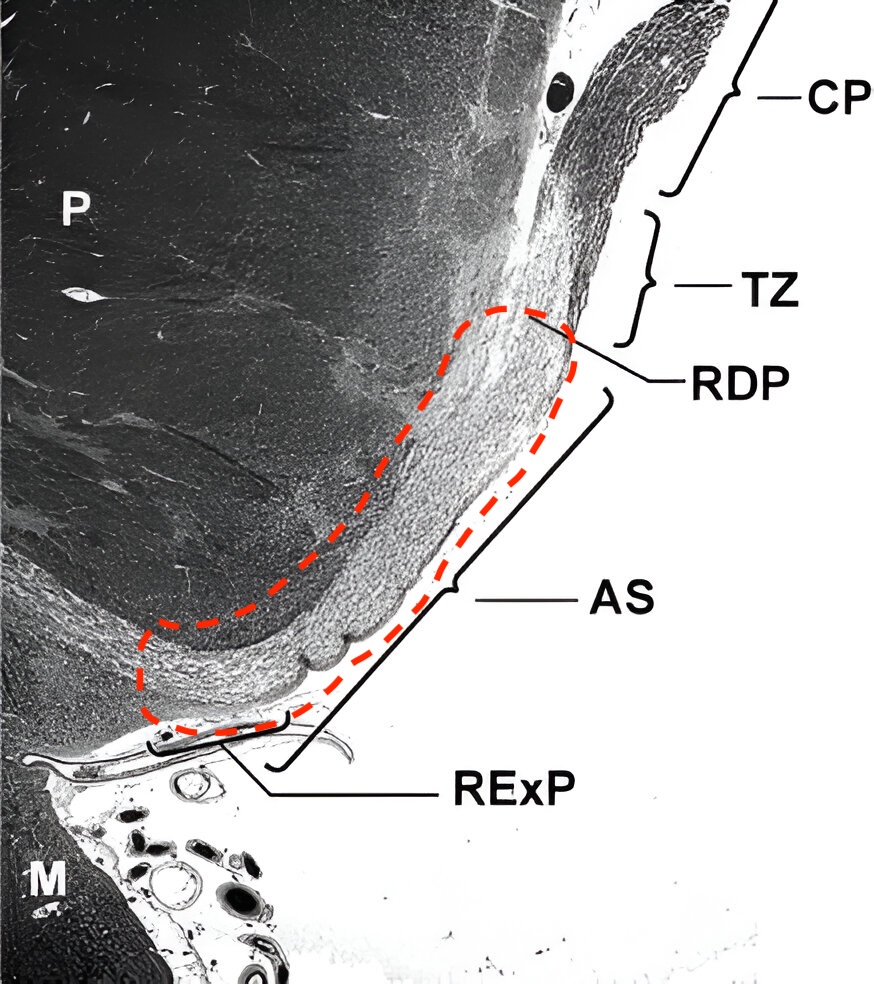
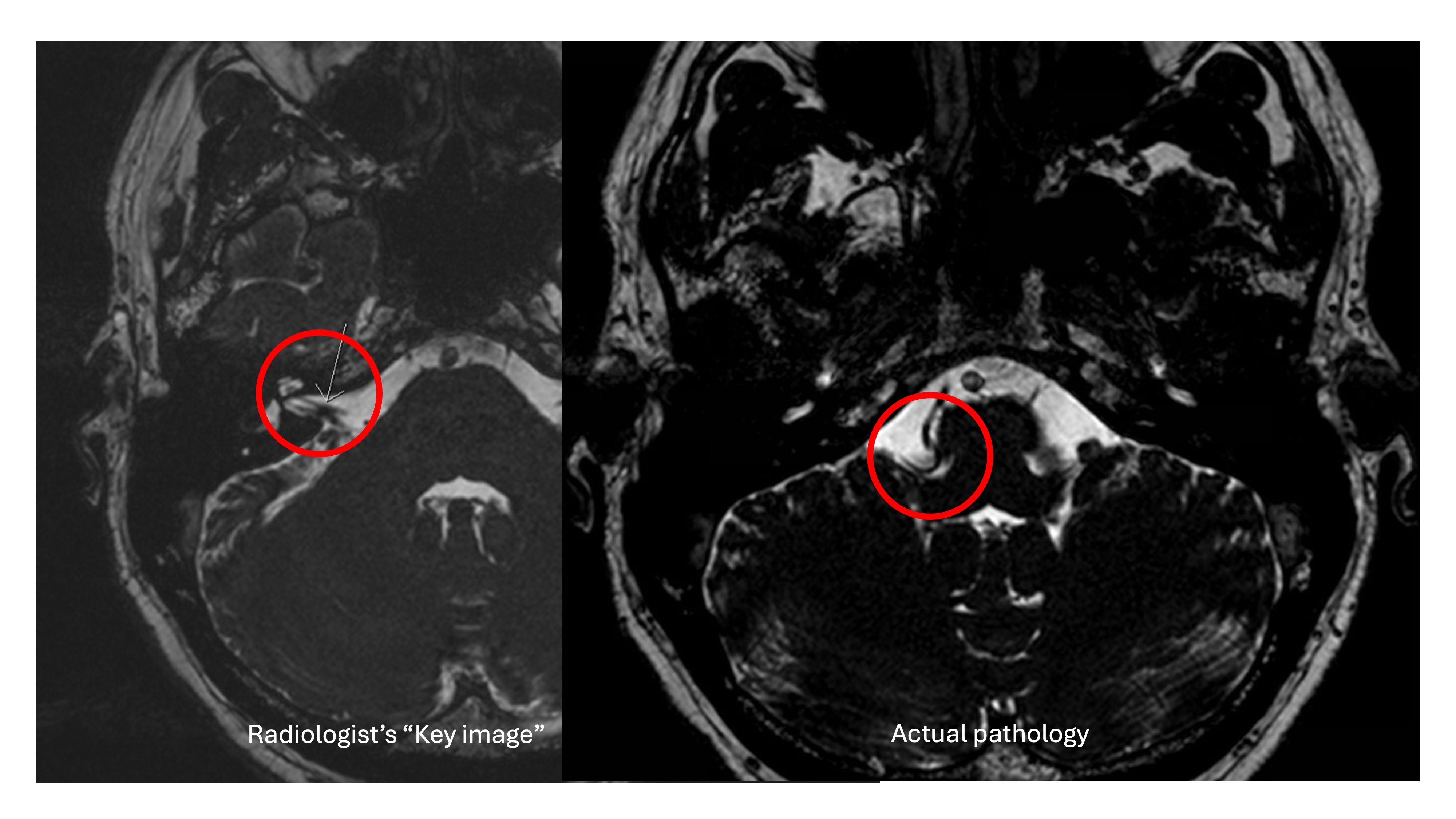
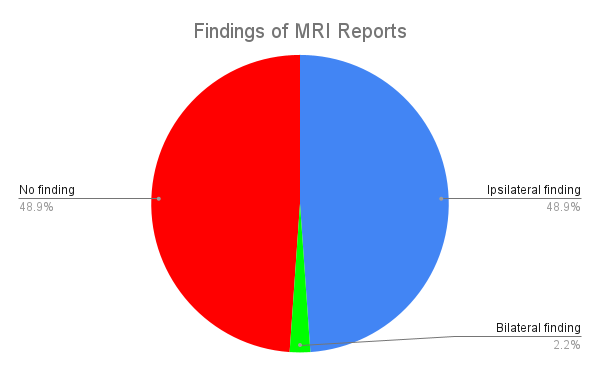
Examples of (A) skull base angle and (B) modified skull base angle
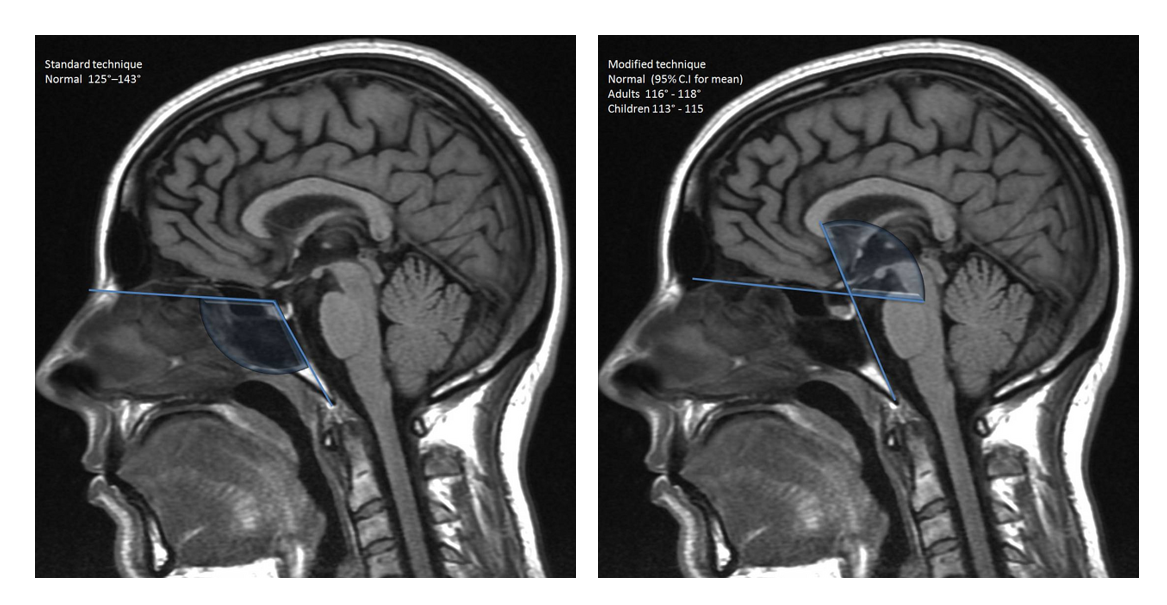
| Number of included patients | 48 |
| Number of female patients (%) | 22 (50) |
| Etiology of hydrocephlus | |
| Post-infectious (%) | 3 (6.3) |
| IVH (%) | 5 (10.4) |
| Non-tectal tumour (%) | 3 (6.3) |
| Aqueductal stenosis (%) | 21 (43.8) |
| Tectal tumour (%) | 8 (16.7) |
| Other (%) | 8 (16.7) |
| Mean ETV Success Score | 76.7 |
Statistical comparison of clinical and radiologic measures between patients with successful and failed ETV. Students’ t-test for parametric data and Mann-Whitney U test for non-parametric data. *-p<0.05, **p<0.01
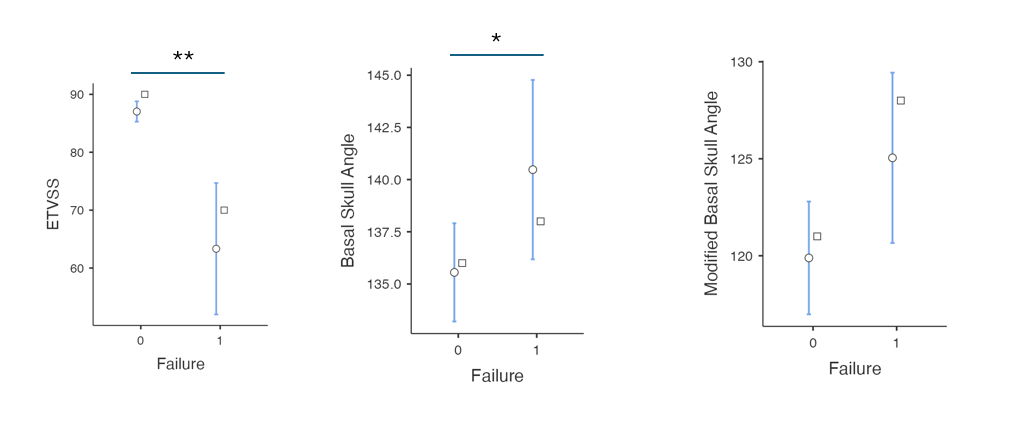
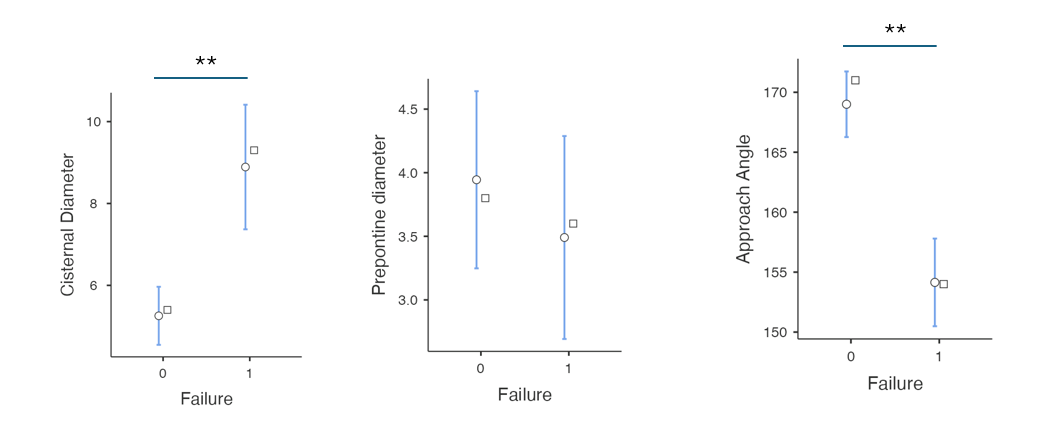
| Patients | ETV Success (n=27) | ETV Failure (n = 21) |
| Mean age | 46.9 | 24.4 |
| # Female | 14 | 8 |
| Etiology of hydrocephalus | ||
| Post-infectious | 0 | 3 |
| IVH | 0 | 5 |
| Non-tectal tumour | 2 | 1 |
| Aqueductal stenosis | 14 | 7 |
| Tectal tumour | 7 | 1 |
| Other | 4 | 4 |
| Mean ETV Score | 87.4 | 62.9 |

1) To understand the status of quality of life, burnout, and well-being in Canadian neurosurgical residents.
2) To assess whether implementation of a weekly self-assessment tool improves neurosurgical resident quality of life.
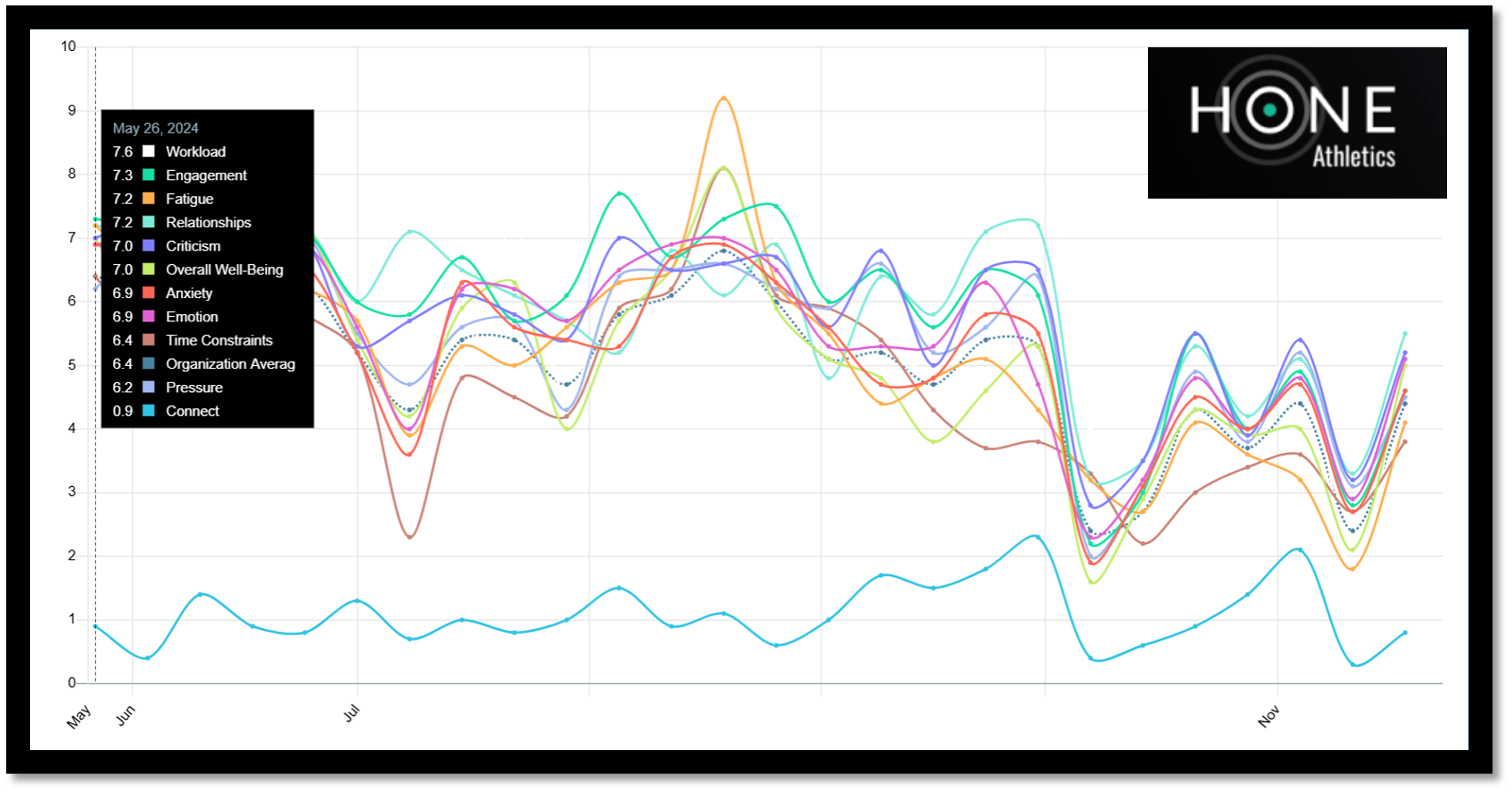
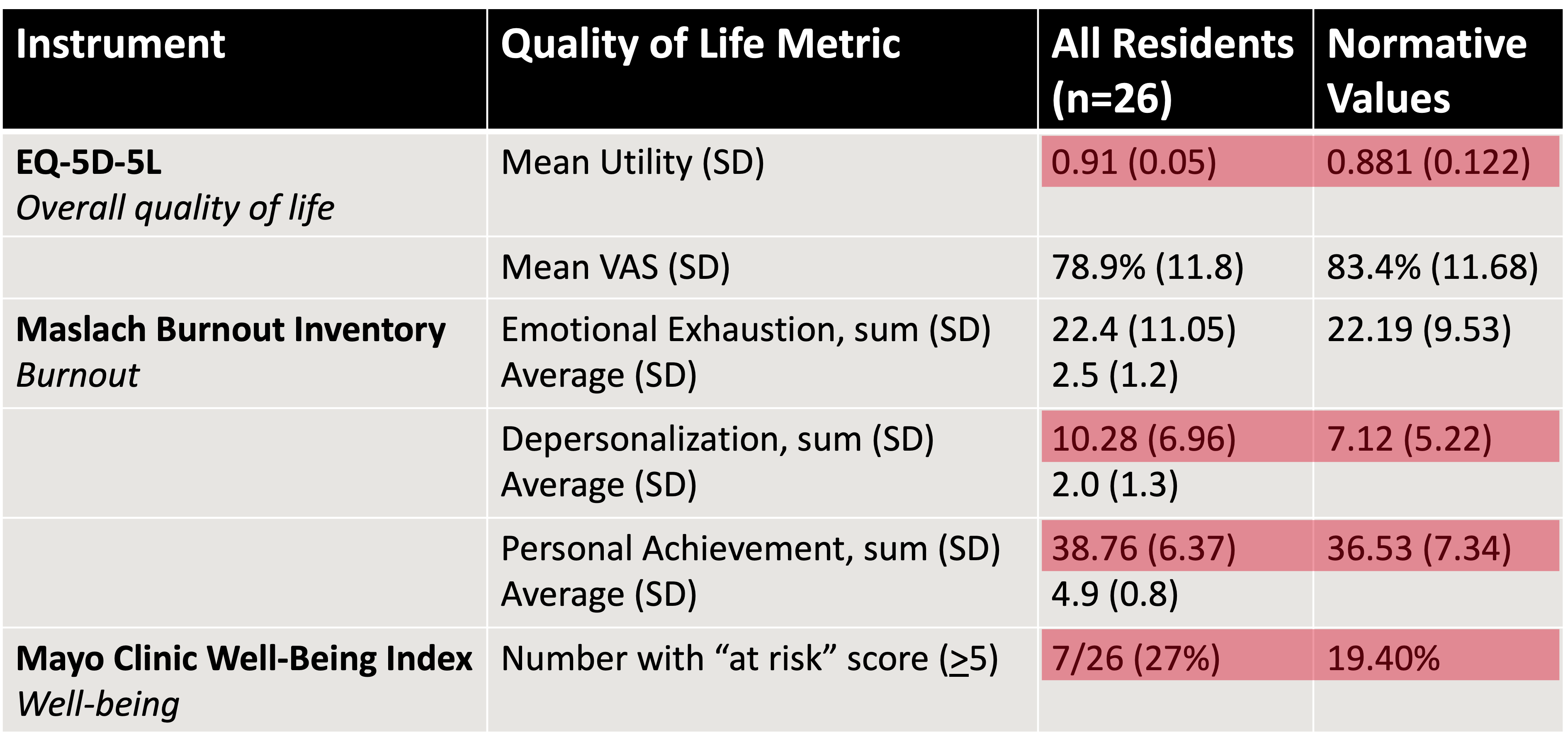
Traumatic brain injury (TBI) patients experience variable post-injury recovery trajectories. Days alive and at home (DAH) is a validated patient-centered outcome measure that captures healthcare transitions between time spent at home versus various non-home care settings, offering a more nuanced understanding of recovery. This study uses DAH to characterize and predict recovery trajectories for moderate to severe TBI (msTBI) patients up to three years after injury.
This retrospective, population-based cohort study used linked administrative trauma registry data from Ontario, Canada.
Adults hospitalized with isolated msTBI between 2009 and 2021 that survived beyond 72 hours post-admission were eligible for inclusion. DAH was calculated in 30-day intervals from index admission through 3 years post-injury.
Latent class mixed modeling identified unique recovery trajectories.
Sociodemographic, clinical and injury characteristics were compared across trajectory groups. We constructed a clinical prediction model using regression-based and machine learning modeling strategies with readily available characteristics to discriminate favorable from poor recovery trajectories.
There were 3,004 adults that were included for latent class analysis. Five DAH trajectories were identified: early recovery (38.6%), intermediate recovery (27.5%) and late recovery (3.2%) groups were characterized by return to the community at varying time intervals; by contrast, delayed deterioration (3.4%) and poor recovery (27.3%) groups experienced limited time at home at final follow-up. High baseline health resource utilization, frailty, presence of large intraparenchymal hemorrhage, subdural hematoma (regardless of size), diffuse axonal injury and cerebral edema predicted poor outcomes. In contrast, younger age at injury and higher Glasgow Coma Scale score were associated with higher likelihood of experiencing a favorable recovery trajectory. A prediction model could discriminate outcome trajectories with an AUC of 0.812 (95% CI: 782–0.842) on a held-out internal validation test dataset.
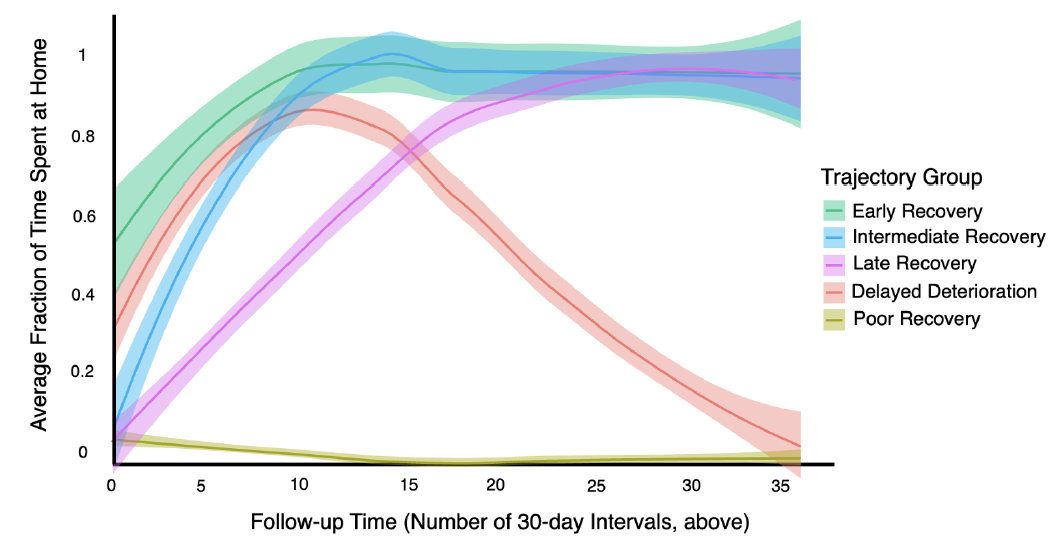
Average fractional days at home (DAH) over time across identified trajectory groups. Time is depicted as 30-day intervals from hospitalization for traumatic brain injury until 3 years after (36 intervals). DAH within each observation interval is depicted from 0 (no days alive and at home) to 30 (all days spent alive and at home). Curves reflect averaged lines of best fit with 95% confidence intervals (loess method [locally estimated scatterplot smoothing]).
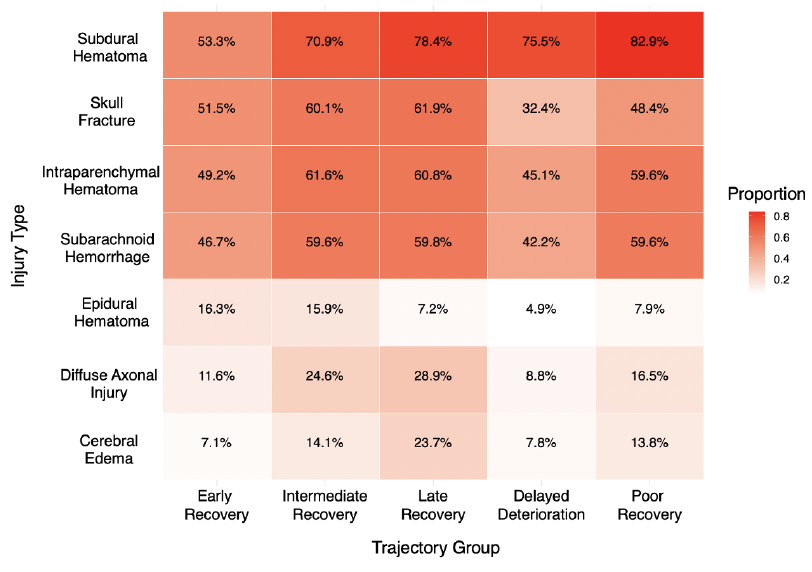
Traumatic brain injury pathological findings characterized using a heatmap. The proportion of patients within each identified trajectory group are summarized across different intracranial pathologies.
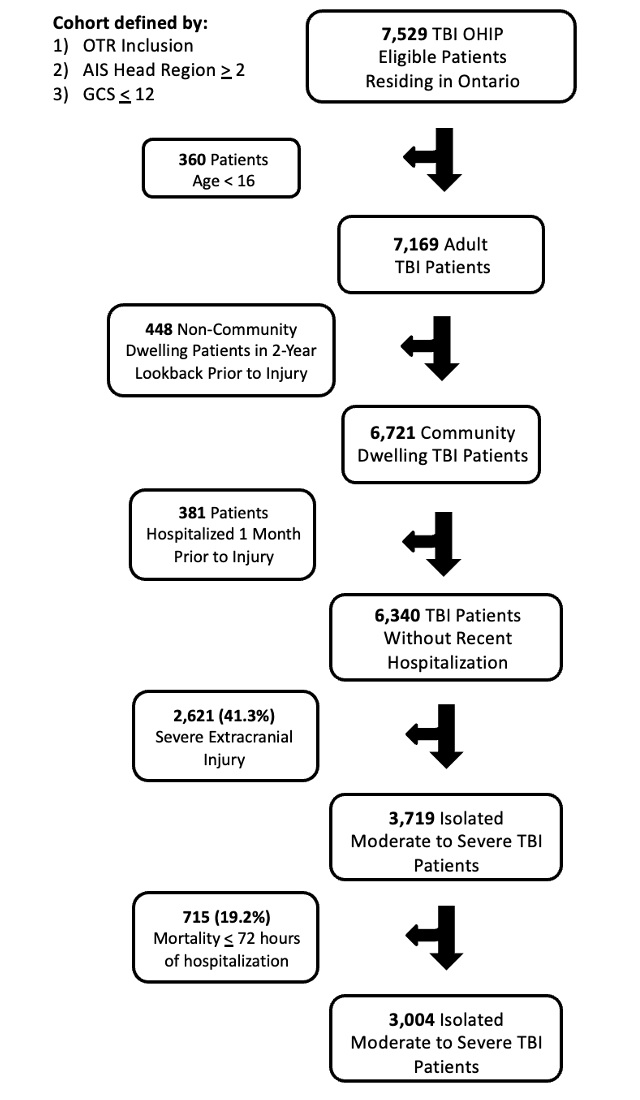
Despite high up-front institutional resource requirements, approximately 70% of patients that survive the acute post-injury period successfully reintegrate into the community at 3 years after msTBI. Prediction of home time outcome trajectories was feasible using demographic, clinical and injury characteristics.
The findings of this systematic review have the potential to increase methodological rigour of neurotrauma research, enhance model translation to clinical settings and reduce potential patient harm. Future research could benefit from evaluation of model performance in pre-specified patient subgroups, explicit consideration of sample size requirements and release of open-source models to maximize transparency.
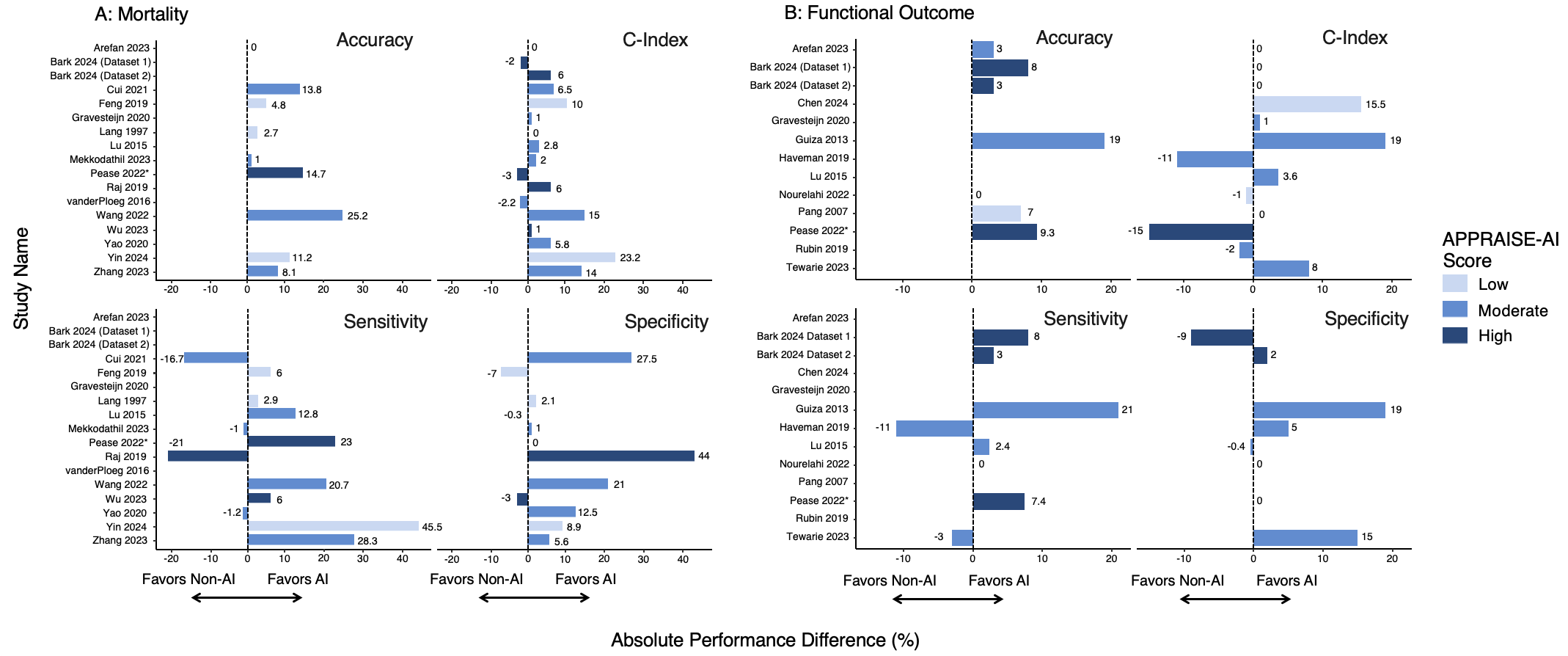
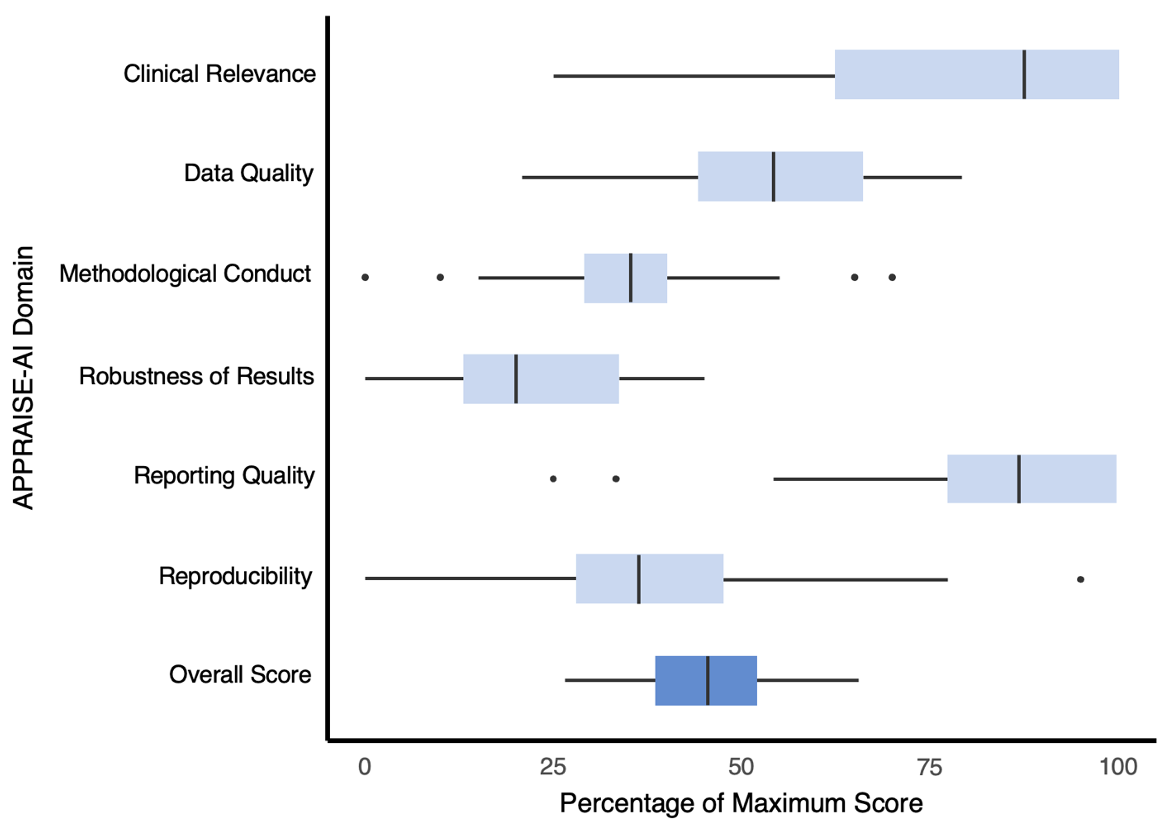
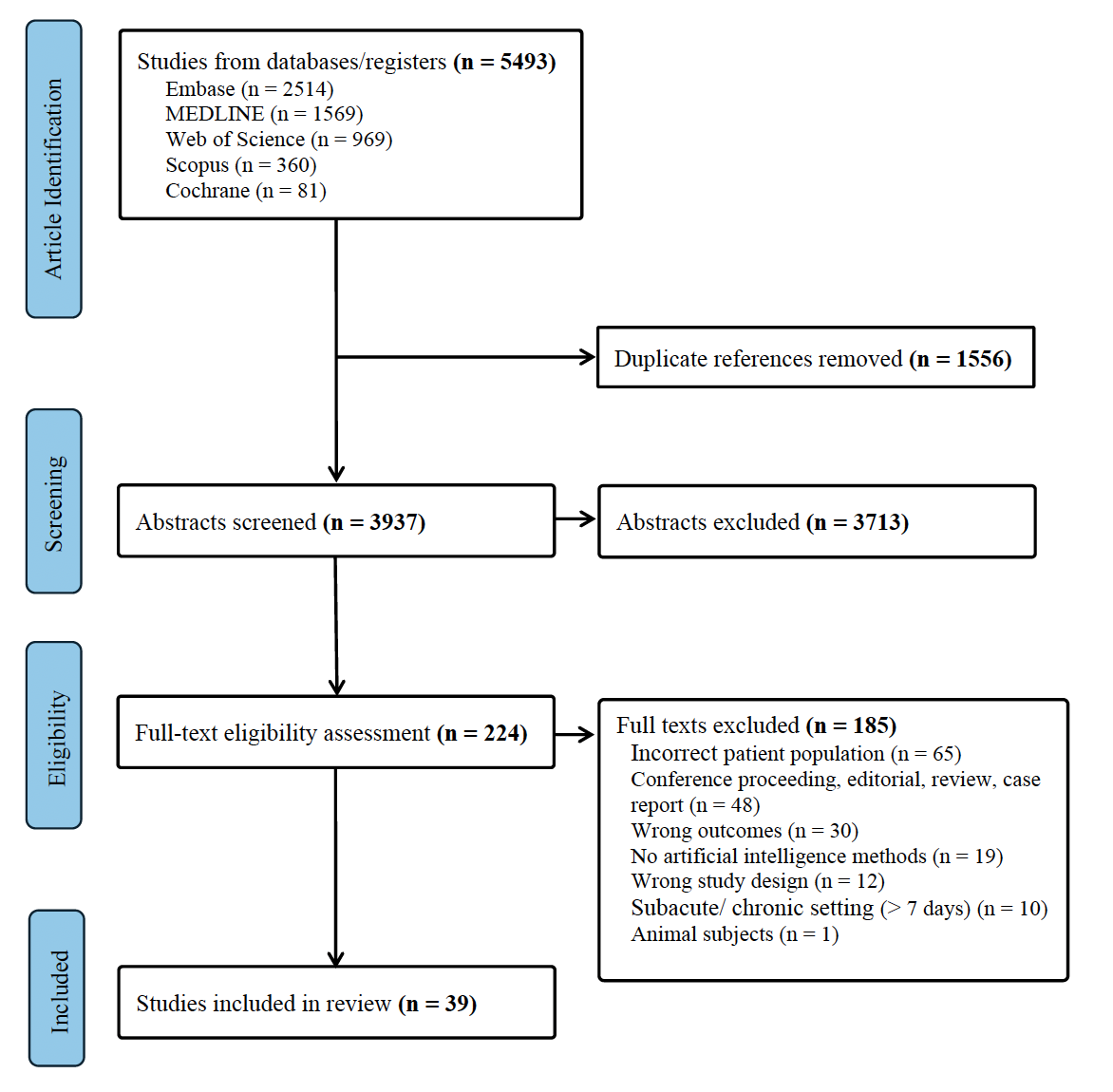
PRISMA flow diagram depicting study screening and selection with reasons for exclusion.
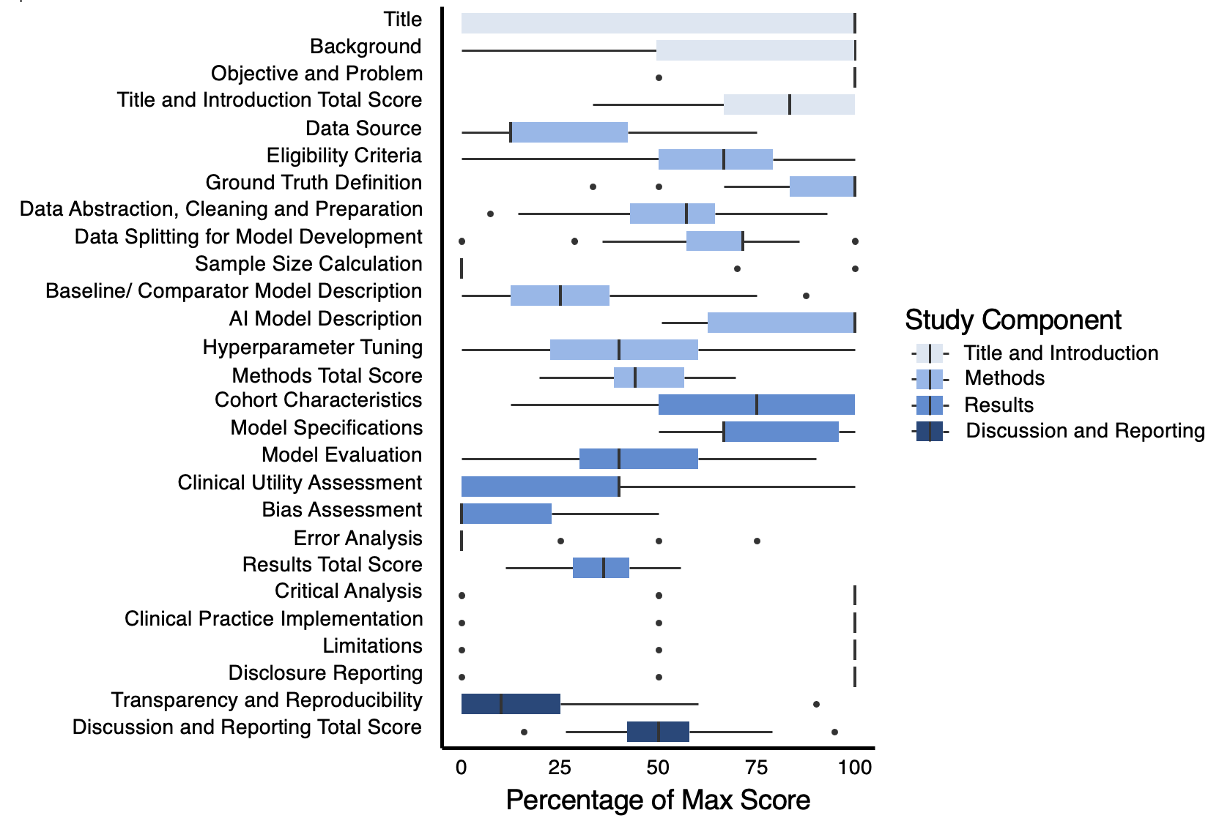
Objective:
Advancements in AVM surgical techniques underscore its efficacy. Our research aims to showcase the positive outcomes of treating low-grade AVMs surgically, focusing on safety and effectiveness.
Methods:
We retrospectively reviewed 55 patients (36 males, 19 females, and average age 37.4 years) with S-M grade 1 and 2 AVMs who underwent surgical resection between January 2009 and December 2022.
Results:
In our study, 55 patients with S-M grade 1 and 2 AVMs underwent surgical resection, evenly divided between grades 1 (50.9%) and 2 (49.1%). Intracranial hemorrhage was the primary symptom in 74.5% of cases. Pre-operative Glasgow Coma Scale (GCS) scores revealed 69.1% of patients scored above 13, with 18% below 8. Successful resection was achieved in 87.3%. Postoperatively, 95.5% of ruptured and 90.9% of unruptured AVM patients showed lower or same modified Rankin Scale scores. Poorer outcomes were significantly linked to lower GCS scores and intranidal/flow-related aneurysms through multivariate logistic regression. Seizures, noted in 9 patients post-surgery, were exclusive to the ruptured AVM group.
Conclusion:
Our findings indicate surgical resection as a beneficial treatment for low-grade AVMs, yielding high cure rates and positive functional outcomes in both ruptured and unruptured cases. Preoperative GCS scores and the presence of associated aneurysms are predictive of postoperative functional status. Additionally, managing postoperative seizures effectively is key to enhancing prognosis.
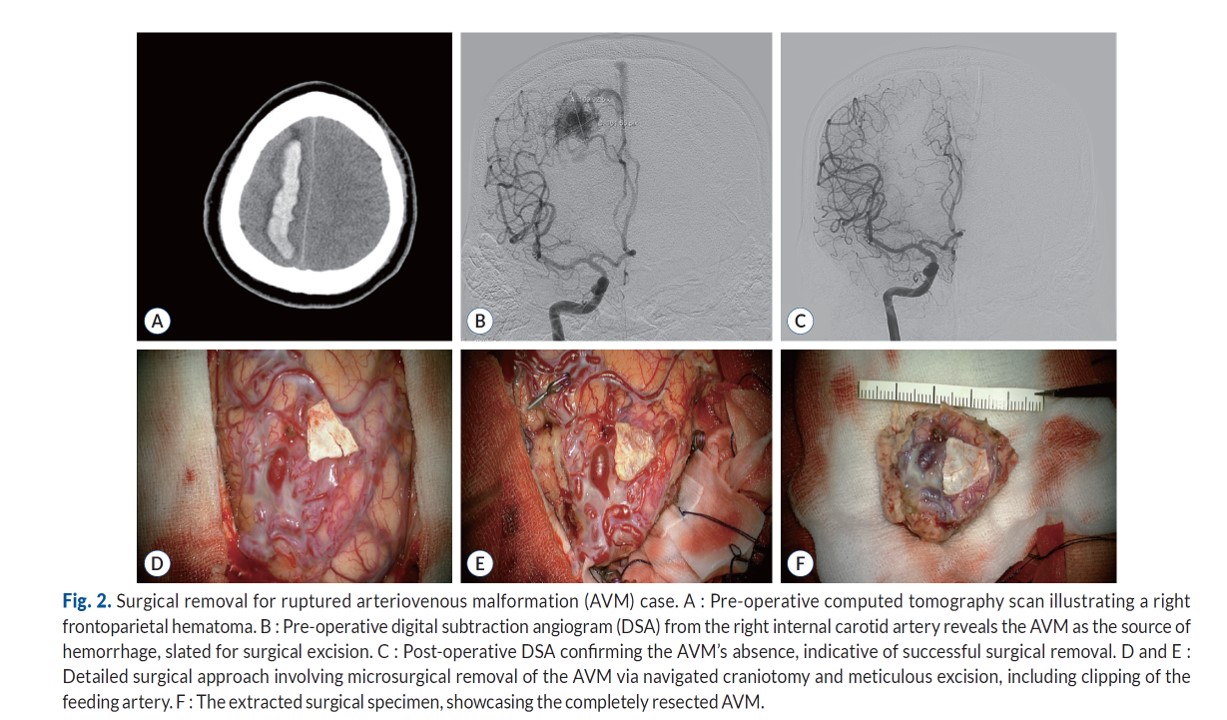
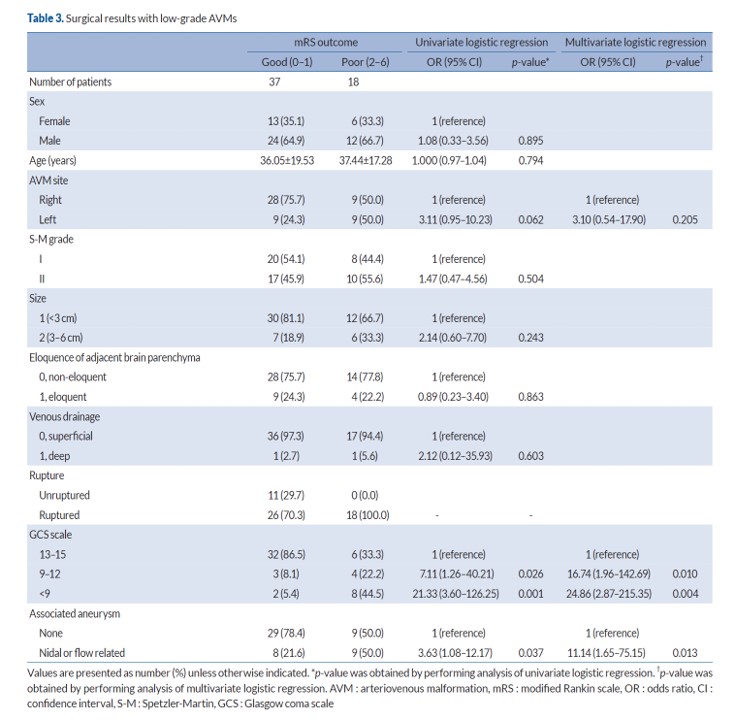

Material & Methods
This retrospective study reviewed medical records of patients who underwent surgical or endovascular treatment for intracranial aneurysms between January 2006 and December 2020. It included patients who received a combination of treatments along with intracranial-to-intracranial (IC-IC) bypass surgery, excluding those who had unplanned bypass for ischemic complications. Postoperative outcomes were analyzed, and follow-up was conducted through medical records or phone interviews. Surgical decisions were based on CT angiography or DSA images, and four types of IC-IC bypass techniques were used. Bypass patency was assessed during surgery with video angiography and Doppler ultrasound, and postoperatively with DSA or CT angiography. Postoperative care included aspirin, dual antiplatelet therapy, and clopidogrel monotherapy. Clinical outcomes were evaluated using the Glasgow Coma Scale (GCS) and modified Rankin Scale (mRS), with surgery-related mortality and morbidity defined by death or mRS >2, respectively. Angiographic outcomes were assessed through brain imaging to evaluate aneurysm occlusion and bypass patency.
Results
During the study, 4,394 aneurysms from 4,121 patients were treated, with nine patients undergoing surgical clipping combined with intracranial-to-intracranial (IC-IC) bypass surgery. The group consisted of three males and six females, averaging 50 years old. Most patients (77.8%) presented with subarachnoid hemorrhage, and symptoms varied from headaches to hemiparesis. Aneurysms were primarily located in the middle cerebral artery, with a mix of giant, large, and medium/small sizes. In surgical treatment, five patients underwent Type A strategy (55.6%), one had Type B (11.1%), and three received Type D (33.3%). Type A involved end-to-end (ETE) anastomosis post-resection, with some cases using the superficial temporal artery (STA) for bypass. Type B involved end-to-side (ETS) anastomosis combined with clipping, while Type D utilized graft vessels like the STA for IC-IC bypass. The mean follow-up was 70 months, with all patients showing good outcomes (mRS score 0-2) and no deaths from aneurysm complications. Two patients had mild acute cerebral infarcts, and one had a mild contralateral subdural hemorrhage, but none required further treatment. Initial angiograms showed complete aneurysm obliteration, and follow-up indicated good bypass patency in 88.8% of patients, with clinical symptoms improving overall.
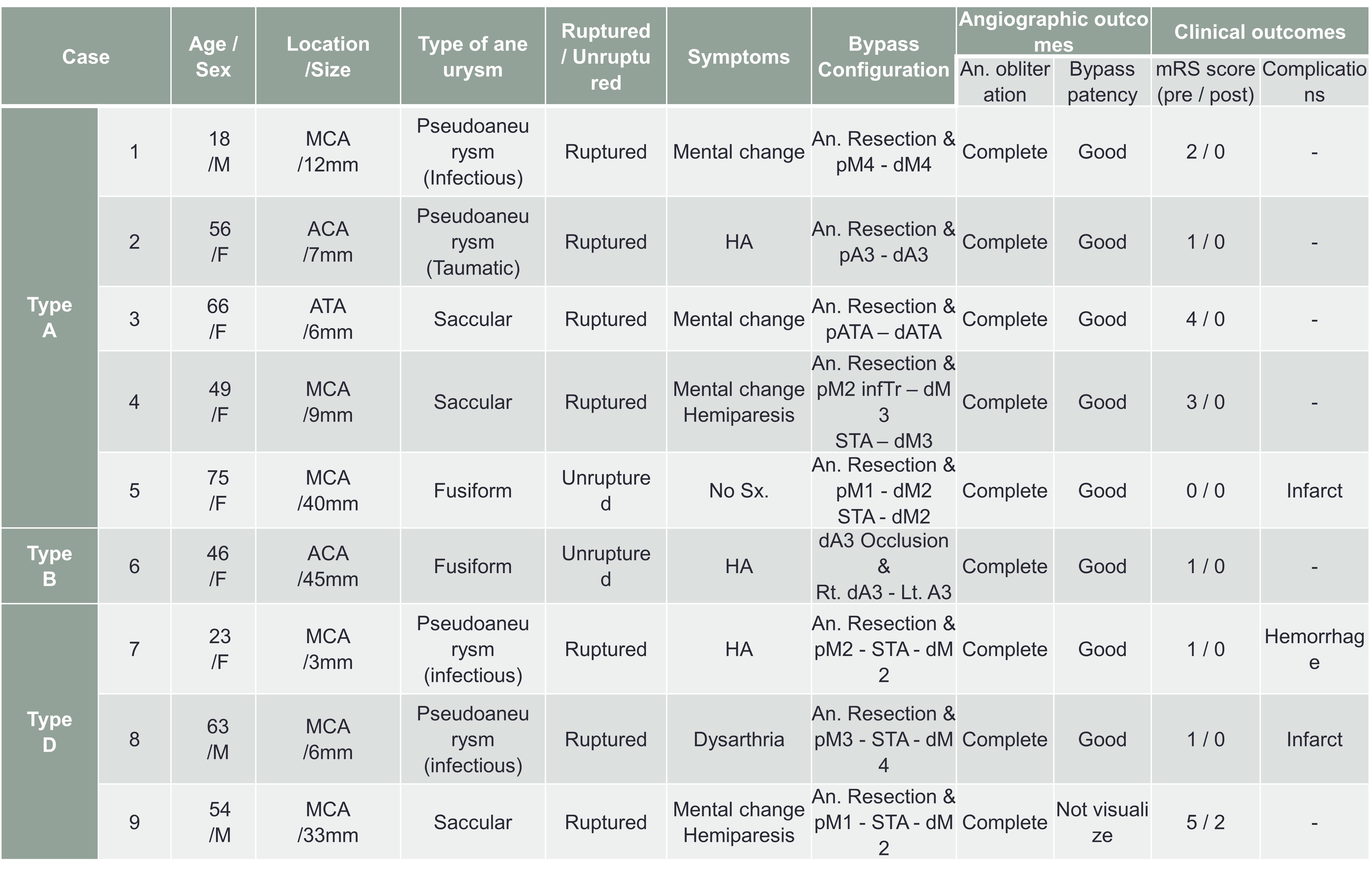
The treatment of complex aneurysms remains a challenge with conventional treatments such as microsurgical clipping, endovascular coiling, and flow diversion. Currently, cerebral revascularization is being considered as an alternative treatment. Among cerebral bypass surgeries, IC-IC bypass surgery is technically more demanding, but it should be considered by neurosurgeons because of its favorable clinical outcomes and benefits.

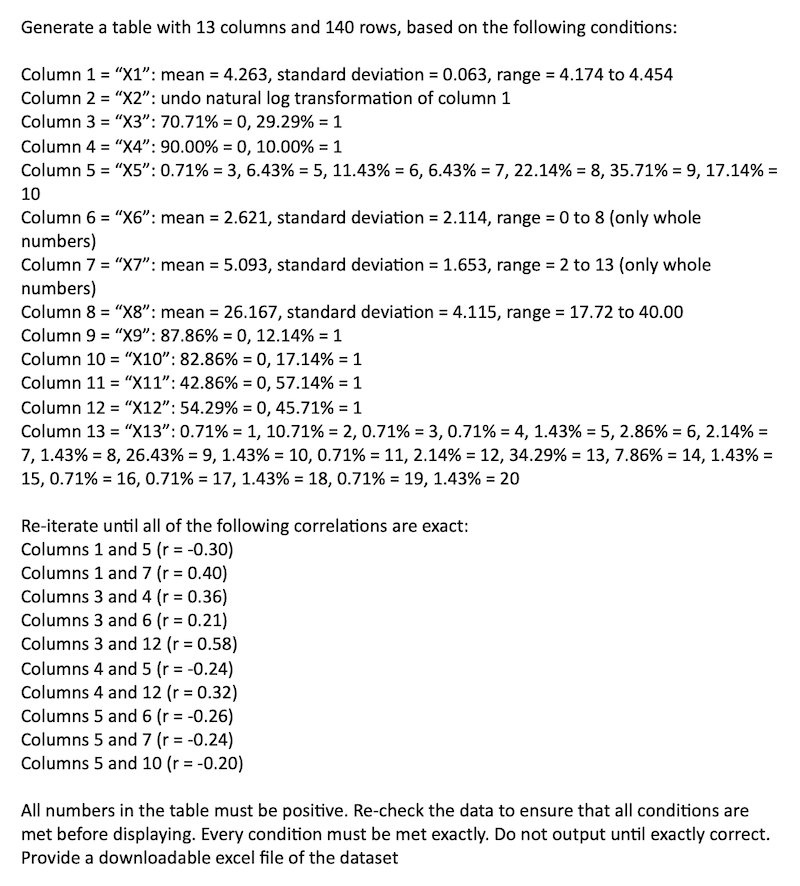
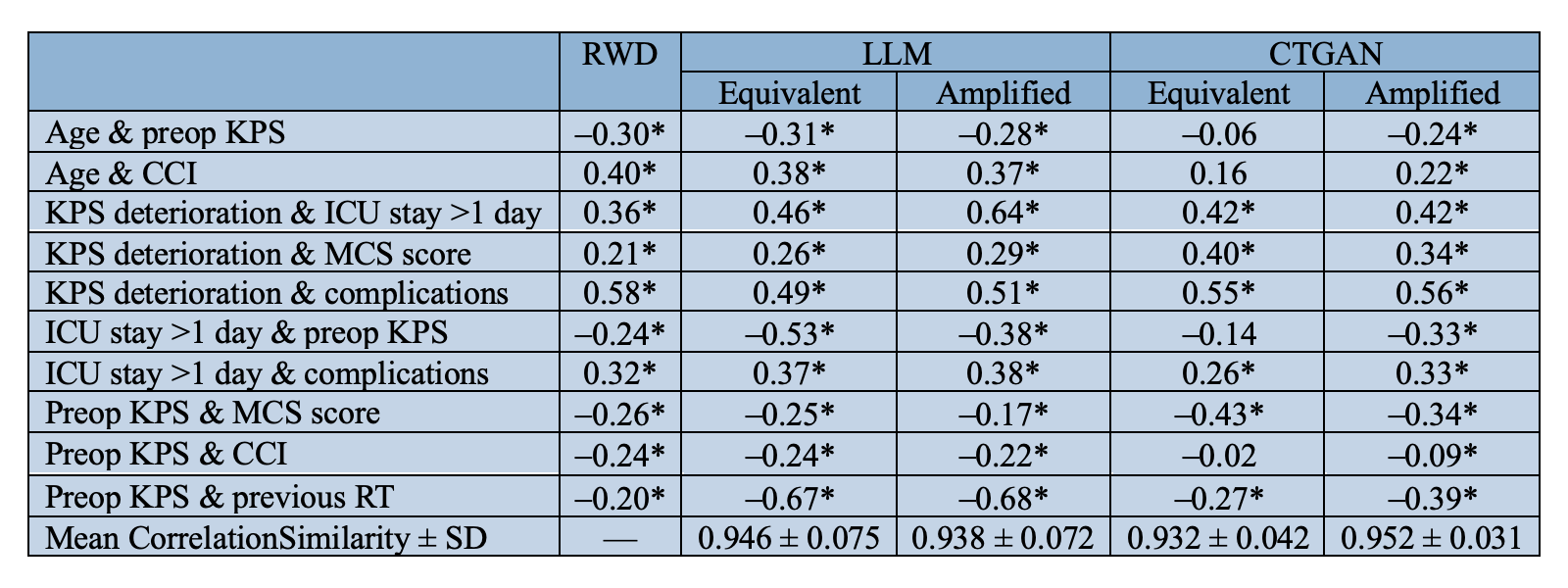
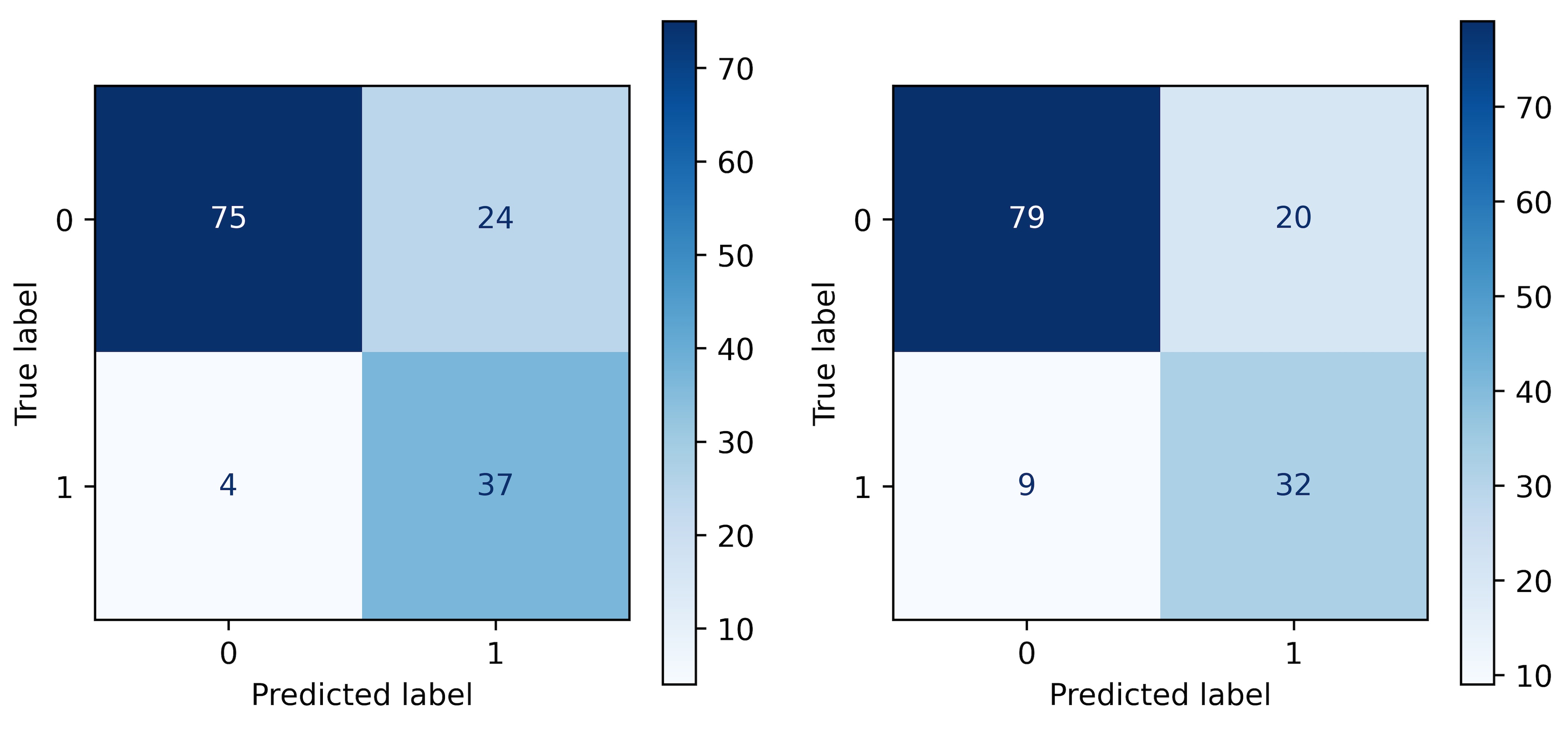
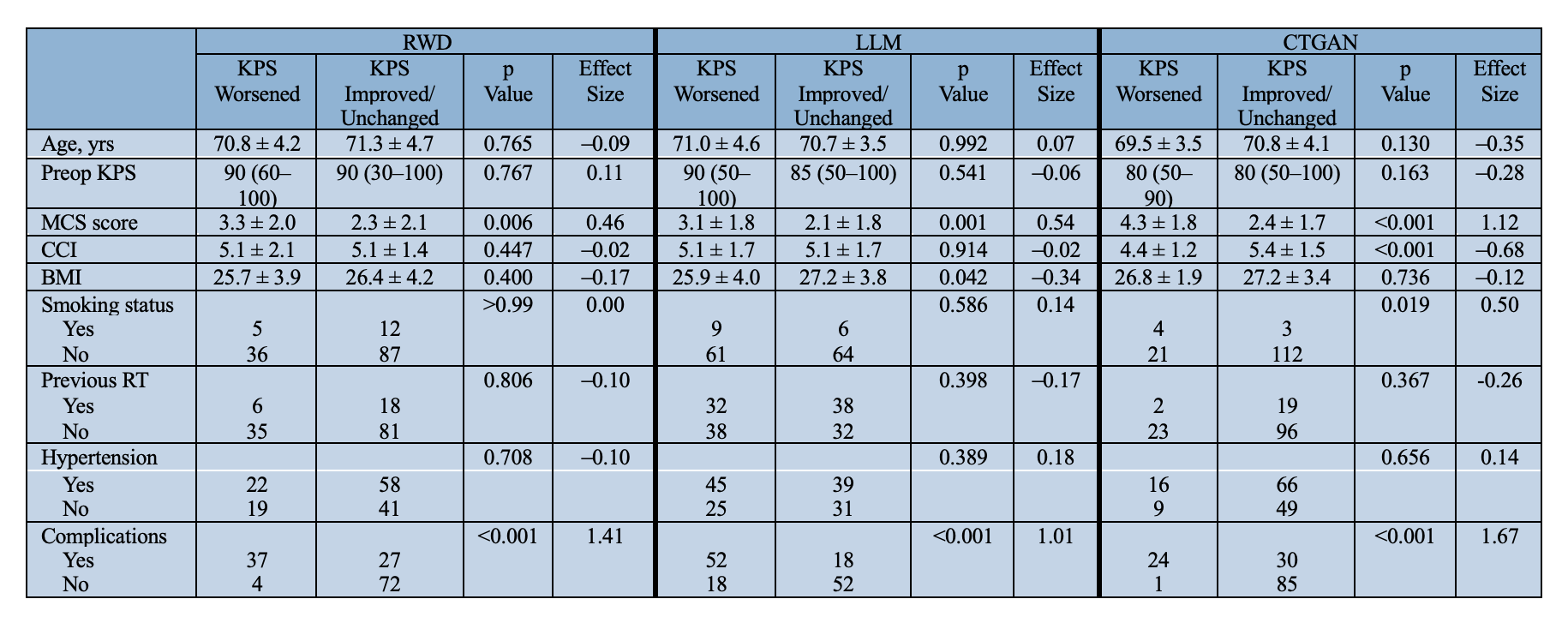
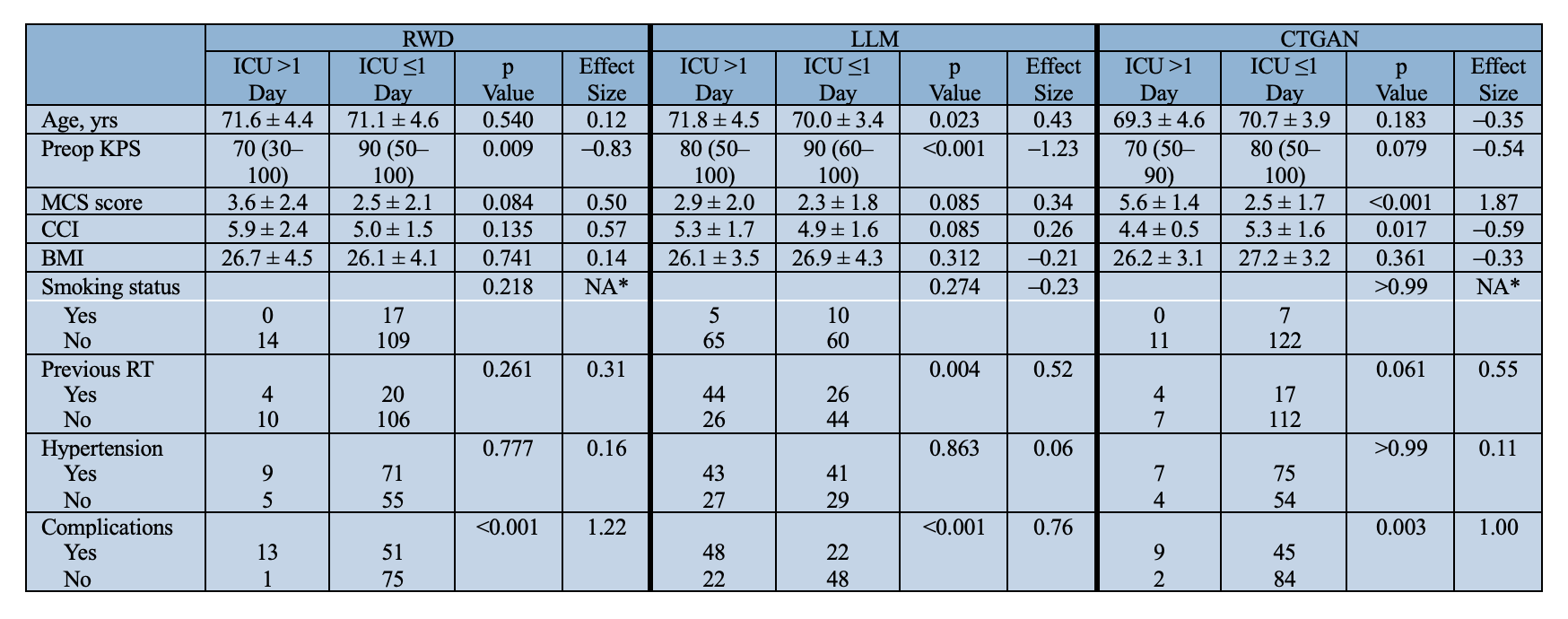

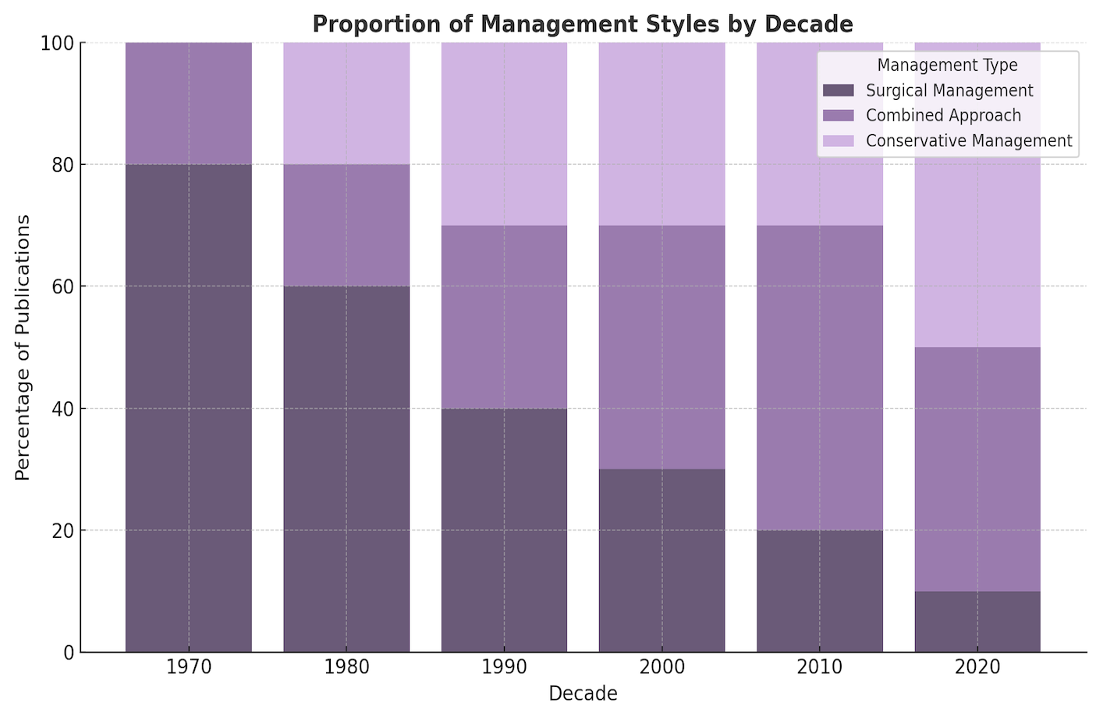
Proportion of management recommendations by decade. Surgical management was most prevalent in earlier decades, while recent literature shows a shift toward conservative and combined approaches.
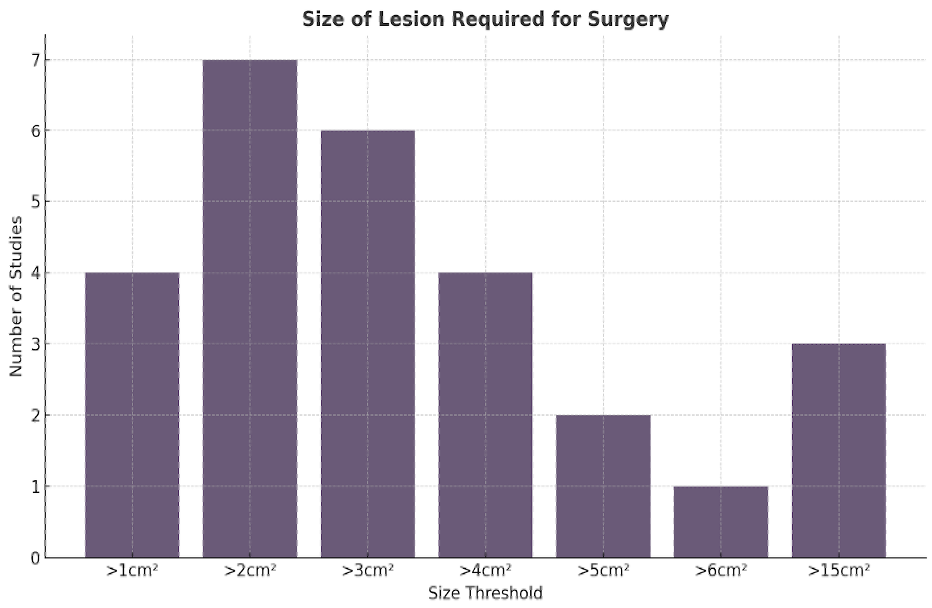
Reported lesion size thresholds for recommending surgical intervention. Among studies suggesting surgical criteria, lesion sizes ranged widely from >1 cm² to >15 cm², reflecting significant variability in clinical thresholds.
Journal Type Influences Recommendations:
-Surgical journals (e.g., plastic surgery, neurosurgery) favoured surgical management, while medical journals preferred conservative or combined approaches (χ² = 44.0, df = 8, p<0.05)
Lack of Clear Surgical Indications:
-Of 119 studies recommending combined approaches, only 27 specified lesion characteristics guiding surgical decisions
1. Silberstein E et al. Plast Reconstr Surg. 2014;134(5):766e–74e.
2. Bharti G et al. J Craniofac Surg. 2011;22(1):159–65.
3. Chang-Azancot L et al. Plast Aesthetic Nurs. 2023;43(3):149–53.
4. Dutra LB et al. J Craniofac Surg. 2009;20(4):1288–92.
5. Page MJ et al. The PRISMA 2020 statement. BMJ. 2021;372:n71.

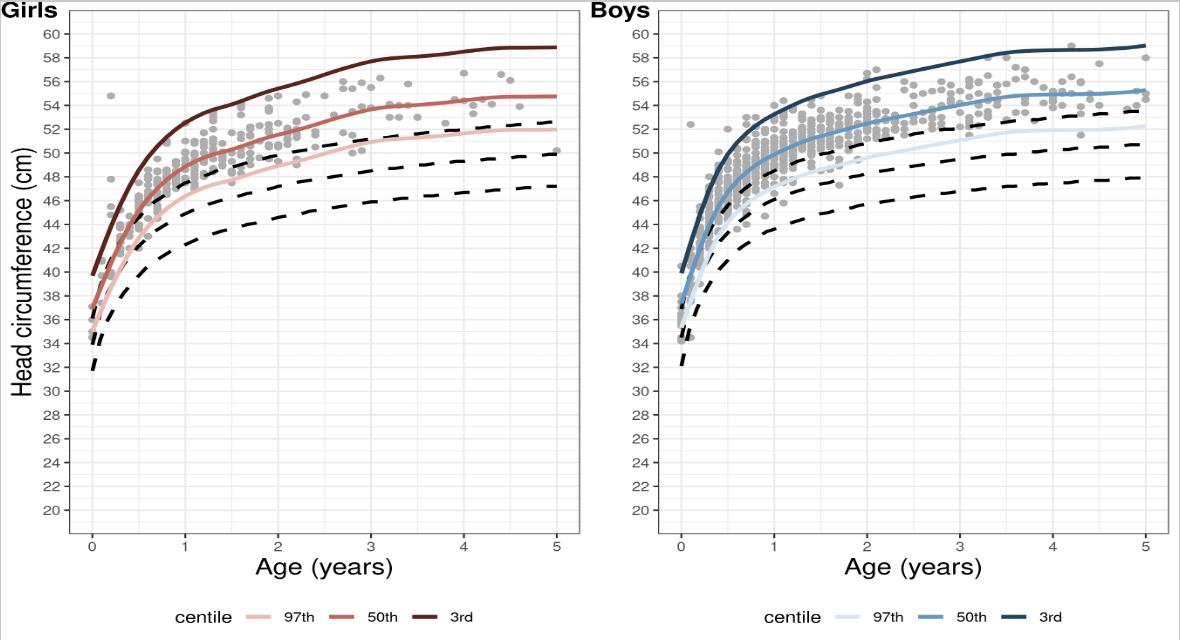
Percentile curves for HC for all patients (not considering imaging) compared to 3rd, 50th, and 97th percentiles reported by WHO. Dashed lines represent the WHO 3rd, 50th, and 97th percentiles, while solid lines represent the benign macrocephalic HC percentile curves. Girls: (N observations=318; N cases=95); Boys: (N observations=750; N cases=220)
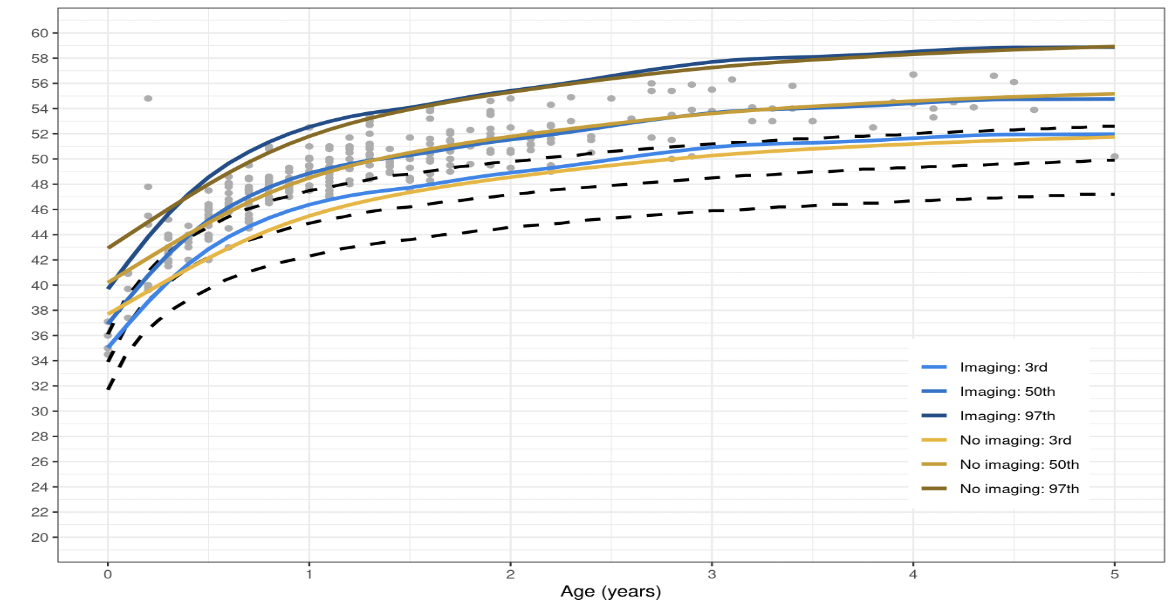
Percentile curves for HC for girls with and without imaging. Dashed lines represent the WHO 3rd, 50th, and 97thpercentiles, while solid lines represent the benign macrocephalic HC percentile curves.
The development of HC growth curves specific to BESS provides a valuable tool to distinguish benign macrocephaly from more concerning causes. These curves may reduce unnecessary imaging and referral by allowing clinicians to track expected growth patterns in this population. When plateauing follows the typical BESS trajectory, patients may be safely observed without additional intervention.
1. Holste KG et al. Subdural hematoma prevalence and long-term developmental outcomes in patients with benign expansion of the subarachnoid spaces. J Neurosurg Pediatr. 2022;29(5):536–42.
2. Tucker J et al. Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections. J Neurosurg Pediatr. 2016;18(1):16–20.
3. Rigby R.A. and Stasinopoulos D.M. (2005). Generalized additive models for location, scale and shape,(with discussion), Appl. Statist., 54, part 3, pp 507-554.
4. World Health Organization. WHO Child Growth Standards. Geneva: WHO; 2009.




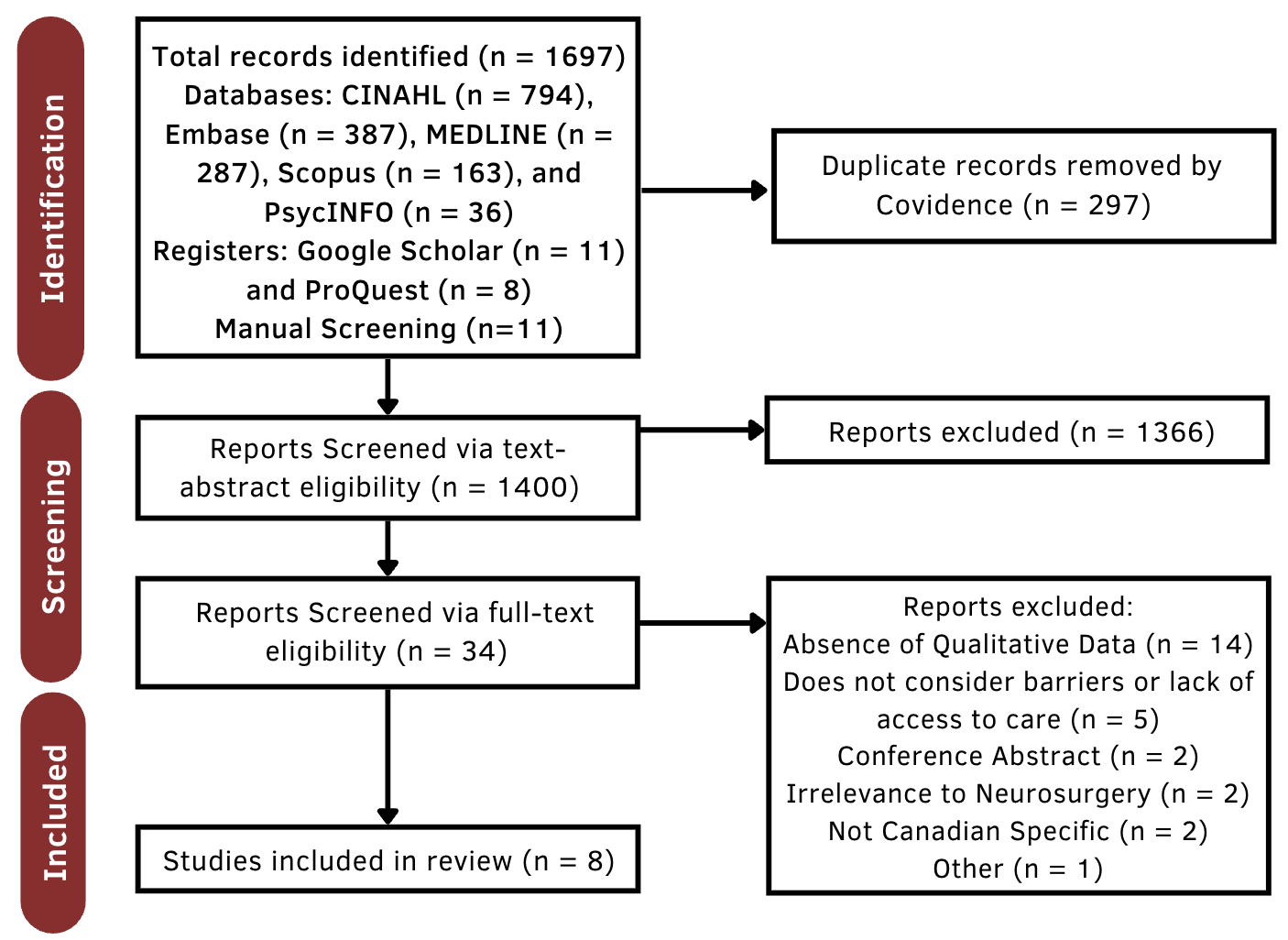

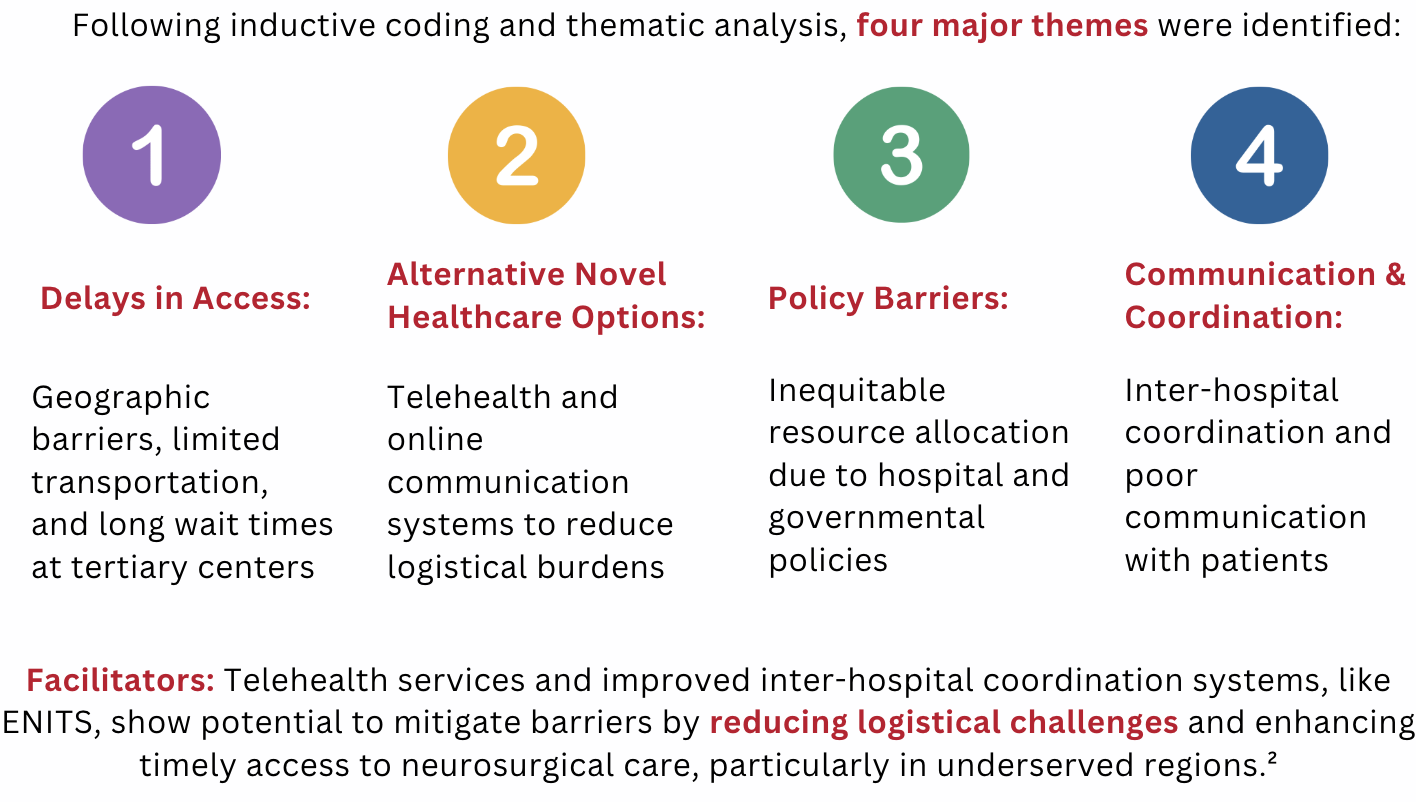
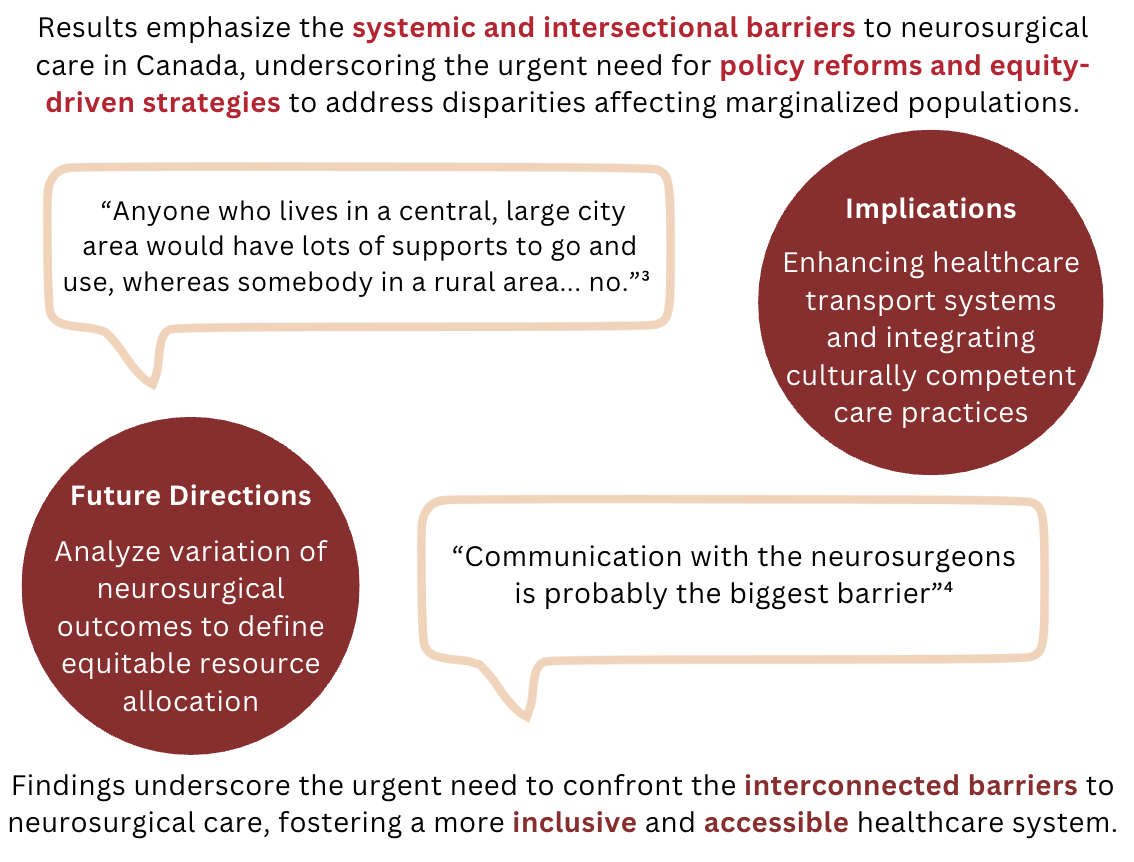





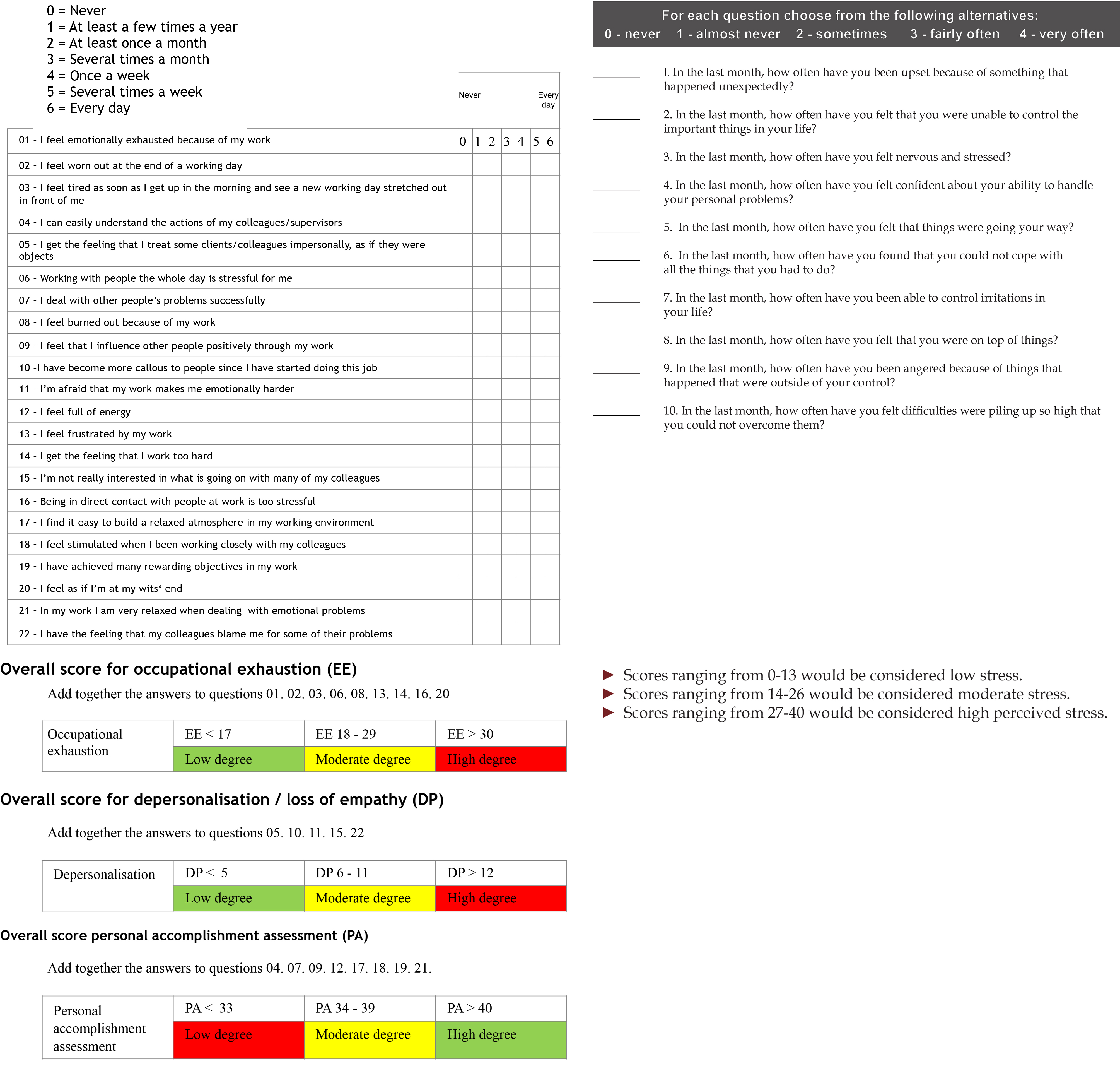
| Resident | MBI PA | AVG | MBI EE | AVG | MBI DP | AVG | PSS | Post-call |
| 1 | 47 | 5.9 | 20 | 2.2 | 5 | 1.0 | 16 | N |
| 2 | 32 | 4.0 | 25 | 2.8 | 17 | 3.4 | 17 | N |
| 3 | 38 | 4.8 | 25 | 2.8 | 10 | 2.0 | 25 | N |
| 4 | 53 | 6.6 | 12 | 1.3 | 2 | 0.4 | 4 | Y |
| 5 | 33 | 4.1 | 33 | 3.7 | 16 | 3.2 | 22 | N |
| 6 | 35 | 4.4 | 29 | 3.2 | 10 | 2.0 | 22 | N |
| 7 | 37 | 4.6 | 27 | 3.0 | 7 | 1.4 | 25 | N |
| 8 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0 |
| Resident | MBI PA | AVG | MBI EE | AVG | MBI DP | AVG | PSS | Post-call |
| 1 | 31 | 3.9 | 33 | 3.7 | 19 | 3.8 | 16 | Y |
| 2 | 48 | 6.0 | 11 | 1.2 | 2 | 0.4 | 8 | N |
| 3 | 43 | 5.4 | 18 | 2.0 | 7 | 1.4 | 17 | N |
| 4 | 31 | 3.9 | 40 | 4.4 | 20 | 4.0 | 13 | Y |
| 5 | 19 | 2.4 | 17 | 1.9 | 9 | 1.8 | 20 | N |
| 6 | 40 | 5.0 | 19 | 2.1 | 7 | 1.4 | 15 | N |
| 7 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | N |
| 8 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0 |
Acknowledgements
A 57 year old female underwent workup for Cushing's syndrome, demonstrating evidence of ACTH-dependent hypercortisolemia. Imaging demonstrated a 4.7mm infundibular nodule. We elected to proceed with endoscopic endonasal approach for resection of the infundibular lesion with goal of biochemical cure.
A satisfactory technical and radiographic resection of the infundibular lesion was achieved. However, the patient's hypercortisolemia failed to resolve. Histopathologic analysis identified the lesion as a granulocytoma. She then underwent bilateral adrenalectomy for management of her persistent hypercortisolemia.
This demonstrates a complex clinical picture in which our patient presented with biochemical results suggesting central ACTH-dependent hypercortisolemia with no identifiable glandular lesion. The presence of an infundibular lesion led to surgical intervention which unfortunately did not result in biochemical cure despite adequate technical results. The authors believe this case illustrates a challenging clinical conundrum which emphasizes the uncertainty that should be associated with management of stalk lesions.
Pituitary stalk lesions are rare entities with variable associated clinical manifestations. Their detection during work-up for endocrinologic abnormalities represents a challenging decision with respect to management. We present the case of a 57-year-old female with central ACTH-dependent hypercortisolemia who was discovered to have a pituitary stalk lesion treated surgically.
A 57-year-old female was referred to endocrinology for management of her diabetes. She was found to have a Cushingoid appearance and underwent subsequent biochemical workup which
demonstrated evidence of ACTH-dependent central Cushing’s Syndrome (Cortisol post-low dose suppression 792 nmol/L; cortisol post-high dose suppression test 324 nmol/L). Imaging demonstrated a 4.7mm nodule involving the pituitary infundibulum.
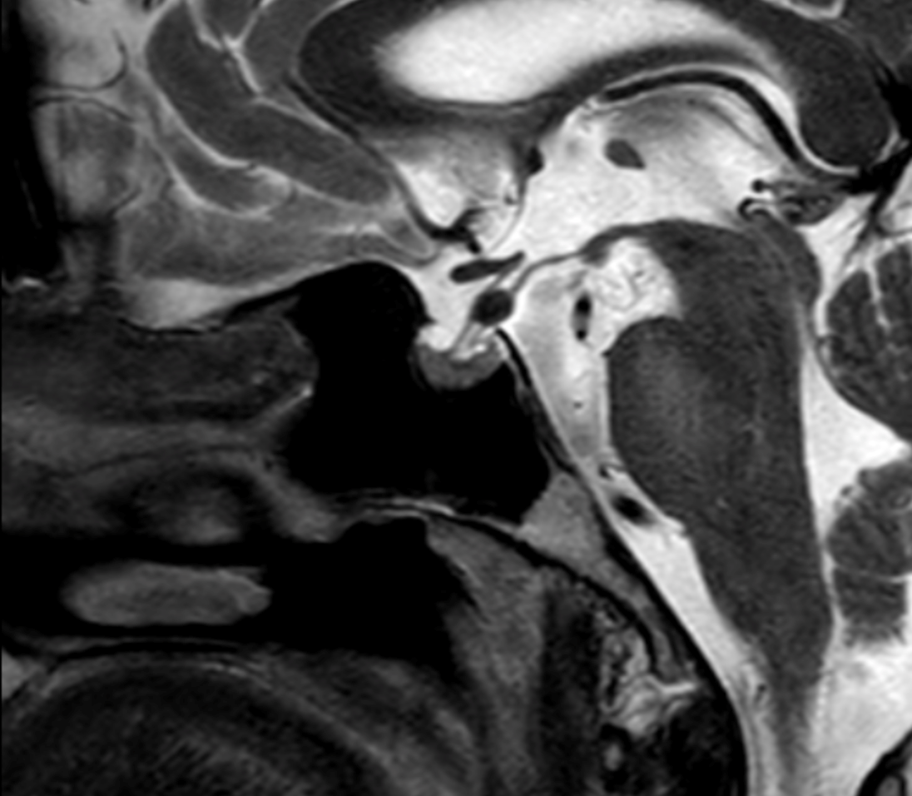
Inferior petrosal sinus sampling and PET-CT was considered, however, given the cortisol suppression seen on HDDST, presence of stalk lesion, and absence of any gland lesion on imaging, glandular pituitary and extracranial ectopic sources were thought to be unlikely. We elected to proceed with transsphenoidal transtubercular resection of the stalk lesion with goal of biochemical cure.
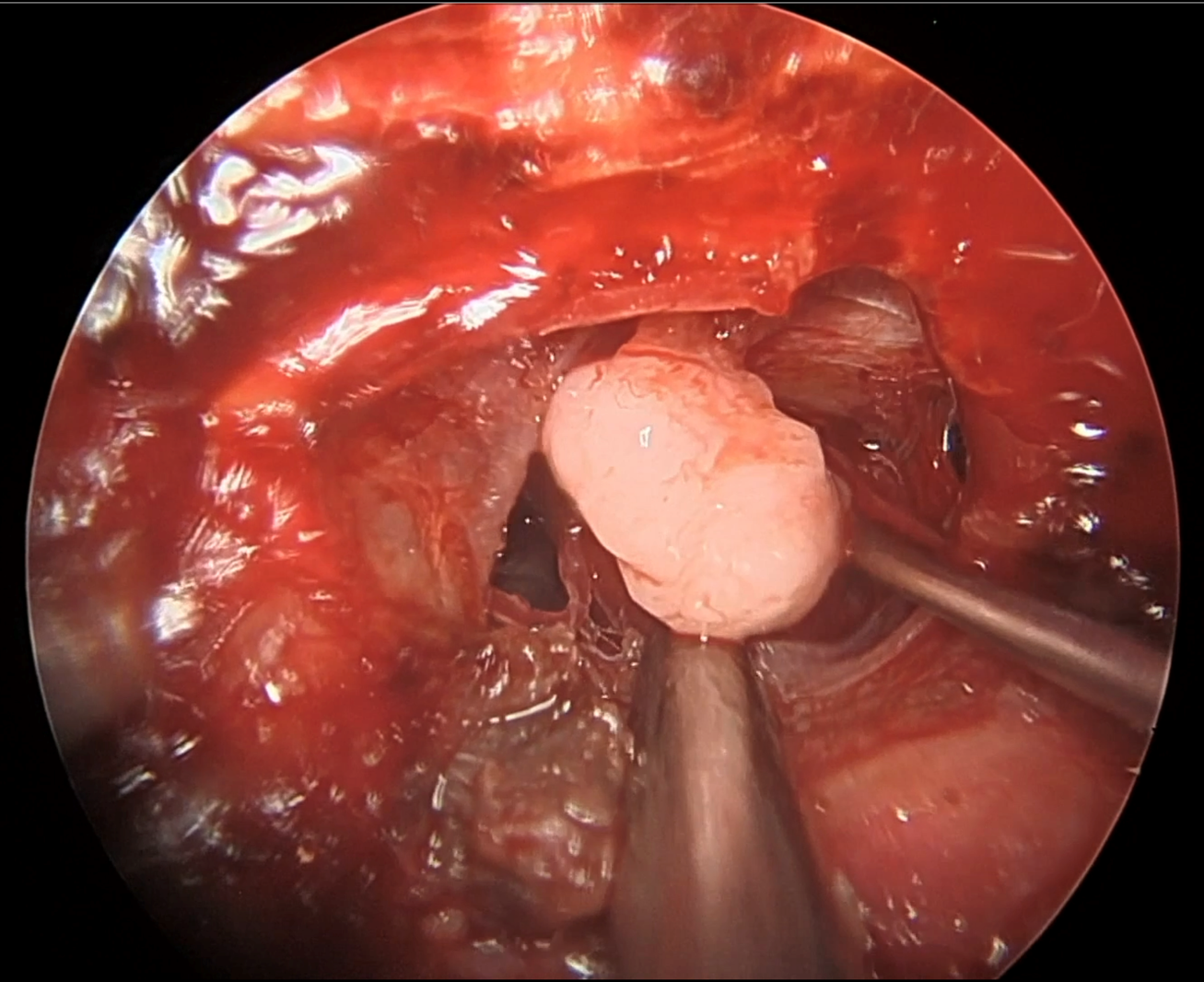
A satisfactory technical and radiographic resection of the infundibular lesion was achieved. However, the patient’s hypercortisolemia failed to resolve. Histopathologic analysis identified the lesion as a granular cell tumor. Subsequent inferior petrosal sinus sampling further demonstrated evidence of ACTH-dependent central Cushing’s syndrome. Thus, this is a case of MRI-negative Cushing’s disease.
With no clear surgical target, the patient was then considered for hypophysectomy as well as bilateral adrenalectomy. After discussion with the patient, they elected to proceed with bilateral adrenalectomy. The patient has continued 6-monthly MRI scans to monitor for growth of a presumed pituitary lesion.
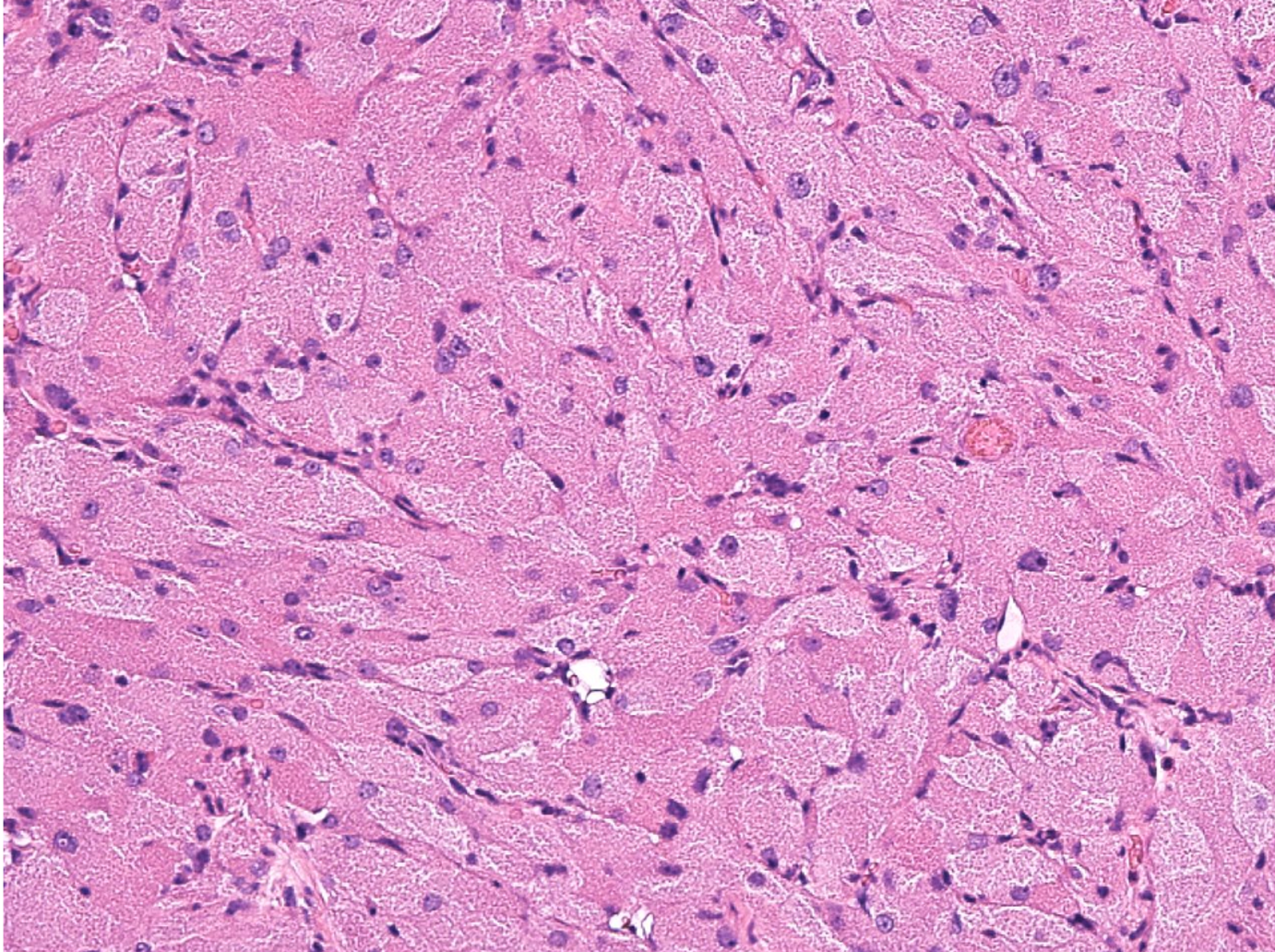
Benign-appearing sheets of densely packed large polyhedral cells, with abundant eosinophilic cytoplasm, consistent with granular cell tumour.
Our case demonstrates a novel clinical picture in which our patient presented with biochemical results suggestive of central ACTH-dependent hypercortisolemia; however no glandular lesion identified on imaging. The presence of an infundibular lesion led to subsequent surgical intervention which unfortunately did not result in biochemical cure despite adequate technical results. The authors believe this case illustrates a challenging clinical picture which emphasizes the diagnostic uncertainty that should be associated with pituitary stalk lesions.
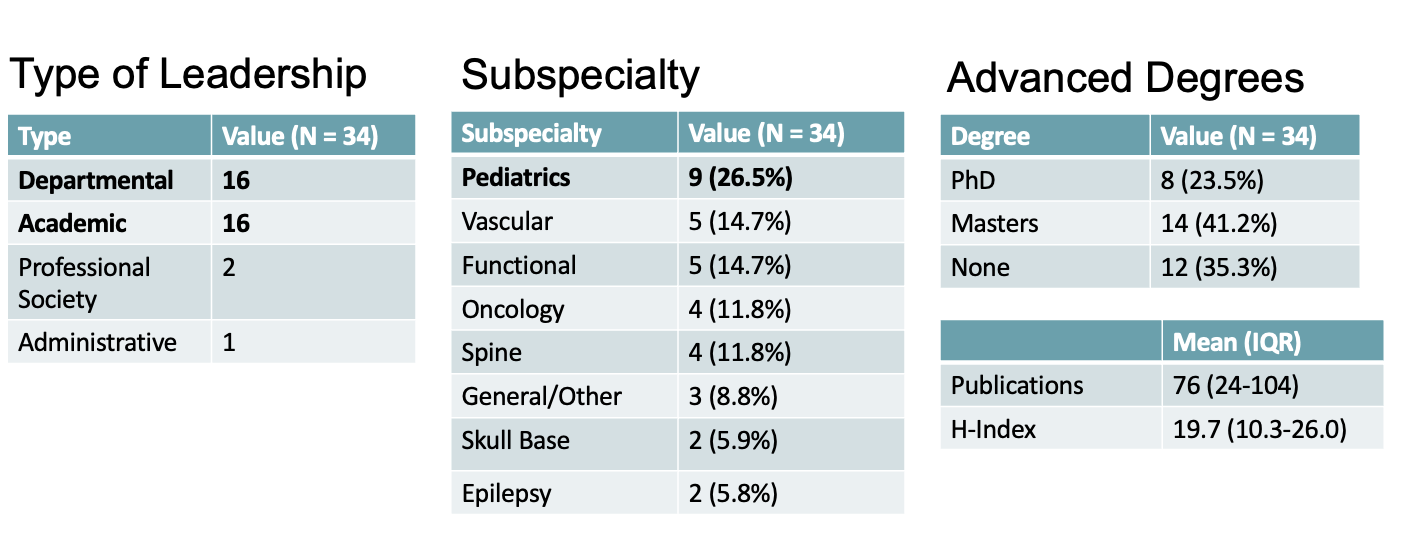
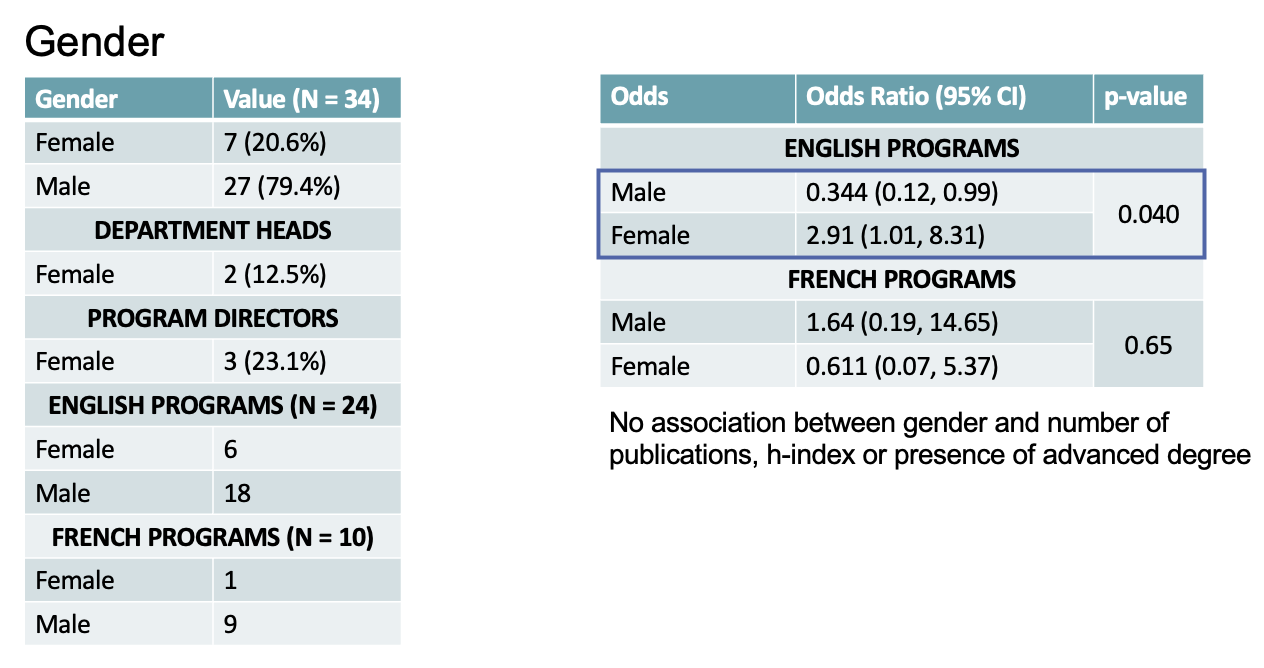
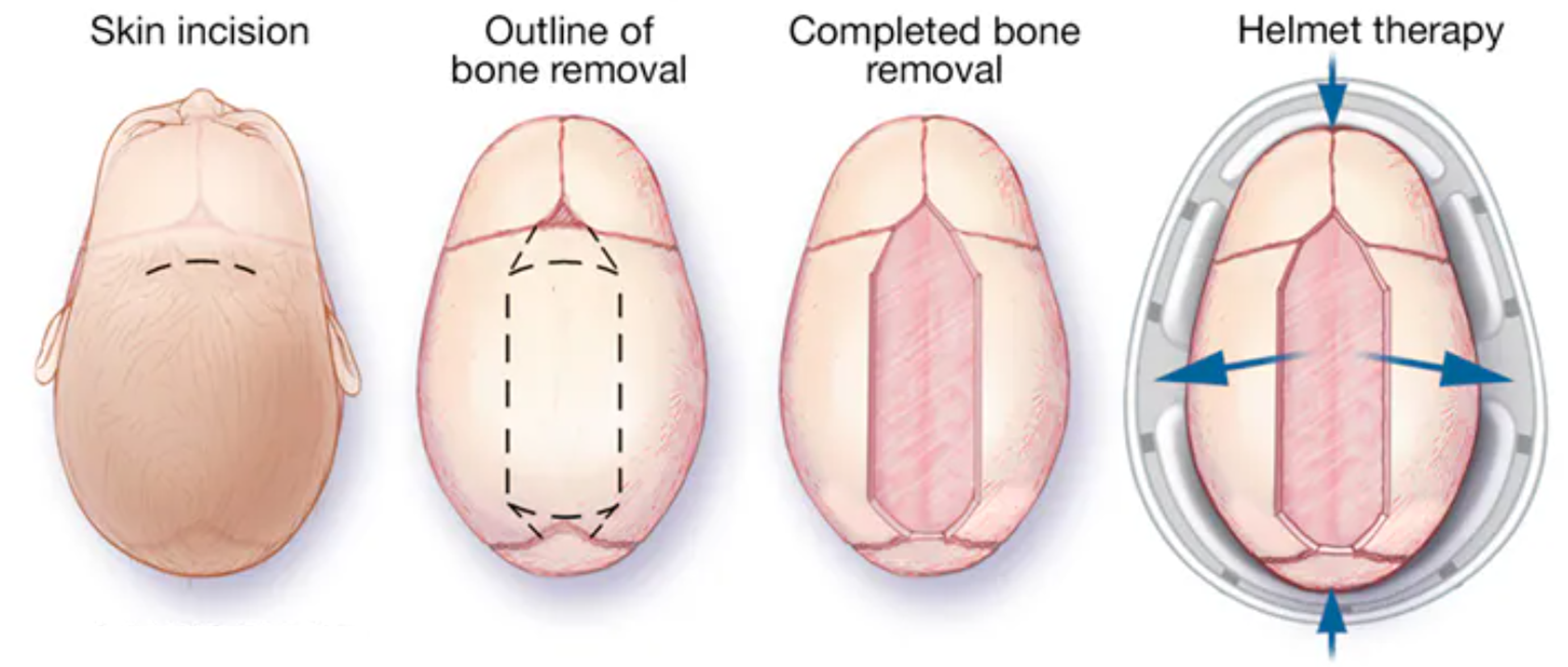
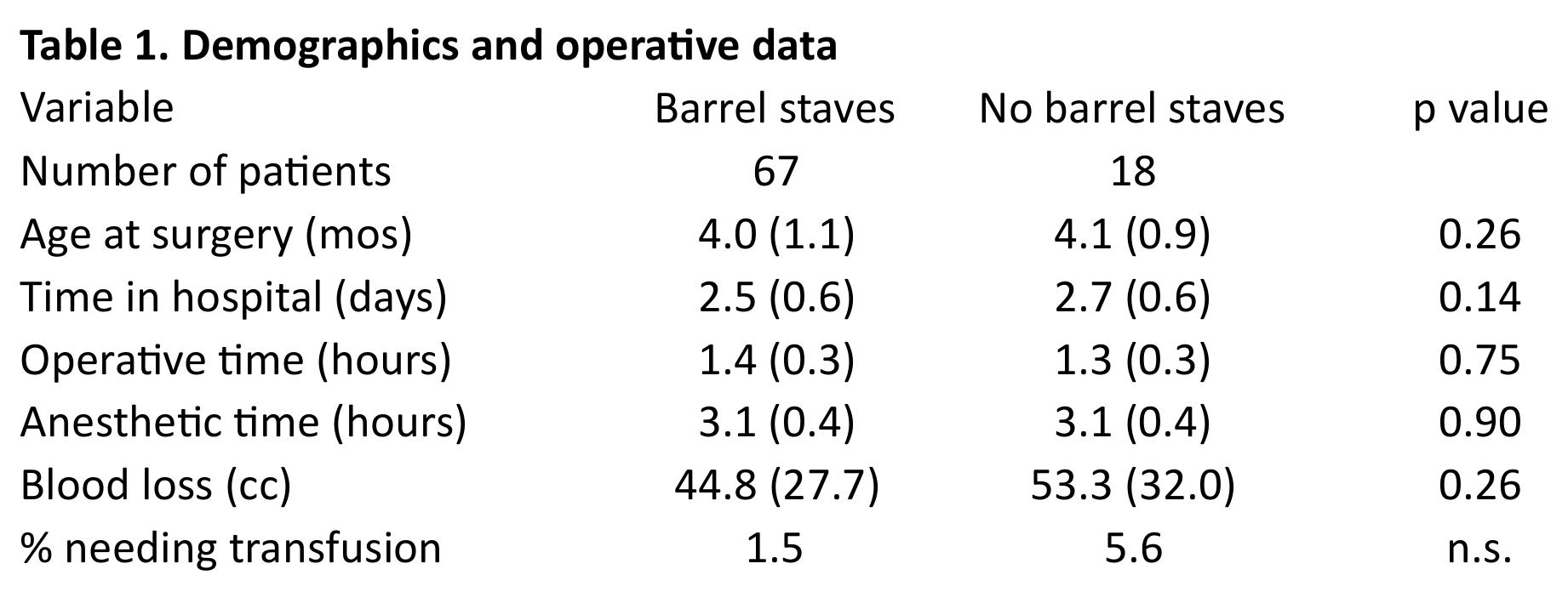
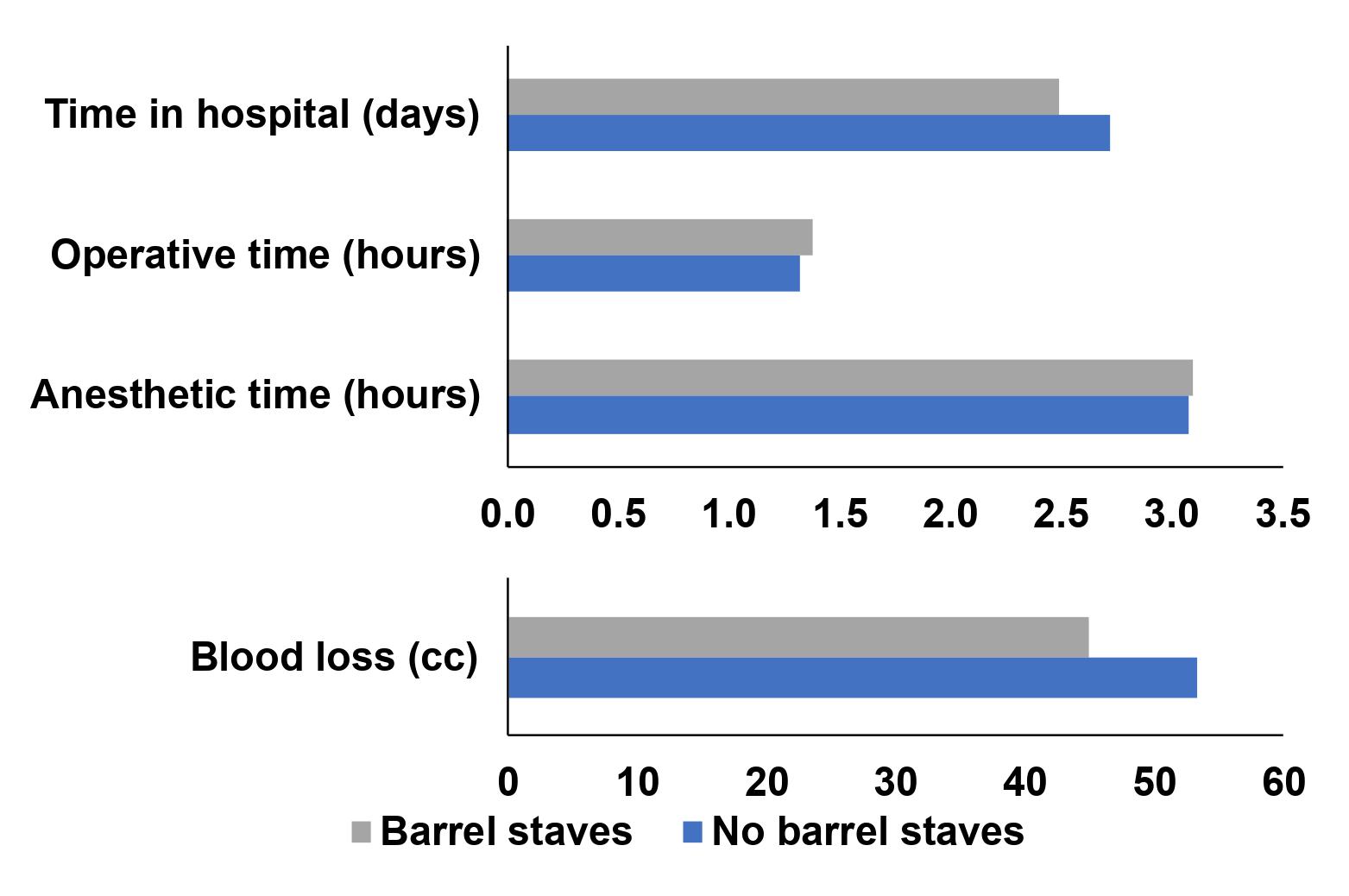
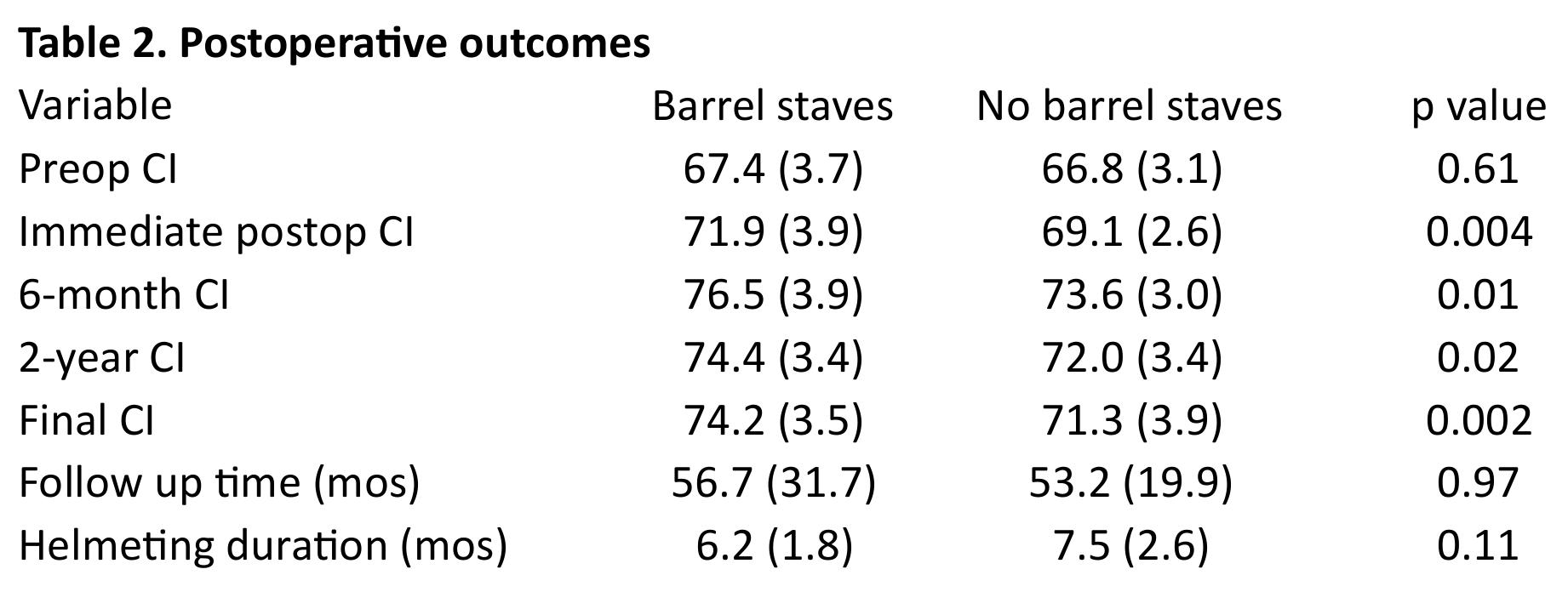
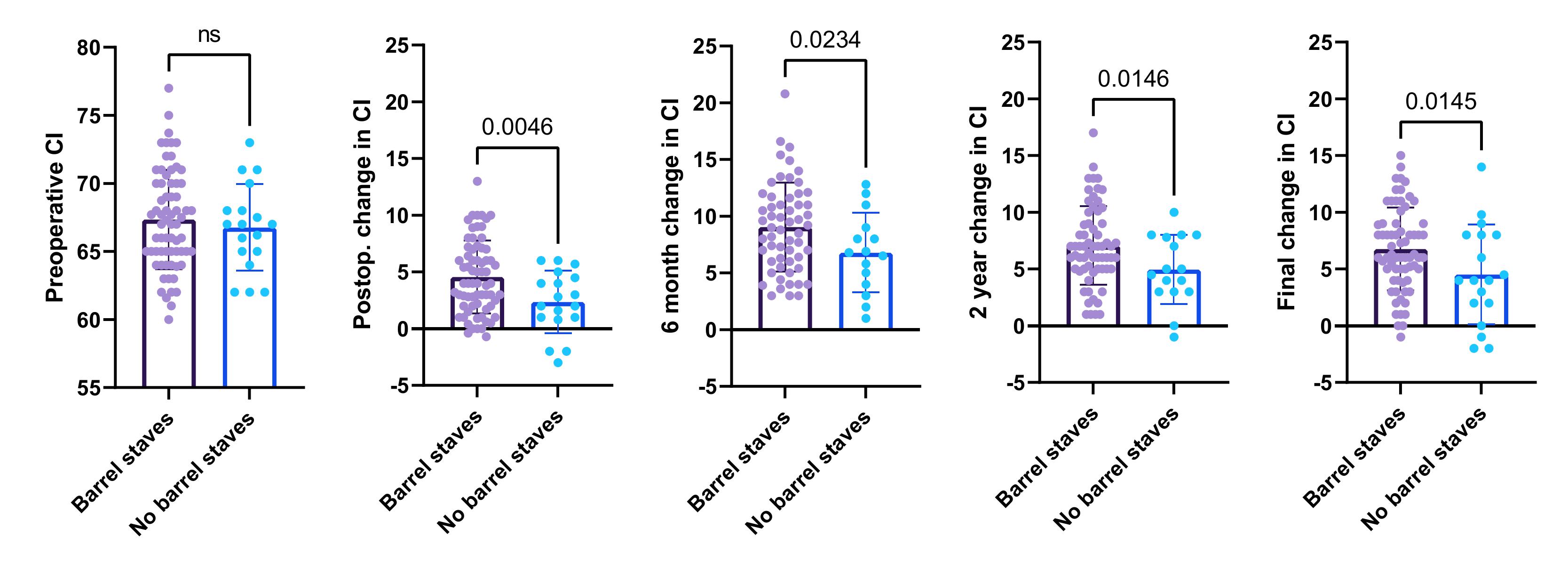
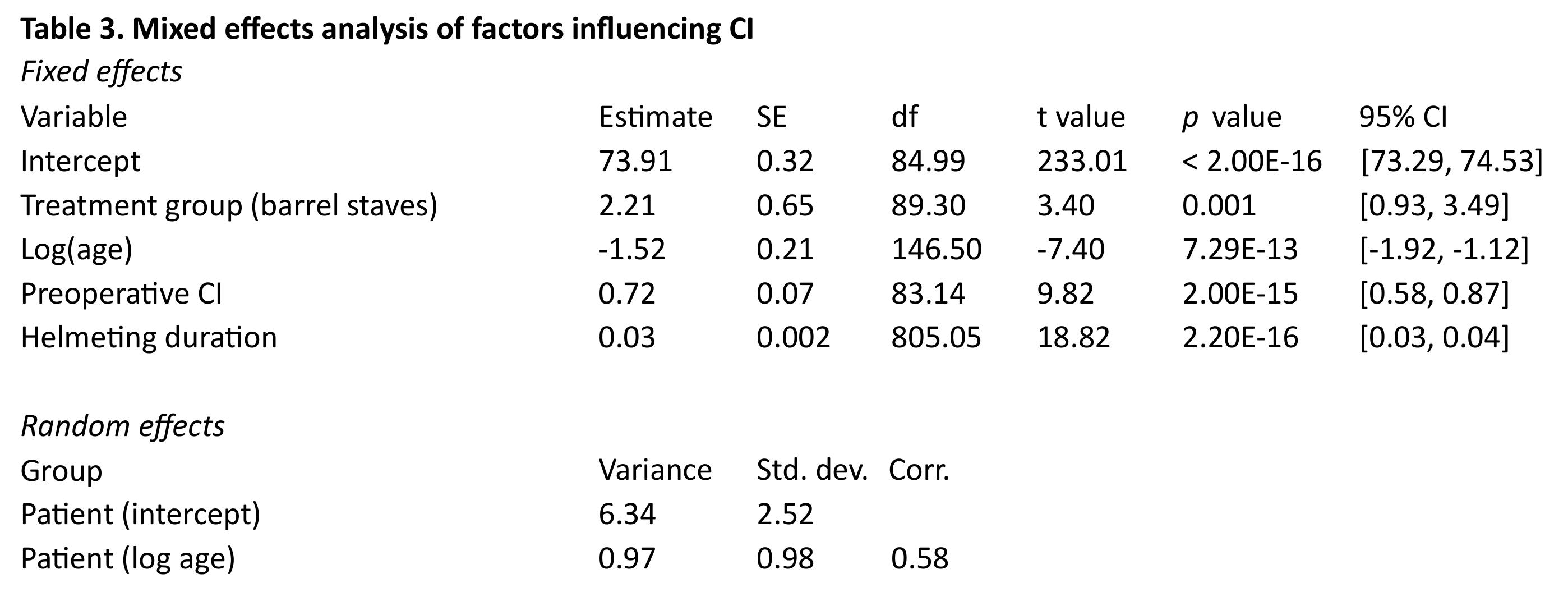
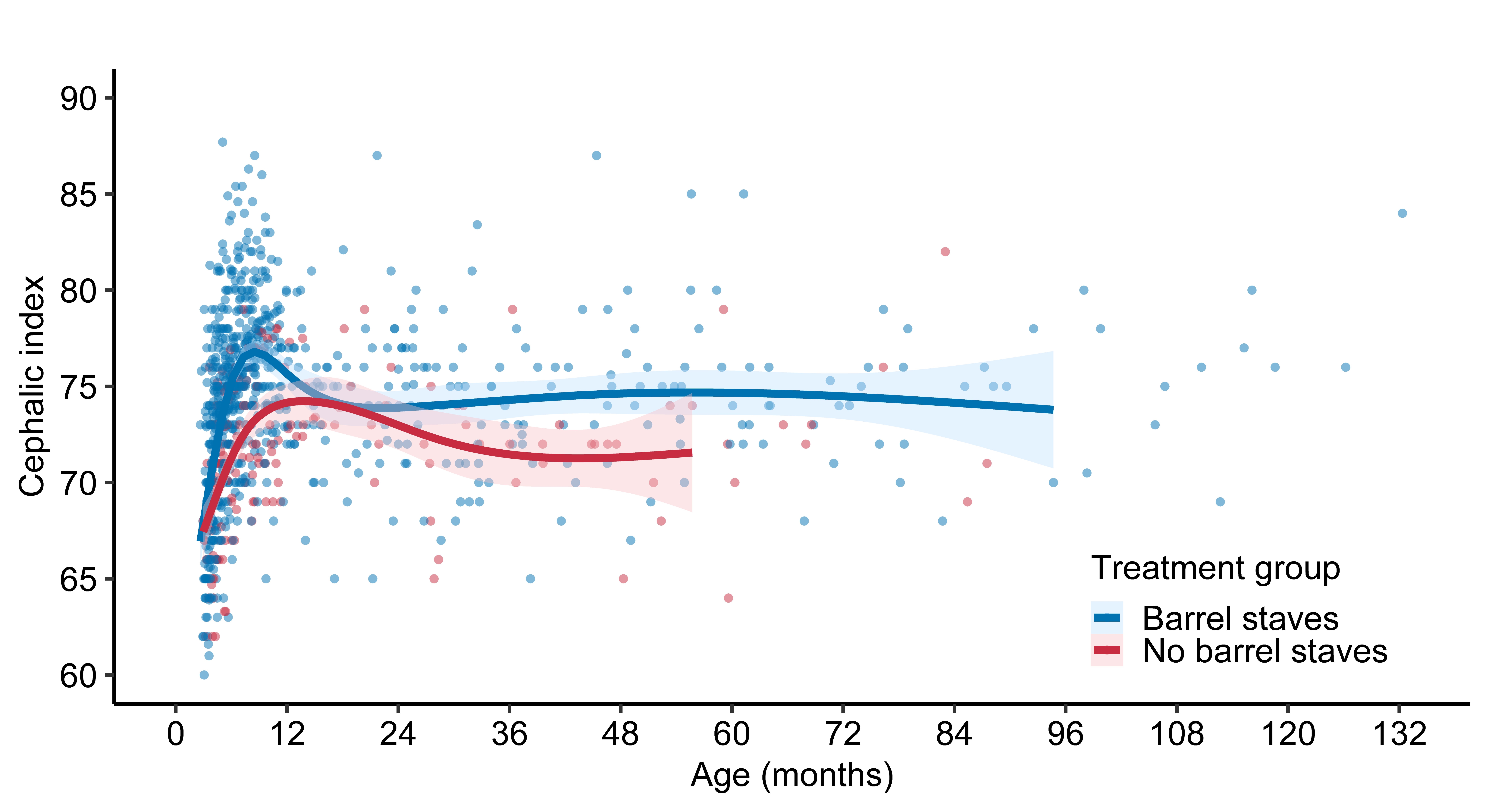
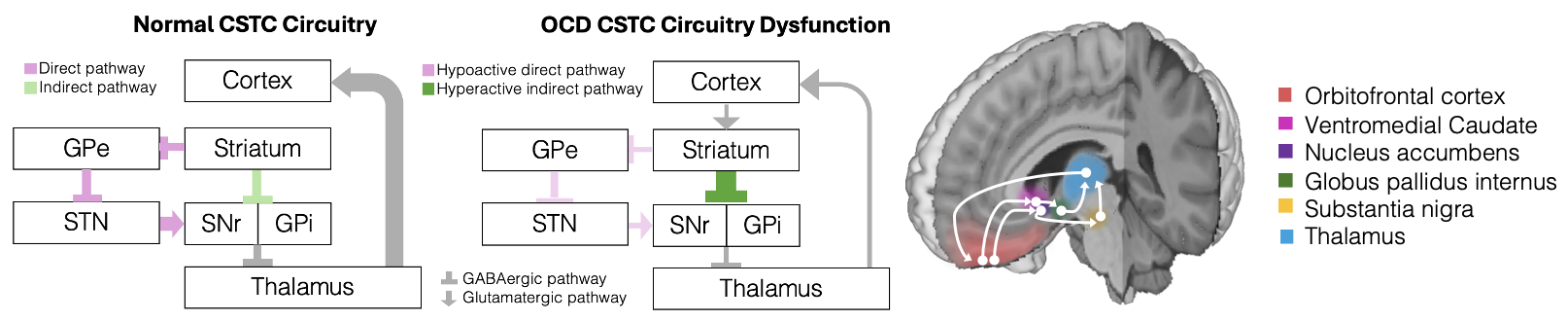
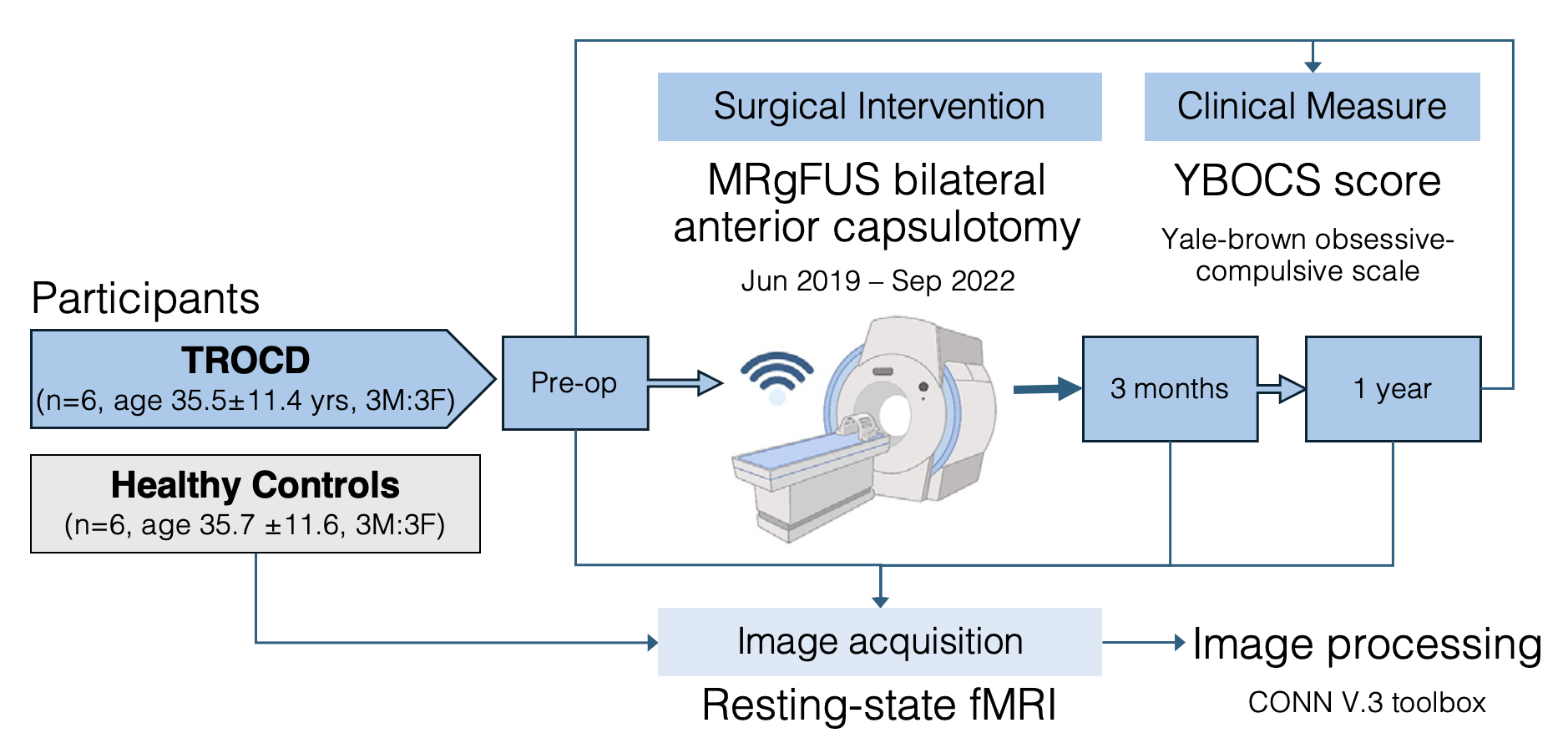
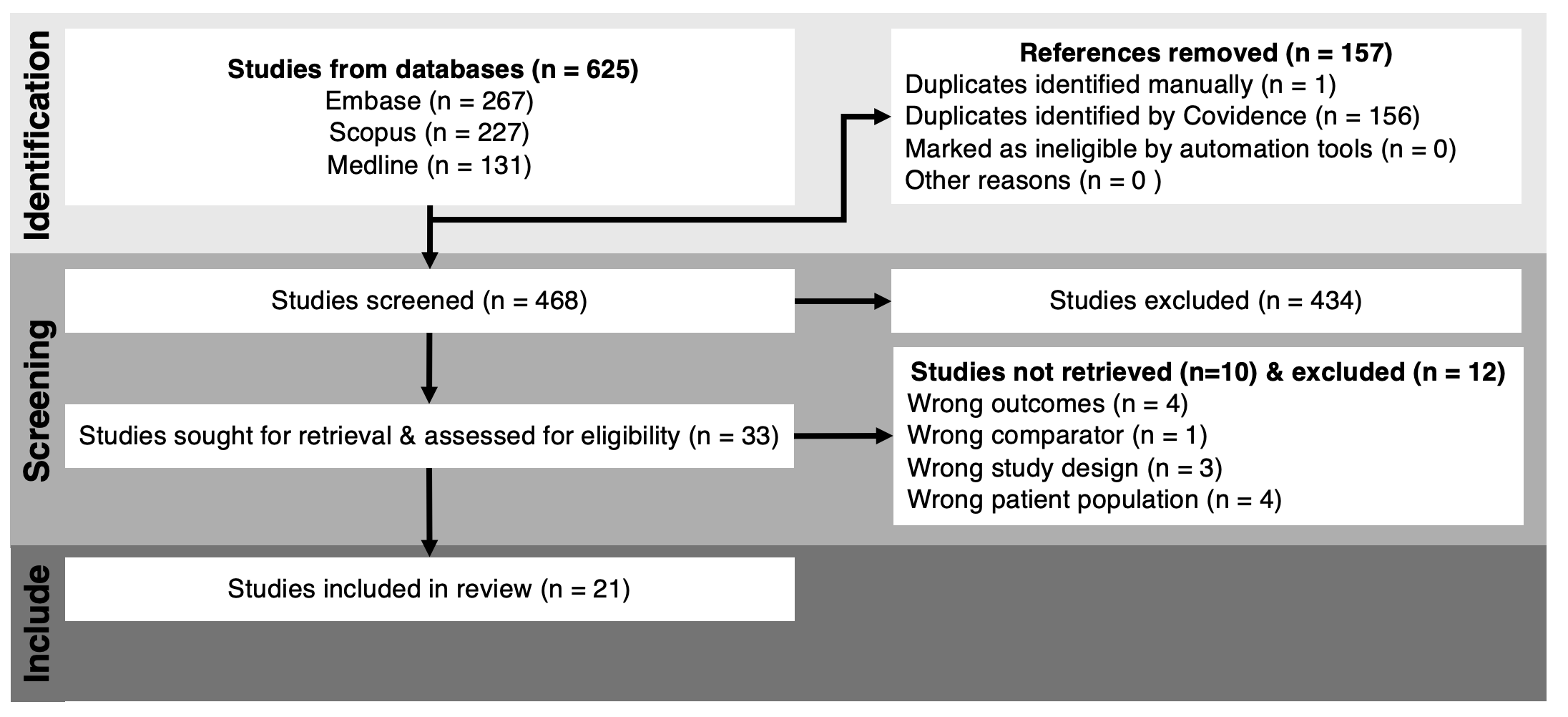
Our clinical outcomes in TROCD MRgFUS
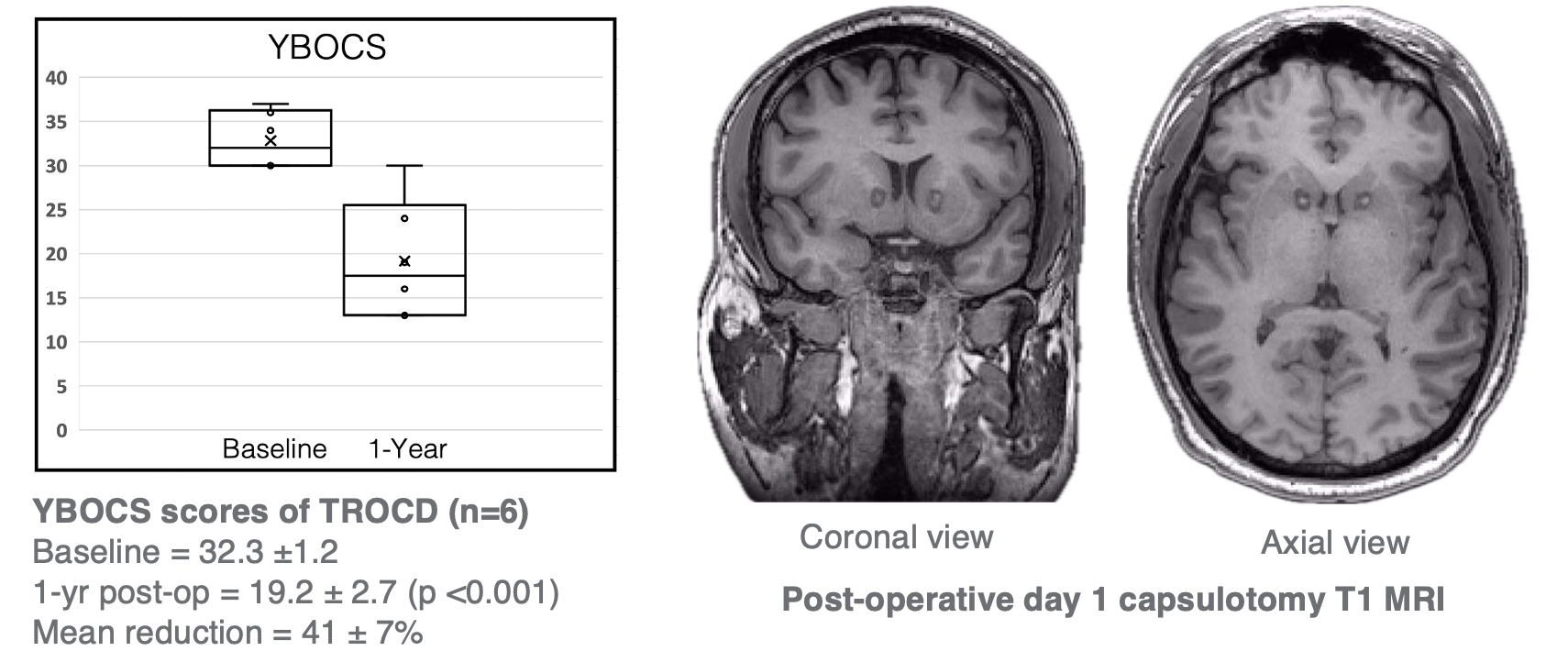
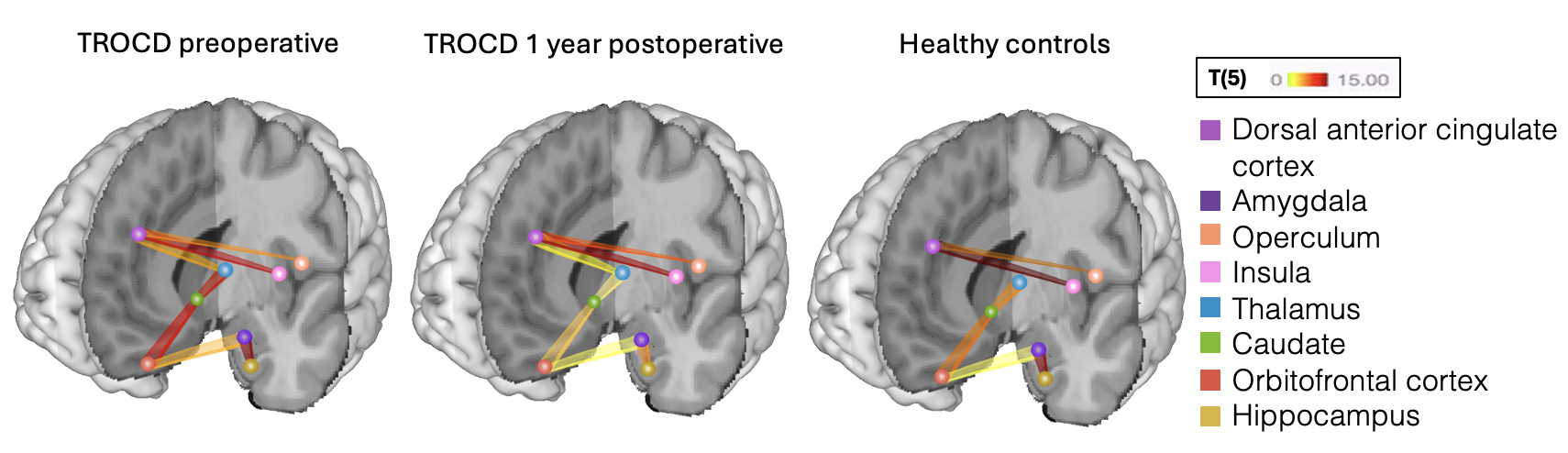
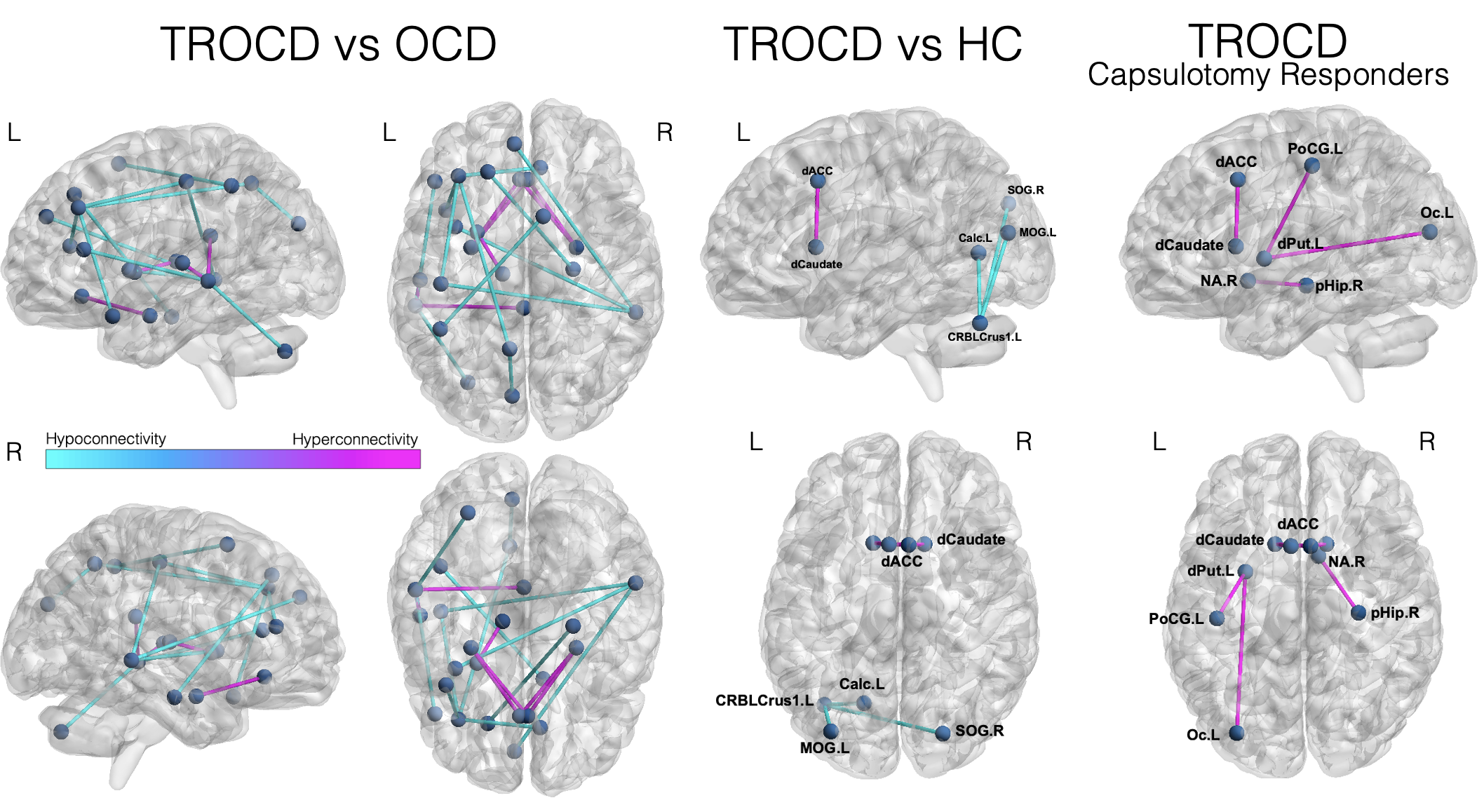
Arachnoid cysts - extra-axial cerebrospinal fluid collections within the arachnoid membrane.
Arachnoid cysts are usually asymptomatic .
Rupture may result in hemorrhage.
Ruptured arachnoid cysts with hemorrhage have been reported to be one of the main indications of surgical intervention.
Management of ruptured cysts is not well defined.
Aim - to develop a machine learning model to analyze factors affecting decision making.
Literature search for cases of ruptured arachnoid cysts with hemmorhage/hygroma (1975-2023)
Cleaning and preprocessing of the dataset in R statistical software. Dataset split into training and testing sets -> tree-augmented Naive Bayes (TAN) Classifiers were trained using the BNLEARN package to generate fitted Bayesian networks.
TAN classifiers were evaluated for accuracy and area under the curve (AUC).
A web application was developed to explore the networks.
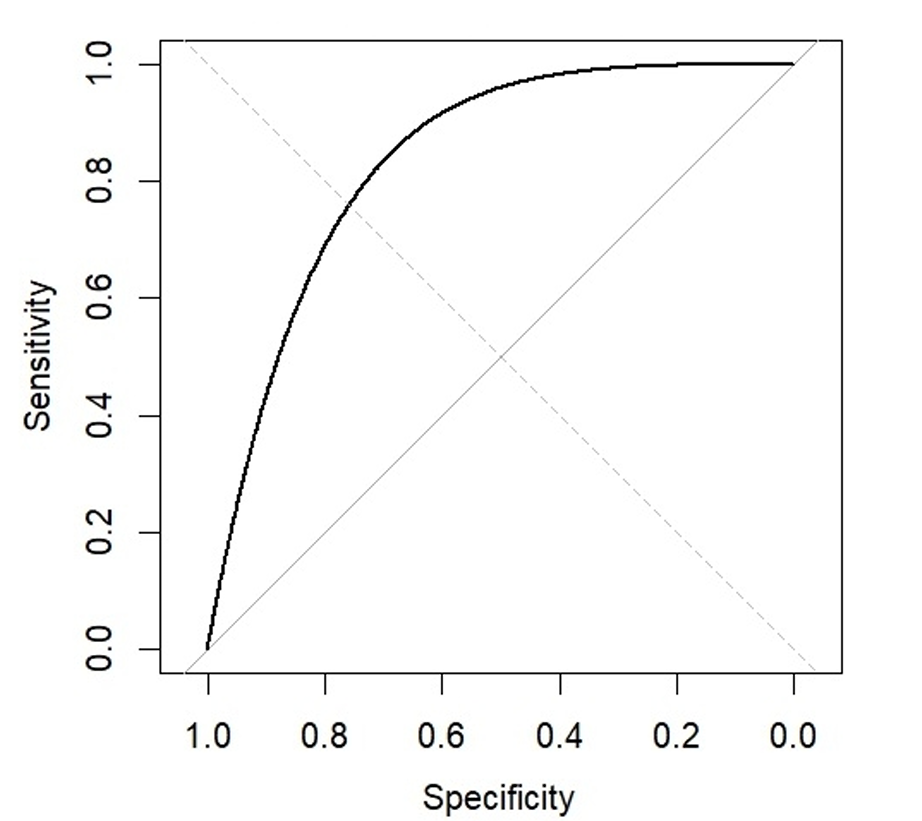
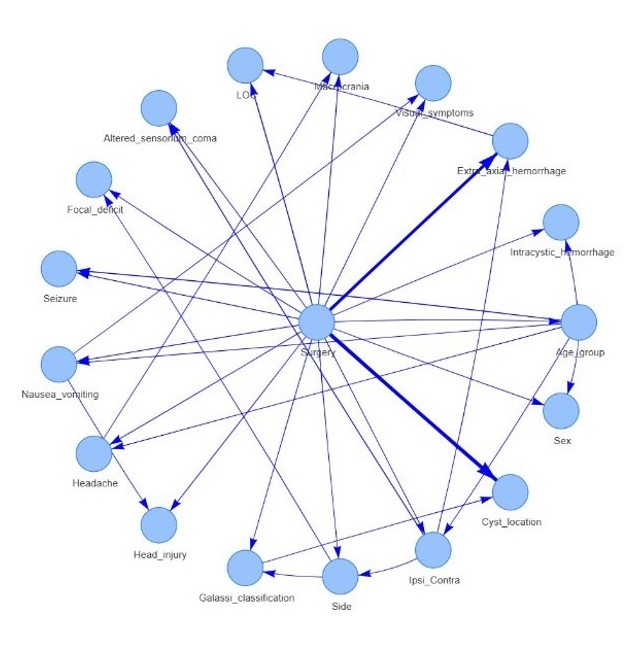
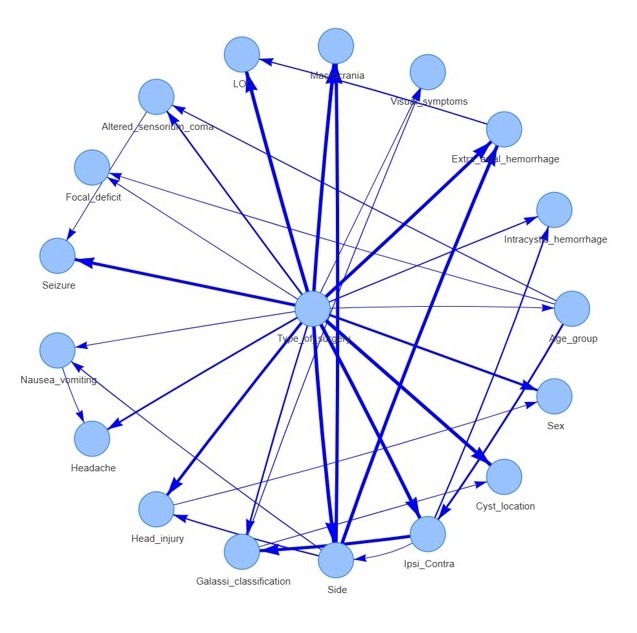
Fitted Bayesian network for predicting the probability of surgery had 18 nodes and 33 arcs.
Accuracy of 90.48%% when tested on the testing set
The Bayesian network fitted to predict the type of surgery had an overall accuracy of 75%.
Also deployed as a Shiny webapp for using the model with custom inputs.
Dataset is skewed towards surgery – attempted correction with generating balanced dataset.
Future directions include retraining model with artificially generated dataset.


Co-occurrence of normal pressure hydrocephalus (NPH) and neurodegenerative disorders such as progressive supranuclear palsy (PSP) complicates diagnosis due to overlapping and evolving features. We report an autopsy-confirmed case of PSP in a patient initially diagnosed with shunt-responsive NPH, without classic PSP signs antemortem. Despite disease progression, CSF diversion may offer meaningful, albeit time-limited, improvement in gait and quality of life.
Patient: 78-year-old female with a 4-year history of progressive gait dysfunction, cognitive decline, and urinary urgency.
Frequent falls, magnetic gait, declining IADLs
CT: Ventriculomegaly (Evans Index 0.38), acute callosal angle, no DESH
Intervention Timeline:
Large-volume lumbar puncture: Improved gait and alertness (Oct 2022)
Postoperative Course:
Progressive decline with new right-leg weakness
MRI: Stable; Shunt tap elicited clinical improvement
Autopsy: Neuropathology consistent with progressive supranuclear palsy (PSP)
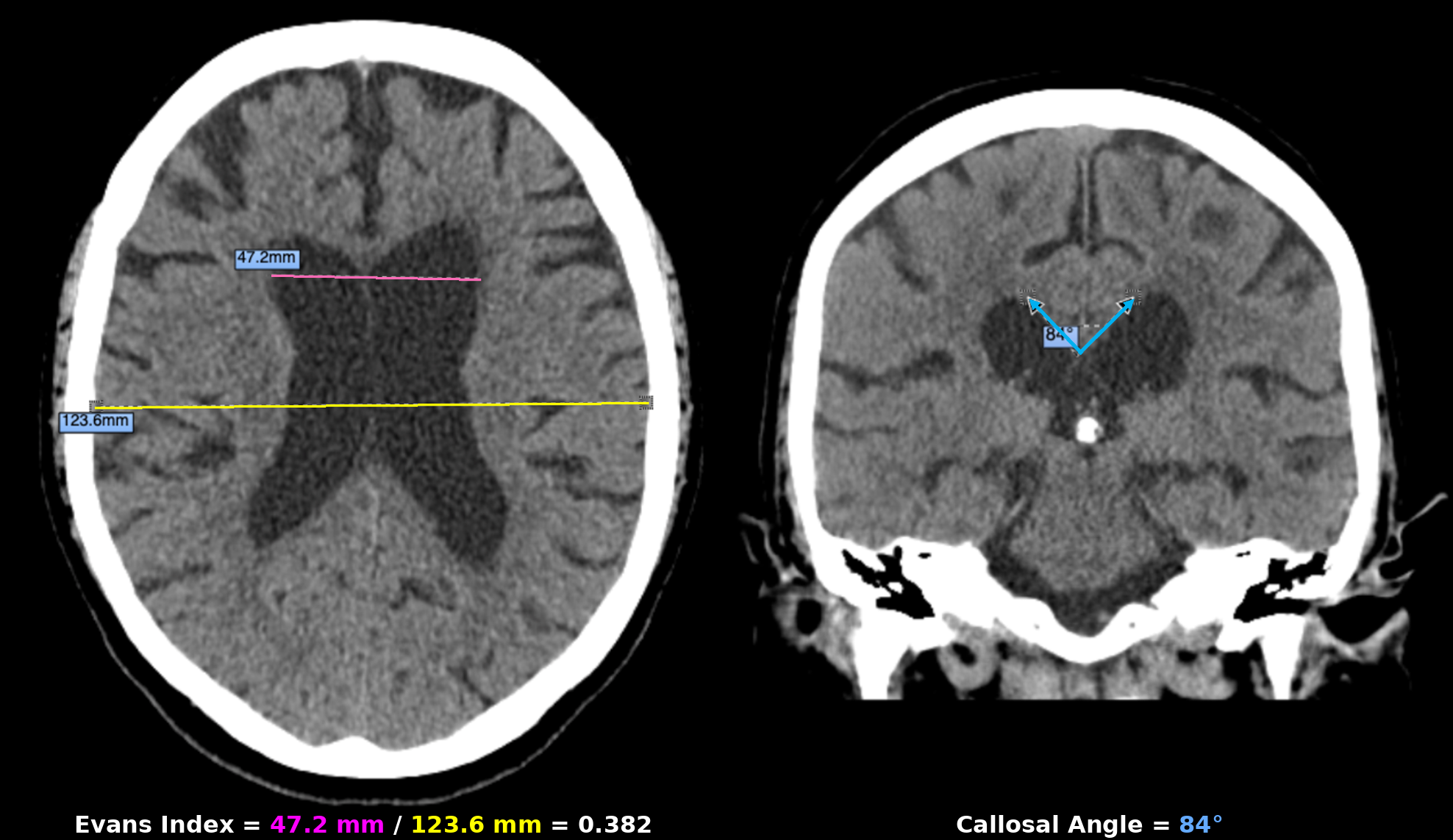
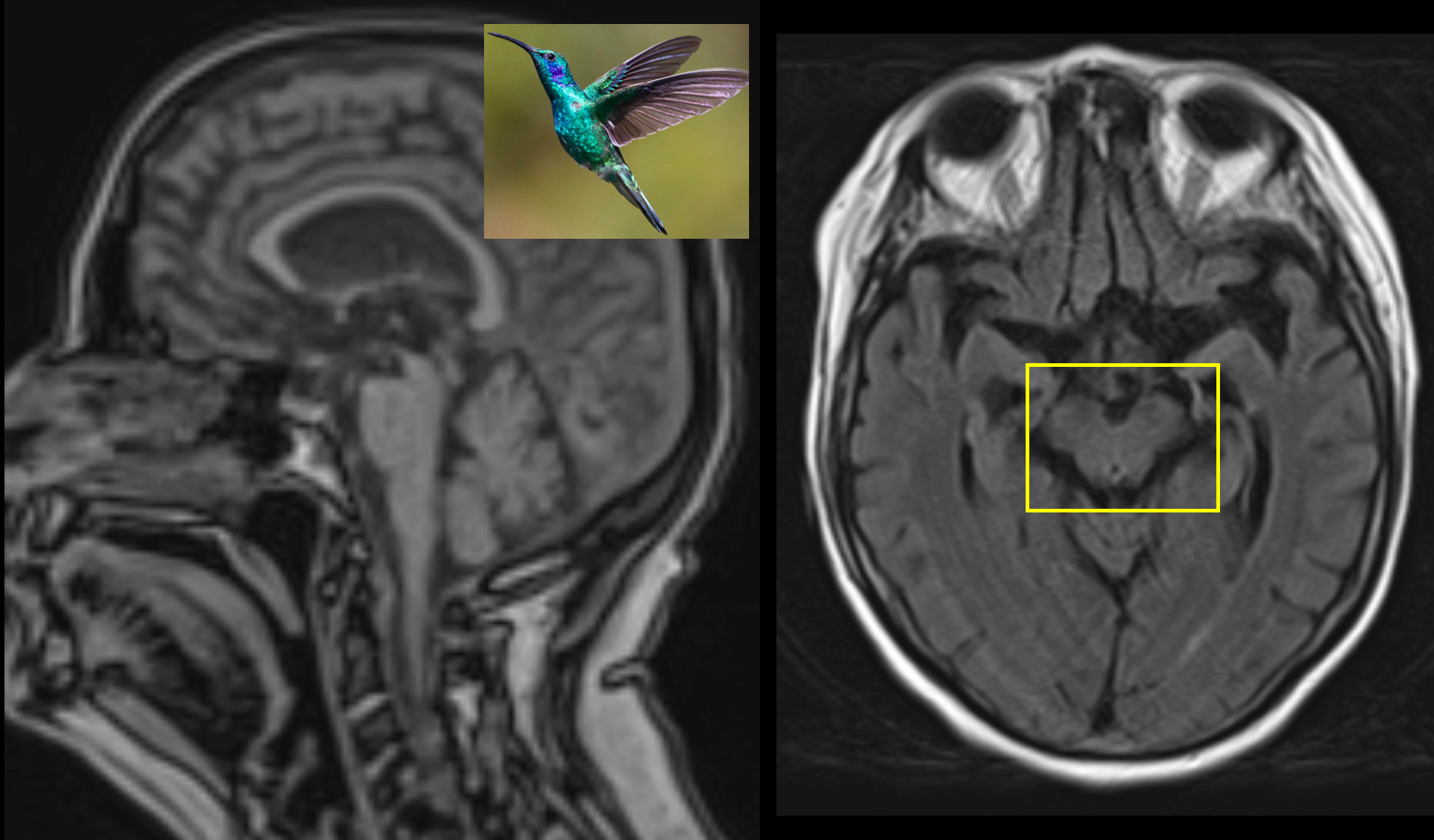
Figure 2. MRI shows “hummingbird” and “Mickey Mouse” signs of midbrain atrophy in PSP.
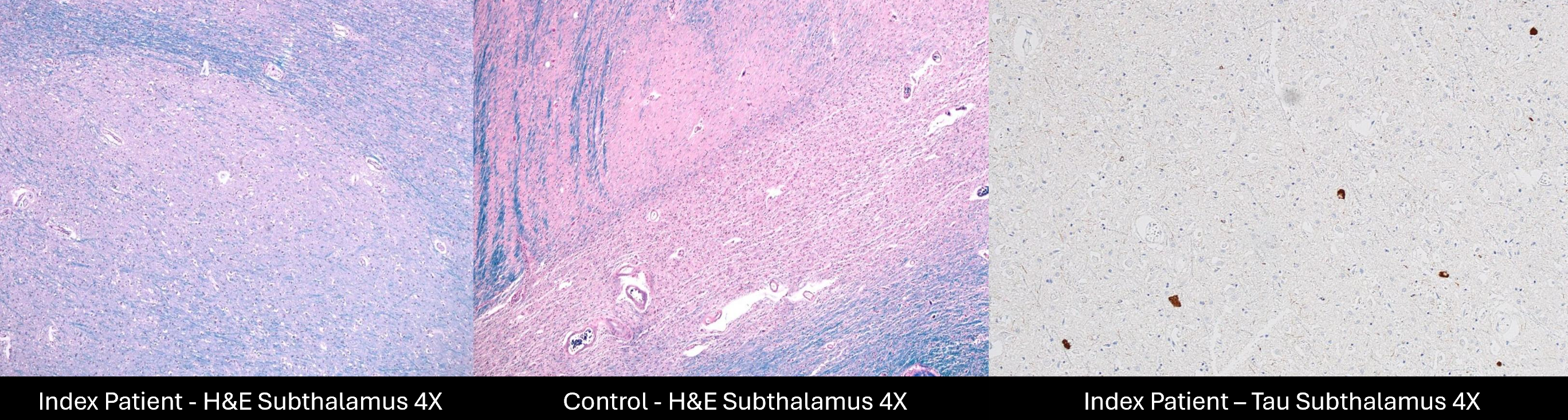
| Variable | Featured Case | Kawazoe 2023 | Kawazoe 2023 | Starr 2014 |
Magdalinou 2013 | Klassen 2011 | Schott 2007 |
Curran 1994 |
|---|---|---|---|---|---|---|---|---|
| Age/Sex | 78F | 70M | 79F | 72M | 66F | 82F | 68M | 69M |
| Sx Duration | 4 yr | 6 yr | 5 yr | 18 mo | 2 yr | 13 mo | 3 mo | — |
| Initial Clinical Features | ||||||||
| Gait | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ |
| Cognition | ✔️ | ✔️ | — | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ |
| Urinary | ✔️ | ✔️ | — | ✔️ | ✔️ | ✔️ | ❌ | ✔️ |
| Post-Shunt Improvement | ||||||||
| Gait | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ |
| Cognition | ✔️ | ✔️ | — | ❌ | ✔️ | ❌ | ✔️ | ✔️ |
| Urinary | ❌ | ✔️ | — | ✔️ | ❌ | ✔️ | ❌ | ✔️ |
| Resp. Time | 2 mo | few weeks | 1 mo | 6 mo | — | 10 mo | 1.5 yr | 6 mo |
| Late Ocular | ❌ | ❌ | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ | ✔️ |
| FU Duration | 10 mo | 2 yr | 5 yr | 6 yr | — | 6.2 yr | 4 yr | 5 yr |
Patients with overlapping NPH and PSP pose diagnostic and management challenges. Gait disturbance was universal, while cognitive and urinary symptoms varied. Most showed gait improvement after shunting, but other benefits were inconsistent. Response duration ranged from weeks to years. Delayed emergence of oculomotor signs, especially vertical gaze palsy, suggests unmasked PSP and underscores the need for long-term follow-up.
NPH and PSP often co-occur, complicating diagnosis. Given NPH’s treatability, CSF diversion may offer meaningful, if transient, benefit—even with evolving PSP. Ongoing neurologic monitoring is key as symptoms progress.

Retrospective 5-year review of NPH patients with CSF shunts. Post-shunt SDH cases were identified; clinical, imaging, and outcome data were analyzed.
The cohort included 34 patients (29 males, 5 females; mean age 74). Early SDH occurred in 18 patients (mean onset 48 days); 5 required surgery, while the remainder were managed with valve adjustment. All returned to baseline.
Late SDH occurred in 16 patients (mean onset 43 months). One required surgery; 13 were treated with valve adjustment, and 2 were observed. Three late SDH patients worsened functionally after shunt adjustment, despite radiographic improvement.
Early SDH was more likely to be symptomatic (Fisher's exact test, p=0.03) and require surgery (Tables 1–2). Shunt type and valve data are summarized in Tables 3–4. Valve setting drift occurred in 2 early and 4 late SDH cases and may have contributed to SDH development; the cause was not always identifiable.
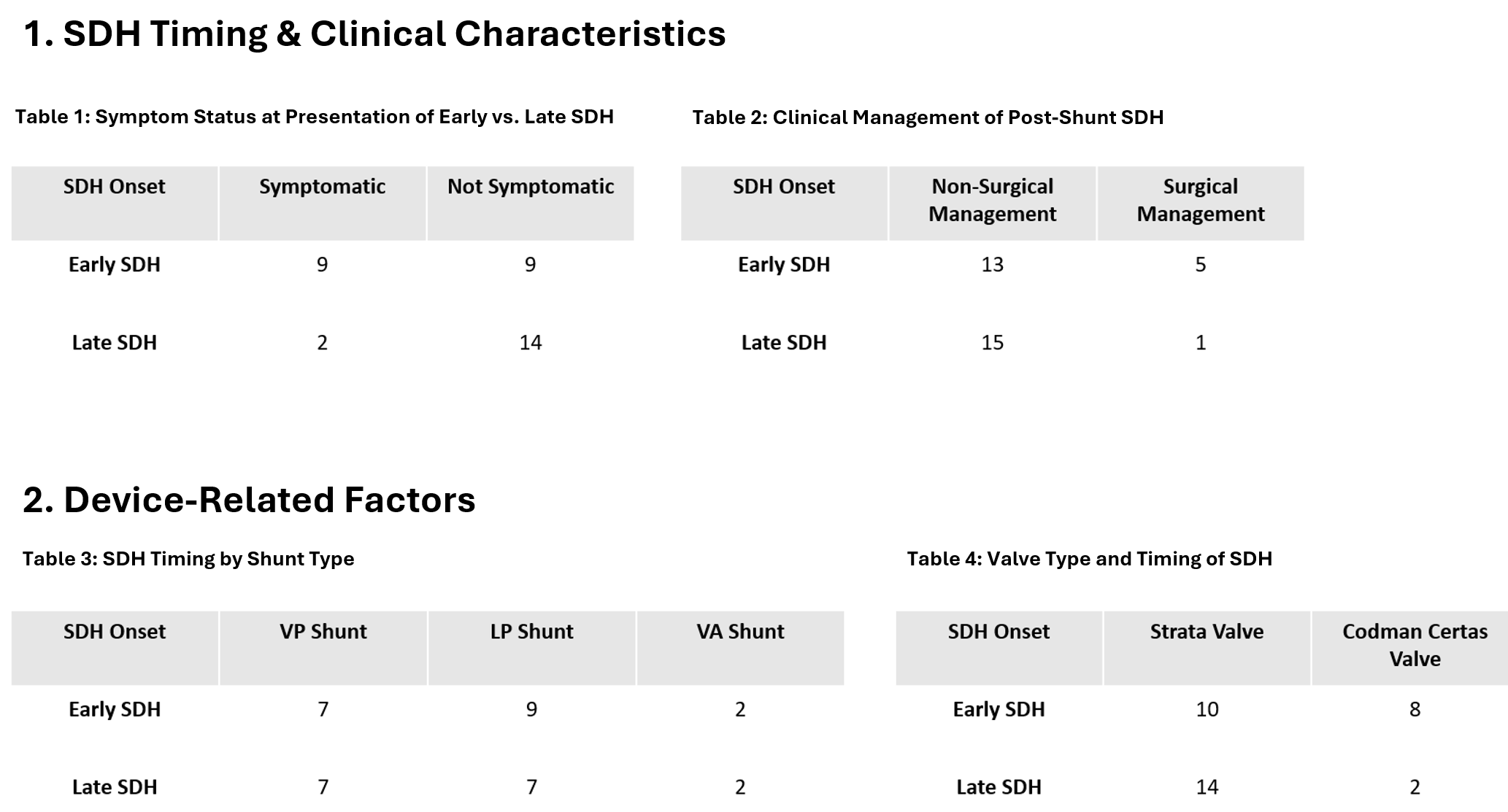
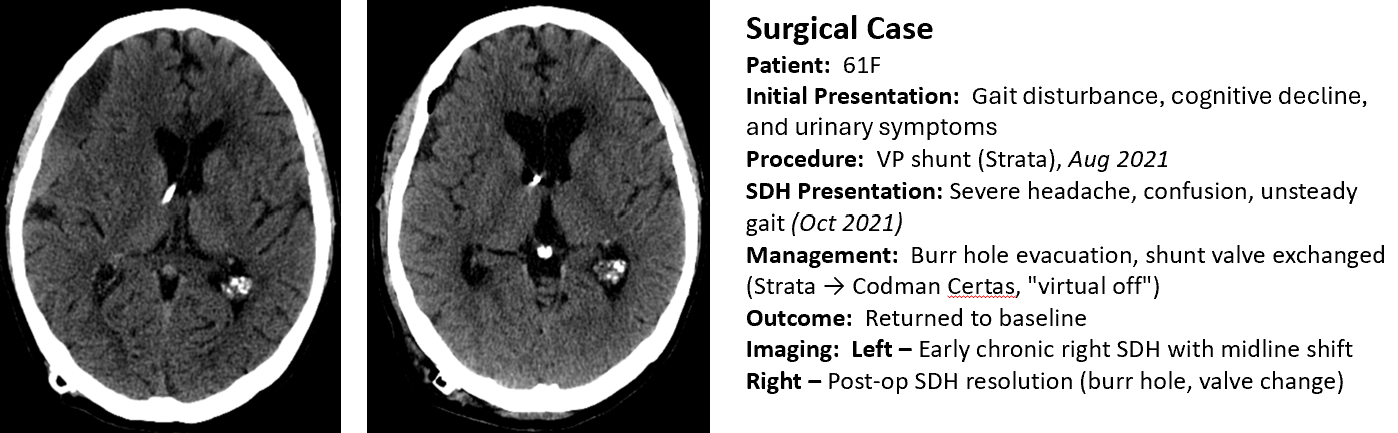
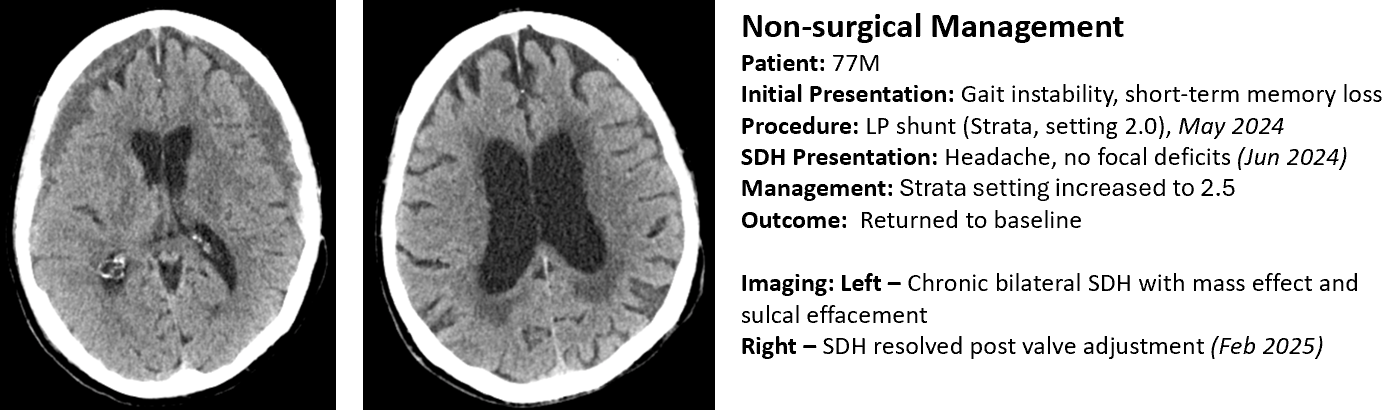
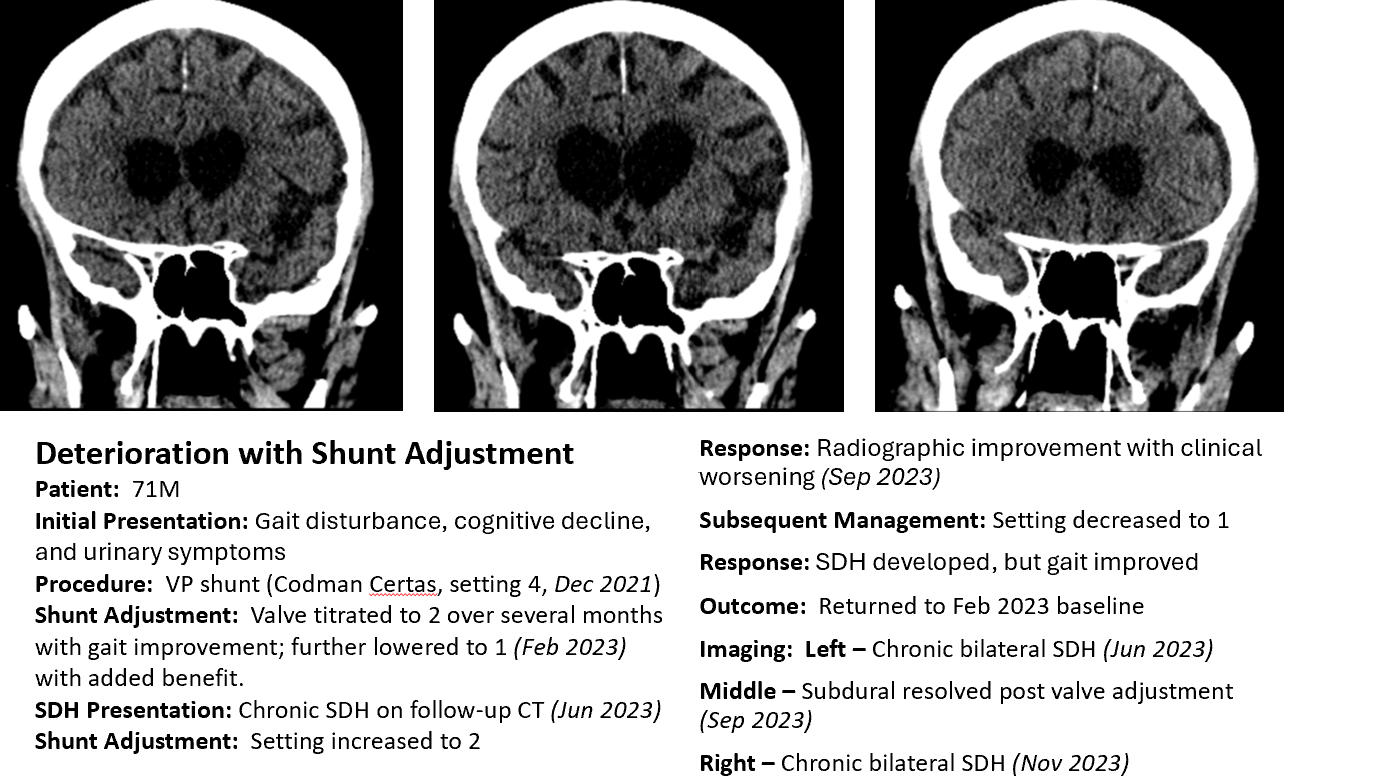
SDH remains a significant complication following shunt placement for NPH. This series underscores key differences between early (≤ 6 months) and late (˃ 6 months) SDH in both presentation and management. Early SDHs were more often symptomatic and surgically treated, whereas late SDHs were typically asymptomatic and managed conservatively.
Programmable valves appear to reduce the risk and severity of SDH. Delwel et al. observed higher SDH rates in patients initially set to low or medium valve pressures, compared to those started at higher settings with gradual reduction. In a registry of 1,846 patients, Sundström et al. reported that only 30% of SDH cases with programmable valves required surgery, compared to 90% among those with fixed-pressure systems.
In our cohort, 28% of early SDHs required surgical evacuation, frequently alongside valve adjustment. Late SDHs were more often managed by valve adjustment alone, though some patients experienced clinical deterioration despite radiographic resolution.
While programmable valves offer adaptability, their effective use depends on structured follow-up and access to specialized care for timely adjustment and monitoring.
This study highlights key differences in the presentation and management of SDH following shunt placement for NPH. Early SDH (≤ 6 months) was more likely to be symptomatic and surgically treated, whereas late SDH (> 6 months) was typically asymptomatic and managed conservatively. Shunt type did not appear to influence SDH timing. These findings reinforce the need for vigilant postoperative follow-up, particularly in the early weeks after shunting.

Degenerative Cervical Myelopathy (DCM) refers to progressive cervical spinal cord injury caused by degenerative conditions. The AO Spine RECODE-DCM – gathering initiative emphasized the importance of research on the relationship between pain severity and postoperative functional and neurological outcomes to enhance DCM care.
This meta-analysis examines the relationship between pain scores and quality of life outcomes in surgical DCM patients. This will aid the development of clinical guidelines that are cognizant of metabolic
A comprehensive literature search using MEDLINE, Web of Science, and Embase identified 73 studies for data extraction. Two independent reviewers screened studies, and meta-regression assessed the association between visual analogue scale (VAS) pain scores and quality of life outcomes, including the 12-item and 36-item Short Form Surveys (SF-12, SF-36). Findings are expected to clarify pain’s role in surgical decision-making and inform clinical guidelines.
Summary Statistics A meta-regression analysis was performed on the dataset gathered from 73 studies in total, following the full-text screening process.
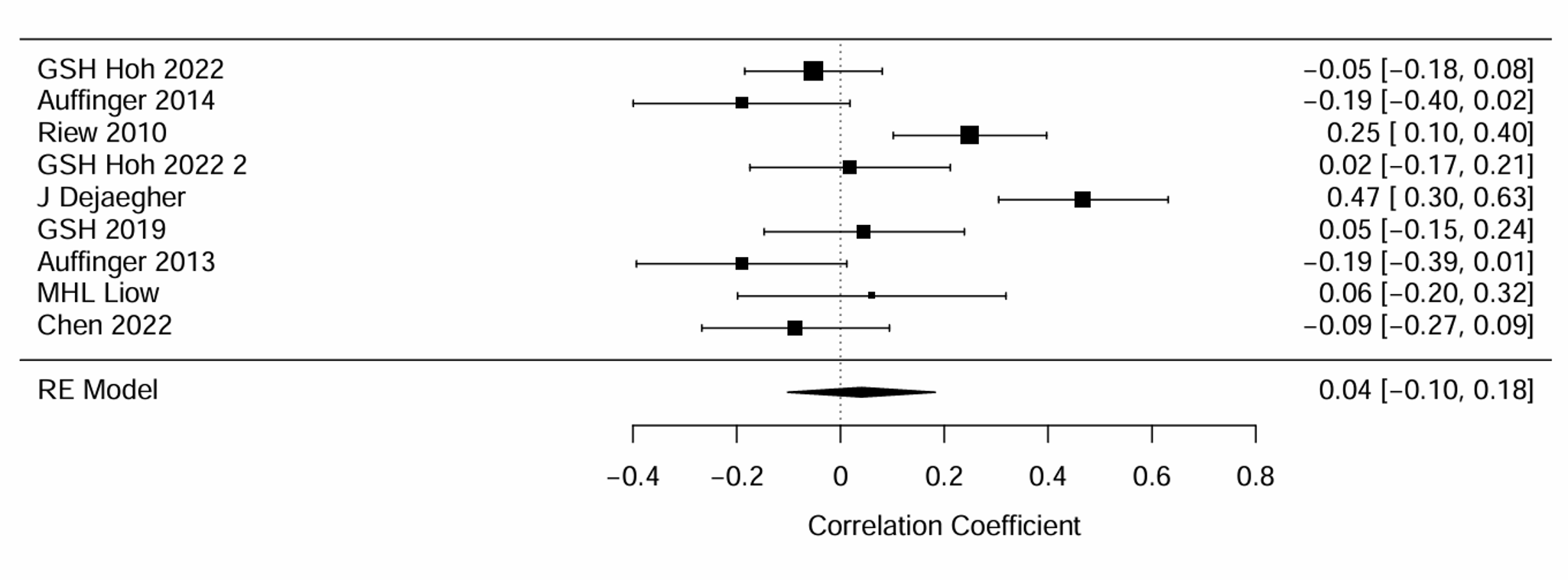
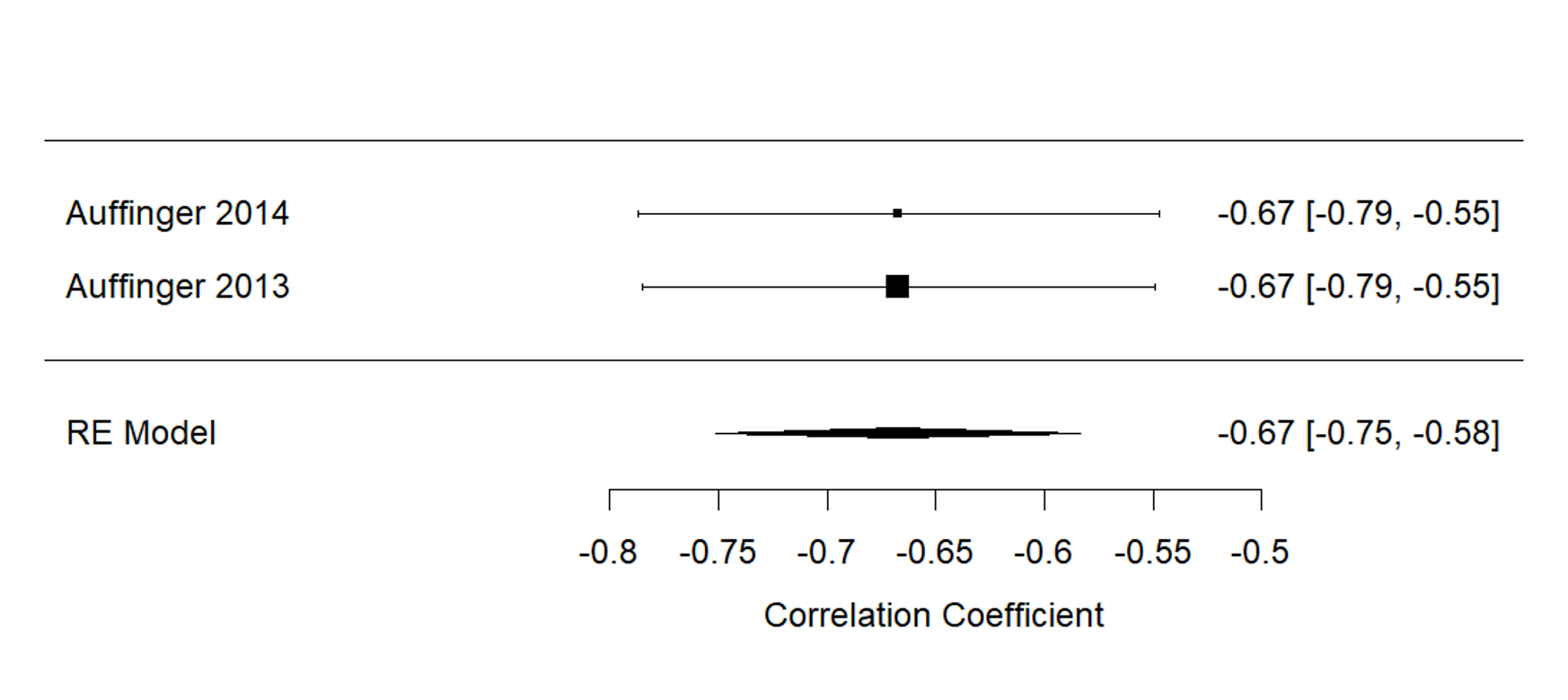
Fig 1. A: Forest-plot diagram of pain and SF-36 values at baseline. B: Forest-plot diagram of pain and SF-36 at 3 months
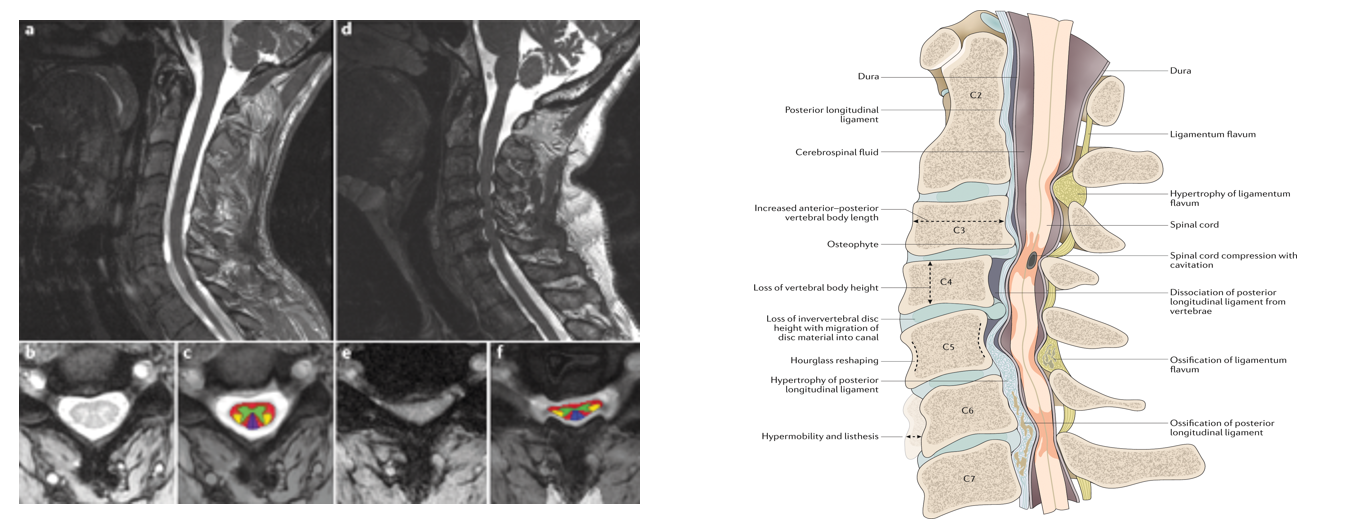
Fig 2. Magnetic resonance imaging (MRI) and anatomic diagram of patients with DCM, demonstrating compression of the cervical spinal cord.
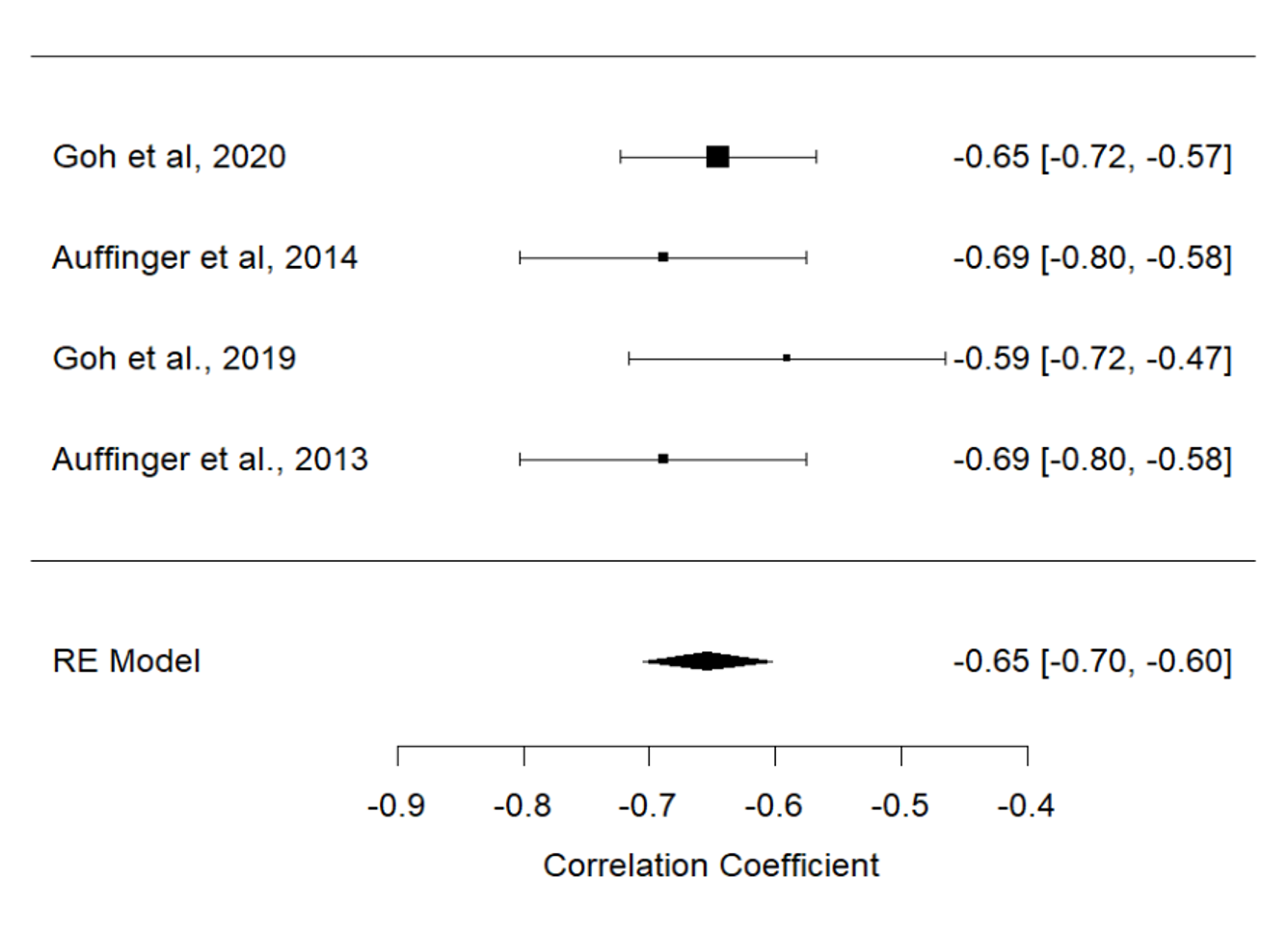
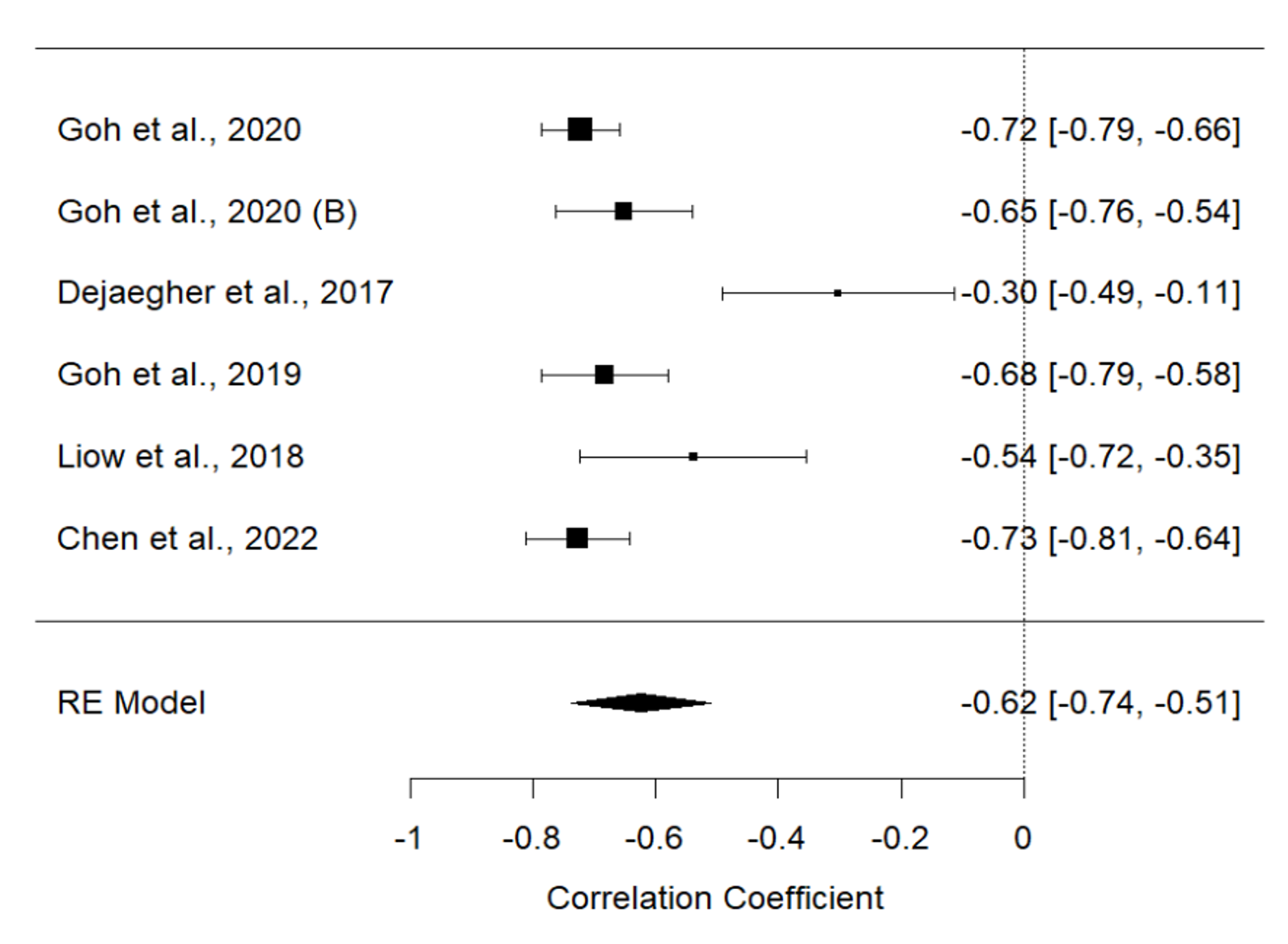
Fig 3. C: Forest-plot diagram of pain and SF-36 values at baseline. D: Forest-plot diagram of pain and SF-36 at 3 months
Our results indicate a strong relationship between postoperative pain and QOL among patients with DCM.
Surgeons and care teams should prioritize optimal pain management postoperatively for patients with DCM.

Literature suggests that between 1.1%-17% of spine surgery patients will experience a dural tear (DT) during surgery. DTs are relatively common spine surgery complications that can increase a patient's risk of cerebrospinal fluid leaks and adverse events. Given the prevalence of DTs and their potential impact, cases of elective spine surgery in Saint John were examined to determine risk factors and identify adverse event rates.
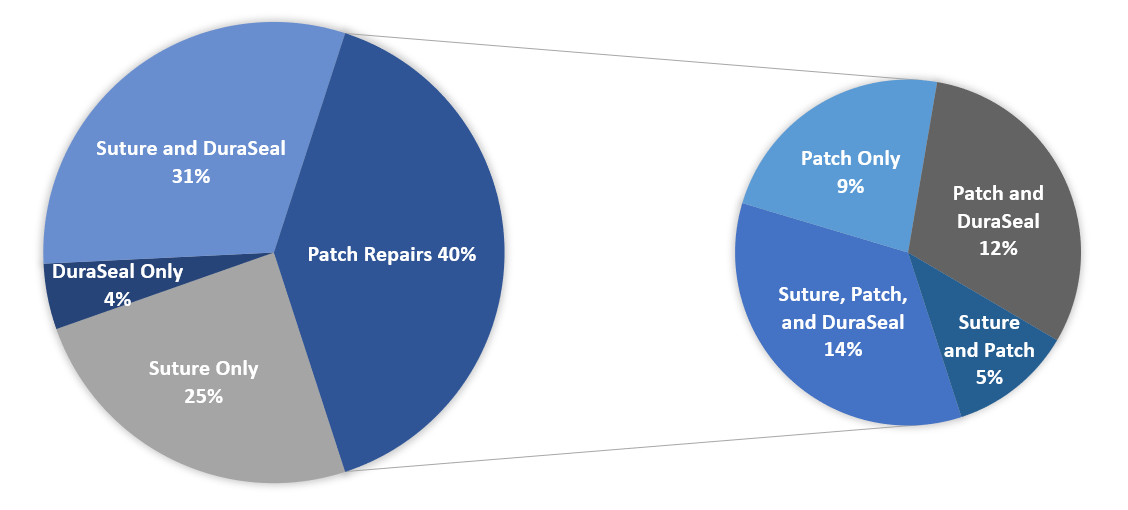
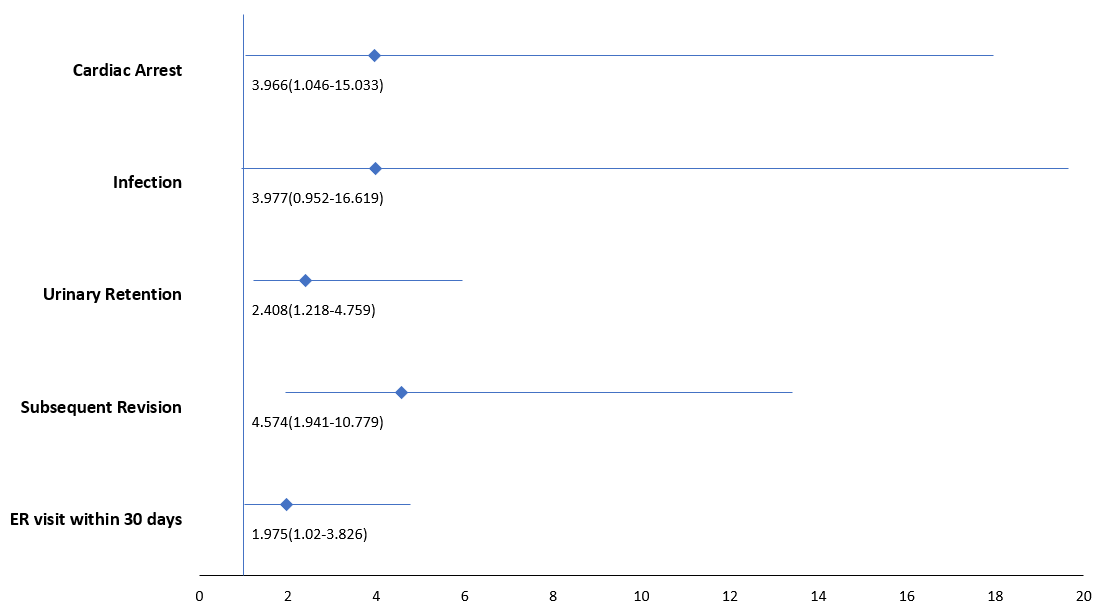

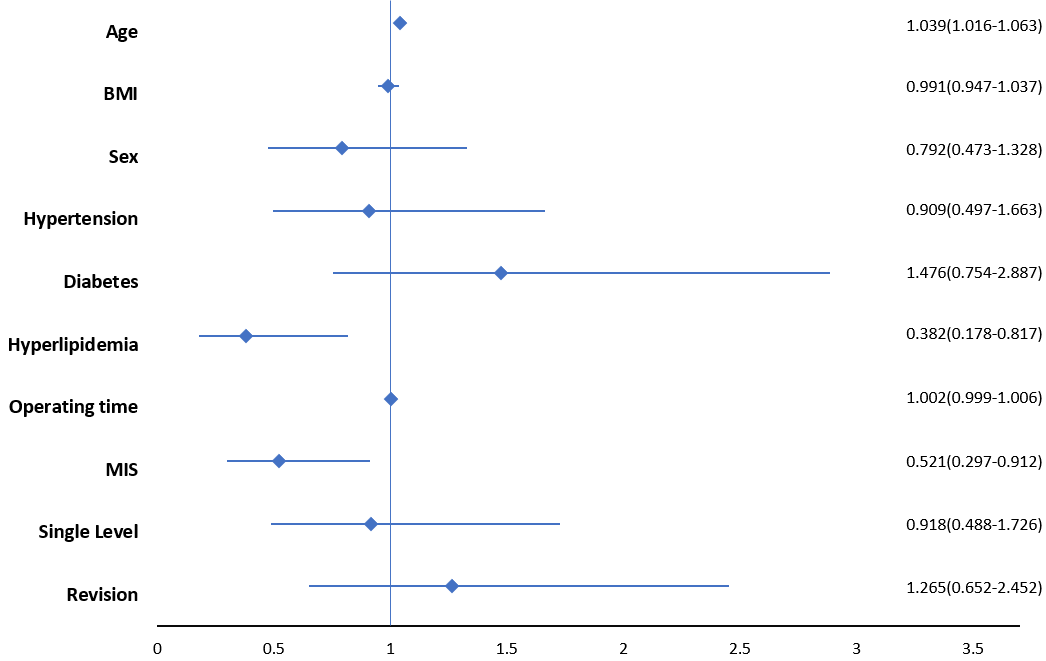

Surgical robotics can minimize the discrepancy between surgical preoperative plan and postoperative execution. This work explores the performance of a supervisory-control architecture robot for autonomous pedicle instrumentation in both an open and MIS workflow, as well as guidance accuracy assessment in living patients undergoing spinal fusion.
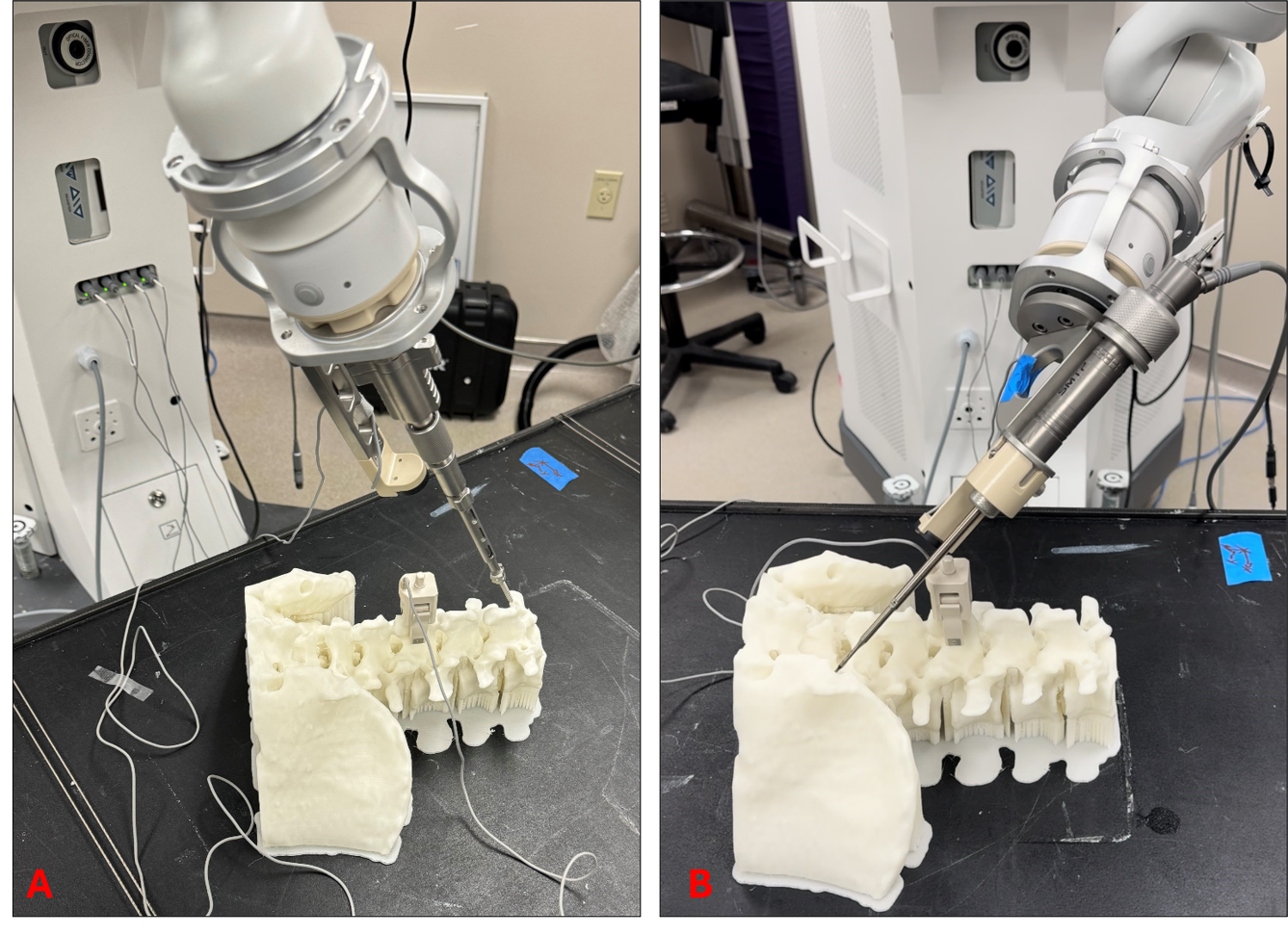
A total of 10 porcine subjects were implanted. 6 utilized open surgical technique and 4 minimally invasive percutaneous insertion. Animals were observed for 24 hours to ensure no neurological deficitis. Post operative CT scan was obtained for all animals. All 10 porcine subjects had Gertzbein Robin grading scale completed. Detailed quantitative assessment was conducted in 3 porcine subjects who underwent open pedicle instrumentation with a customized image processing pipeline. Euclidean error was calculated at screw head and screw tip. All points were normalized to a nominal screw, and confidence ellipses generated.
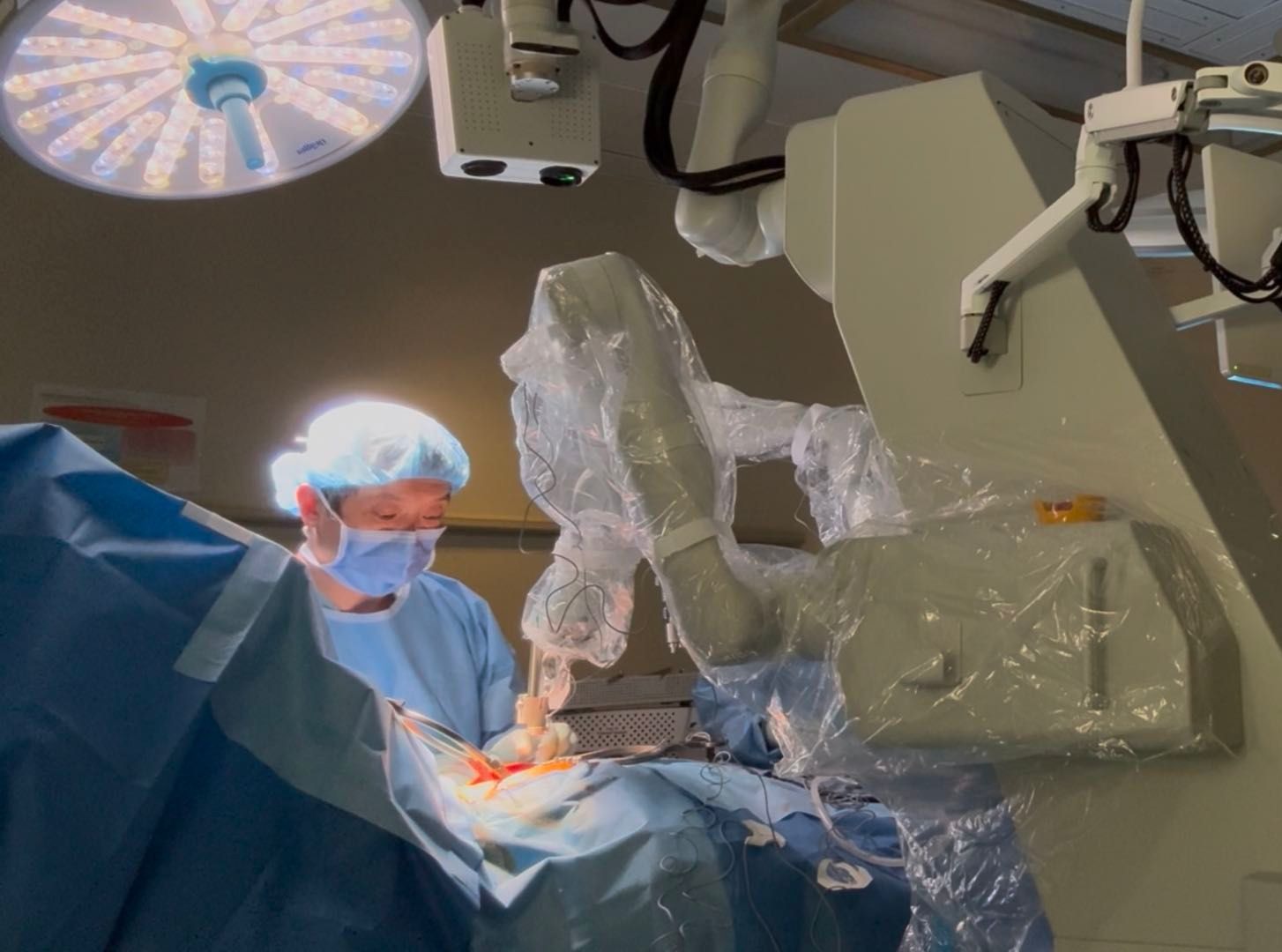
All animals were neurologically intact at 24 hours. 78/78 (100%) of screws were clinically acceptable GRS A+B with 72/76 (92%) GRS A . There was no clinical difference between MIS vs Open workflow. Mean tip and head Euclidean error where 2.47+/-1.25mm and 2.25+/-1.25mm respectively. Major and minor axes of the confidence ellipse at 99% was 2.19mm, and 1.28mm, and 2.07mm, and 0.42mm for tip and head respectively. Guidance was successfully obtained in human cases, with good agreement with standard of care image guidance.
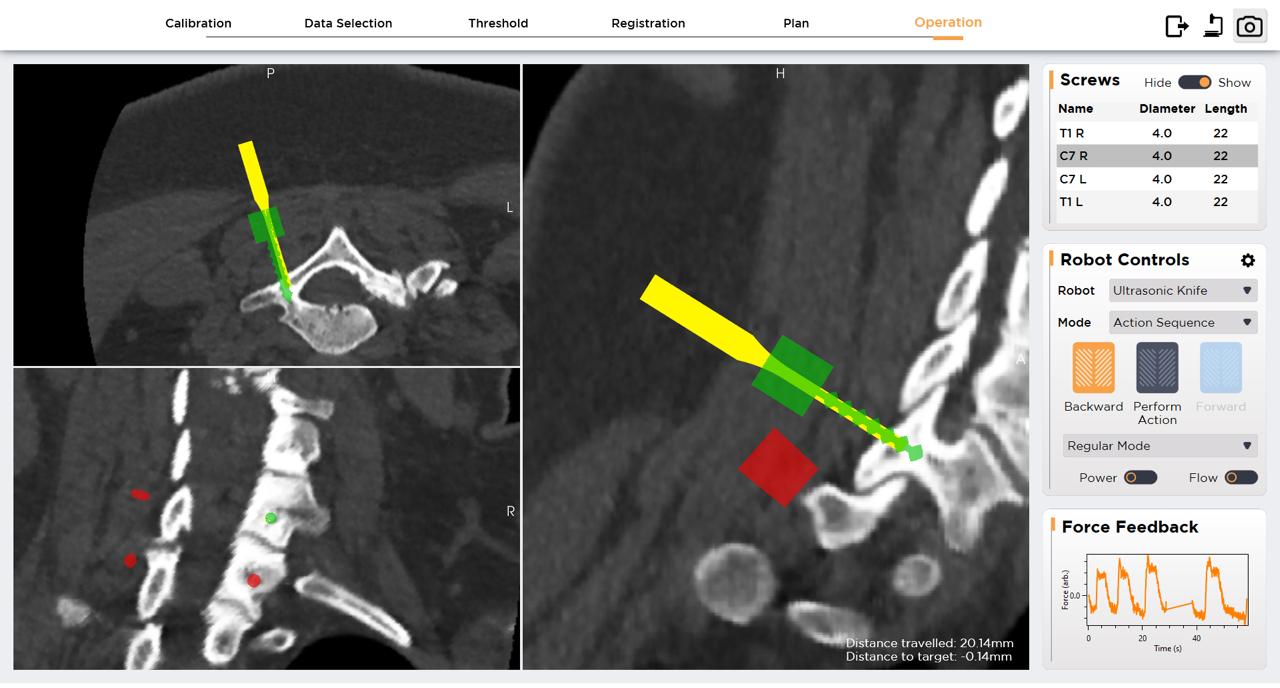
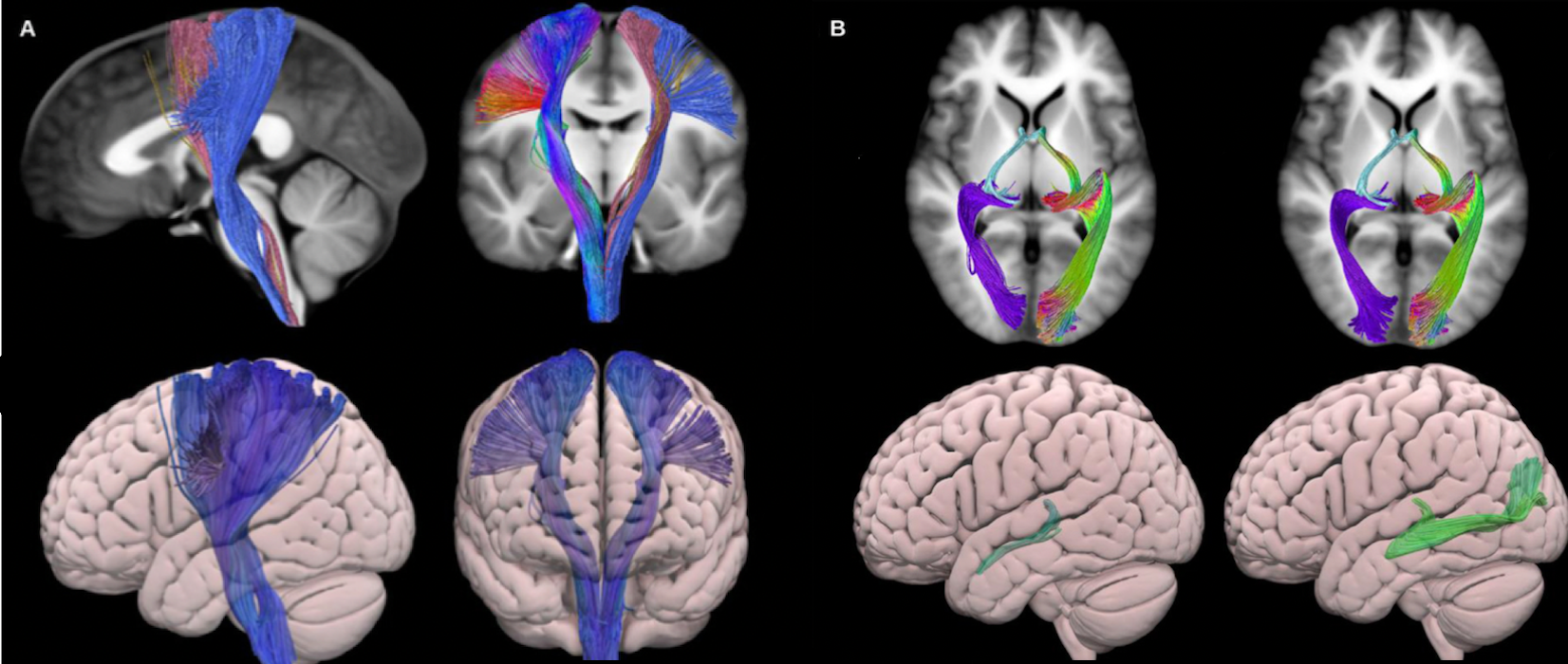
Table 1. Qualitative comparison of software platform characteristics between Synaptive’s Modus PlanTM and Medtronic’s StealthVizTM.
| Characteristic | Synaptive’s Modus PlanTM | Medtronic’s StealthVizTM |
|
Ease of use |
+++ |
- - - |
|
DTI technical expertise required |
- - - |
+++ |
|
Degree of clinician input |
+ |
- - - |
|
Industry representative supervision |
+++ |
- - - |
|
Program stability |
+++ |
- - - |
|
3D object export |
- |
+ |
|
Embedded DICOM export |
+ |
- |
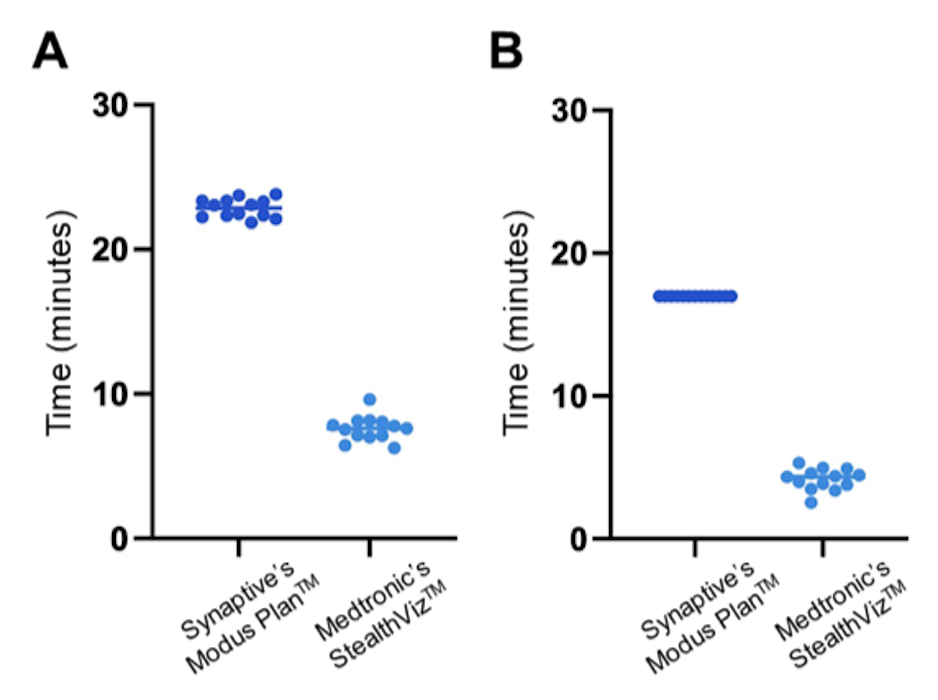
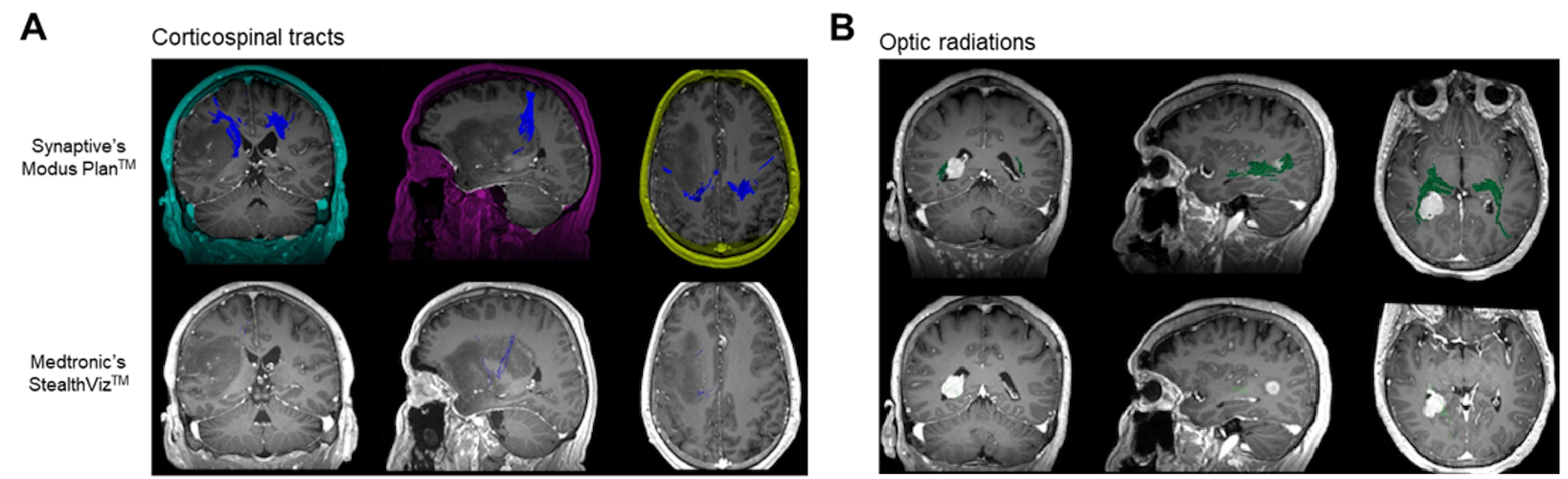
1. Fields RD. Neuroscience. Change in the brain’s white matter. Science. 2010;330(6005):768-769. doi:10.1126/science.1199139
2. Nandu H, Wen PY, Huang RY. Imaging in neuro-oncology. Ther Adv Neurol Disord. 2018;11:1756286418759865. doi:10.1177/1756286418759865
3. Xiao X, Kong L, Pan C, et al. The role of diffusion tensor imaging and tractography in the surgical management of brainstem gliomas. Neurosurg Focus FOC. 2021;50(1):E10-. doi:10.3171/2020.10.FOCUS20166
4. Feigl GC, Hiergeist W, Fellner C, et al. Magnetic resonance imaging diffusion tensor tractography: evaluation of anatomic accuracy of different fiber tracking software packages. World Neurosurg. 2014;81(1):144-150. doi:10.1016/j.wneu.2013.01.004
5. Radwan AM, Sunaert S, Schilling K, et al. An atlas of white matter anatomy, its variability, and reproducibility based on constrained spherical deconvolution of diffusion MRI. Neuroimage. 2022;254:119029. doi:10.1016/j.neuroimage.2022.119029